")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Poor mental health status and aggression are associated with poor driving behavior among male traffic offenders
Authors Abdoli N, Farnia V, Delavar A, Esmaeili A, Dortaj F, Farrokhi N, Karami M, Shakeri J, Holsboer-Trachsler E, Brand S
Received 19 May 2015
Accepted for publication 18 June 2015
Published 11 August 2015 Volume 2015:11 Pages 2071—2078
DOI https://doi.org/10.2147/NDT.S88835
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Nasrin Abdoli,1,2 Vahid Farnia,3 Ali Delavar,4 Alirez Esmaeili,5 Fariborz Dortaj,4 Noorali Farrokhi,4 Majid Karami,6 Jalal Shakeri,3 Edith Holsboer-Trachsler,7 Serge Brand7,8
1International University of Imam Reza, Mashhad, 2Kermanshah University of Medical Sciences, Kermanshah, 3Substance Abuse Prevention Research Center, Psychiatry Department, Kermanshah University of Medical Sciences, Kermanshah, 4Allameh Tabataba’i University, Tehran, 5Police University, Tehran, 6Baharestan Research Center, Kermanshah Transportation Terminal, Kermanshah, Iran, 7Center for Affective, Stress and Sleep Disorders, Psychiatric Clinics of the University of Basel, Basel, 8Department of Sport and Health Science, Sport Science Section, University of Basel, Basel, Switzerland
Background: In Iran, traffic accidents and deaths from traffic accidents are among the highest in the world, and generally driver behavior rather than either technical failures or environmental conditions are responsible for traffic accidents. In the present study, we explored the extent to which aggressive traits, health status, and sociodemographic variables explain driving behavior among Iranian male traffic offenders.
Method: A total of 443 male driving offenders (mean age: M =31.40 years, standard deviation =9.56) from Kermanshah (Iran) took part in the study. Participants completed a questionnaire booklet covering sociodemographic variables, traits of aggression, health status, and driving behavior.
Results: Poor health status, such as symptoms of depression, anxiety, insomnia, and social dysfunction, and also higher levels of trait aggression explained poor driving behavior. Multiple regressions indicated that poor health status, but not aggression, independently predicted poor driving behavior.
Conclusion: Results suggest that health status concerns are associated with poor driving behavior. Prevention and intervention might therefore focus on drivers reporting poor mental health status.
Keywords: insomnia, depression, anxiety aggression, health status, male traffic offenders
Introduction
In Iran, the most widely used forms of transportation are not airplanes, trains, or metros, but cars, motorcycles, buses, and trucks. Compared to Western countries (North America and Europe), the traffic-related prevalence of mortality is higher in Iran.1,2 Indeed, whereas the World Health Organization2 reported 24.1 traffic death of 100,000 people per annum in Iran, the prevalence rate is dramatically lower for instance in Switzerland (3.4), Germany (4.3), or in the USA (11.6). Traffic accidents are the main cause of injuries requiring surgical intervention,3 and the second largest cause of mortality in Iran.4,5
Further, worldwide it has been estimated that 90%–95% of road crashes are due to human actions, namely, the behavior of drivers, and not to technical malfunctions,6 making it therefore more important to focus on the determinants of driver behavior to explain traffic accidents.
Recently, several studies have examined possible associations between personality traits and driving behavior.7–9 Hilton et al10 showed among a sample of 1,324 heavy goods vehicle drivers that severe and very severe self-reported symptoms of depression were associated with the increased risk of being involved in an accident. To explain this association, Hilton et al10 supposed that not symptoms of depression per sé, but the lack of concentration and poor sleep might have an unfavorable impact on driving behavior. Likewise, Scott-Parker et al11 showed that among novice drivers, symptoms of depression predicted risky behavior, while in a further analysis, Scott-Parker et al12 reported that not symptoms of depression, but anxiety predicted risky driving among female, but not male novice drivers. From these studies, we learn that risky driving behavior seemed to be associated with symptoms of depression10,11 and anxiety12 among professional drivers and novice drivers.11,12 Next, Pourabdian and Azmoon13 were able to show that among 168 Iranian drivers causally involved in traffic accidents poor driving behavior was significantly related to higher trait anxiety scores. Pourabdian and Azmoon13 offered the following as a possible explanation of this association: cognitive–emotional states such as trait anxiety increase the load on working memory and concentration. In effect, cognitive–emotional states such as trait anxiety take up resources otherwise needed to drive safely and avoid lapses and errors. However, correlations between trait anxiety and lapses and errors were low (rs 0.21–0.23), as were those between trait anxiety and aggressive reactions (rs from 0.15 to 0.17; note that the terminology used in the Manchester Driving Behavior Questionnaire [DBQ14] for aggressive reactions is “Aggressive violations” and “Ordinary violations”). Although Pourabdian and Azmoon13 were not in a position to test their explanation, to our knowledge they are the first to propose a causal role for cognitive–emotional processes in traffic accidents. Indeed, research on the association between cognitive performance and cognitive–emotional load was already observed in other fields: findings from neuropsychological testing of patients suffering from psychiatric disorders such as anxiety disorders,15 depressive disorders,16 and posttraumatic stress disorders17 indicate that poor neuropsychological performance outcome and increased psychiatric burden are causally associated. We took these observations into account in asking about the extent to which poor health status (more severe symptoms of anxiety and insomnia, depression, and social dysfunctions) might be linked to driving behavior.
A further line of research focuses on the association between poor driving behavior and aggression. Aggressive driving is acknowledged as a contributor to motor vehicle accidents. Thus, the DBQ14 explicitly includes aggressive reactions (ie, aggressive violations and ordinary violations) as a factor of adversely affecting driving. Aggressive reactions are for instance becoming angered by a certain type of a driver and indicating one’s hostility by whatever means one can, or becoming angered by another driver and giving chase with the intention of giving him/her a piece of one’s mind, or sounding the horn to indicate one’s annoyance with another road user. Similarly, Beanland et al8 identified personality traits such as antagonism, negative affectivity, and disinhibition as predictors of poor driving behavior; these personality traits have in common aggressive behavior, understood as a deliberate inclination to threaten another person verbally, nonverbally, or physically. Likewise, Stephens and Sullman18 identified trait aggression as a predictor of crash-related behaviors among drivers from the United Kingdom and the Irish Republic. Further, the same authors showed that aggressive forms of expression were higher for drivers who reported initiating road incidents, and total scores for aggressive expression were also higher for drivers who reported recent crash-related conditions, such as loss of concentration, losing control of their vehicle, moving violations, near misses, and major crashes.
To summarize, there is evidence that aggressive behavior and poor driving behavior are associated. We took this observation into account and asked to what extent aggressive behavior (physical aggression, verbal aggression, anger, and hostility; Aggression Questionnaire; AGQ: Buss and Perry19) was associated with poor driving behavior as measured with the Manchester DBQ.14
With regard to driving behavior and health status, surprisingly, the literature is sparse. Possis et al20 showed that among veterans, poor and risky driving behavior and poor mental health status were associated. Other researchers (eg, Morris et al21) focused on the association between general health status and driving ability among elderly people. Though, whereas Scott-Parker et al11,12 assessed novice drivers, and Hilton et al10 assessed heavy goods vehicle professional drivers, surprisingly, the association between driving behavior and health status among adult and experienced traffic offenders has not been investigated so far. The aim of the present study was, therefore, to explore the association between health status and driving behavior among male traffic offenders.
To summarize, traffic accidents make a substantial contribution to the high mortality rates and health care costs in Iran. Psychological processes that might explain the high rate of traffic accidents include those related to poor health status, aggression, and sociodemographic characteristics. However, to our knowledge, no study of traffic offenders in Iran has taken these variables into account. The aims of the present study were, therefore, to assess Iranian male traffic offenders and to investigate the associations between aggressive behavior, health status, driving behavior, and sociodemographic characteristics. In our view, this study has the potential to contribute to a better understanding of the psychological mechanisms underlying traffic accidents and to help focus efforts to reduce traffic accidents in Iran.
The following two hypotheses and two research questions were formulated. First, following Possis et al,20 Morris et al,21 Scott-Parker et al11,12 and Hilton et al10 we expected that poorer health status would be associated with poorer driving behavior. Second, following Reason et al,14 Beanland et al8 and Stephens and Sullman,18 we anticipated that higher scores for aggression would be associated with poorer driving behavior. Next, we took as exploratory the following two research questions: first, if both health status and aggression traits are associated with poor driving behavior, which dimension emerges as the stronger predictor of driving behavior, when both variables are entered into a regression analysis? Second, to what extent do health status, aggression, and driving behavior vary as a function of sociodemographic and other driver-related factors?
Method
Sample
A total of 443 male traffic offenders (mean age: M =31.40 years, standard deviation =9.56; range: 15–70 years; median: 29 years) took part in the present study. Participants were recruited from February to October 2014 in the Police Center of Kermanshah University of Medical Sciences, Kermanshah, Iran. Sample characteristics are reported in Table 1. Participants had to undergo a brief medical and psychological check because they had violated traffic regulations on at least three separate occasions and because they had the highest number of points on their driving licenses according to police reports. Participants were fully informed about the aims and scope of the present study, and they were assured that all data were anonymized in the analyses and study reporting. Inclusion criteria include 1) male sex, 2) nonaccidental traffic violations on at least three separate occasions and taken to the police station for prosecution, 3) willing and able to complete written questionnaires, and 4) giving written informed consent. Exclusion criteria include 1) not willing or not able to complete written questionnaires, 2) severe health issues such as psychiatric disorders or somatic disorders impeding participation at the enquiry, and 3) a history of substance abuse. The Review Board of the University of Imam Reza of Mashhad (Mashhad, Iran) approved the study, which was conducted following the rules laid down in the Declaration of Helsinki.
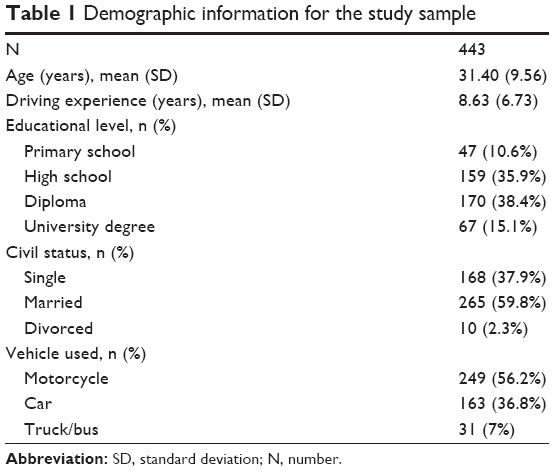 | Table 1 Demographic information for the study sample |
Tools
Sociodemographic and driver-related information
This questionnaire asked for sex, age (years), highest educational level (primary school, high school, diploma, university degree), civil status (single, married, divorced/widowed), years of driving experience (years), and vehicle driven when traffic violations occurred (motorcycle, car, truck/bus).
Driving behavior
Participants completed the Manchester Driving Behaviour Questionnaire (DBQ;14 Farsi version: Oreyzi Samani and Haghayegh22). The DBQ is a self-rating questionnaire consisting of 50 items measuring aberrant driving behaviors and focuses on aggressive violations (eg, “Sound your horn to indicate your annoyance to another road user”; “Become angered by another driver and give chase with the intention of giving him/her a piece of your mind”; Cronbach’s alpha: 0.88), ordinary violations (eg, “Disregard the speed limit on a residential road/motor way”; “Overtake a slow driver on the inside”; “I drive so close to the car in front that it would be difficult to stop in an emergency”; Cronbach’s alpha: 0.85), errors (eg, “Underestimate the speed of an oncoming vehicle when overtaking”; “Fail to check your rear-view mirror before pulling out, changing lanes, etc.”; Cronbach’s alpha: 0.91), and lapses (eg, “Attempt to drive away from the traffic lights in third gear.”, “Forget where you left your car in a car park”; “Intending to drive to destination A, you “wake up” to find yourself on the road to destination B”; Cronbach’s alpha: 0.91). Responses are given on six-point Likert scales ranging from 0 (= never) to 5 (= nearly all the time), with higher mean scores reflecting more numerous violations, errors, and lapses (Cronbach’s alpha: 0.89).
General health
Participants completed the General Health Questionnaire23 (Farsi version: Malakouti et al24). The General Health Questionnaire is a self-rating questionnaire to identify psychological distress. It consists of 28 items and assesses anxiety and insomnia, depression, social dysfunction, and somatic health. Answers are given on four-points Likert scales ranging from 0 (= not at all) to 3 (= more than usual), with higher sum scores reflecting more severe health issues (Cronbach’s alpha from 0.88 to 0.90).
Aggression
Participants completed the Aggression Questionnaire19 (Farsi version: Zahedi25). The Aggression Questionnaire is a self-rating questionnaire, consists of 29 items and focuses on physical aggression, verbal aggression, anger, and hostility. Answers are given on seven-point Likert scales ranging from 1 (= extremely uncharacteristic of me) to 7 (= extremely characteristic of me), with higher scores reflecting a higher tendency toward aggressive behavior (Cronbach’s alpha from 0.84 to 0.91).
Statistical analysis
A series of correlations was computed between the main variables of driving behavior, aggression, health status, age, and driving experiences. To further detect mean differences in driving behavior, aggression, health status, age, and driving experience, a series of one-way analysis of variance was performed with educational level, civil status, and vehicle device as independent factors. Next, a series of multiple regression analyses was performed with driving behavior (aggressive violations, ordinary violations, errors, lapses) as dependent variable and aggression traits (physical aggression, verbal aggression, anger, hostility, total score) and health status (anxiety and insomnia, depression, social dysfunction, physical health, total health score) as predictors. The nominal level of statistical significance was set at alpha =0.05. Statistical computations were performed with SPSS® 20.00 (IBM Corporation; Armonk NY, USA).
Results
Associations between health status, aggression, driving behavior, age and driving experience
Table 2 reports the descriptive statistics and correlations between traits of health status, aggression, driving behavior, and age.
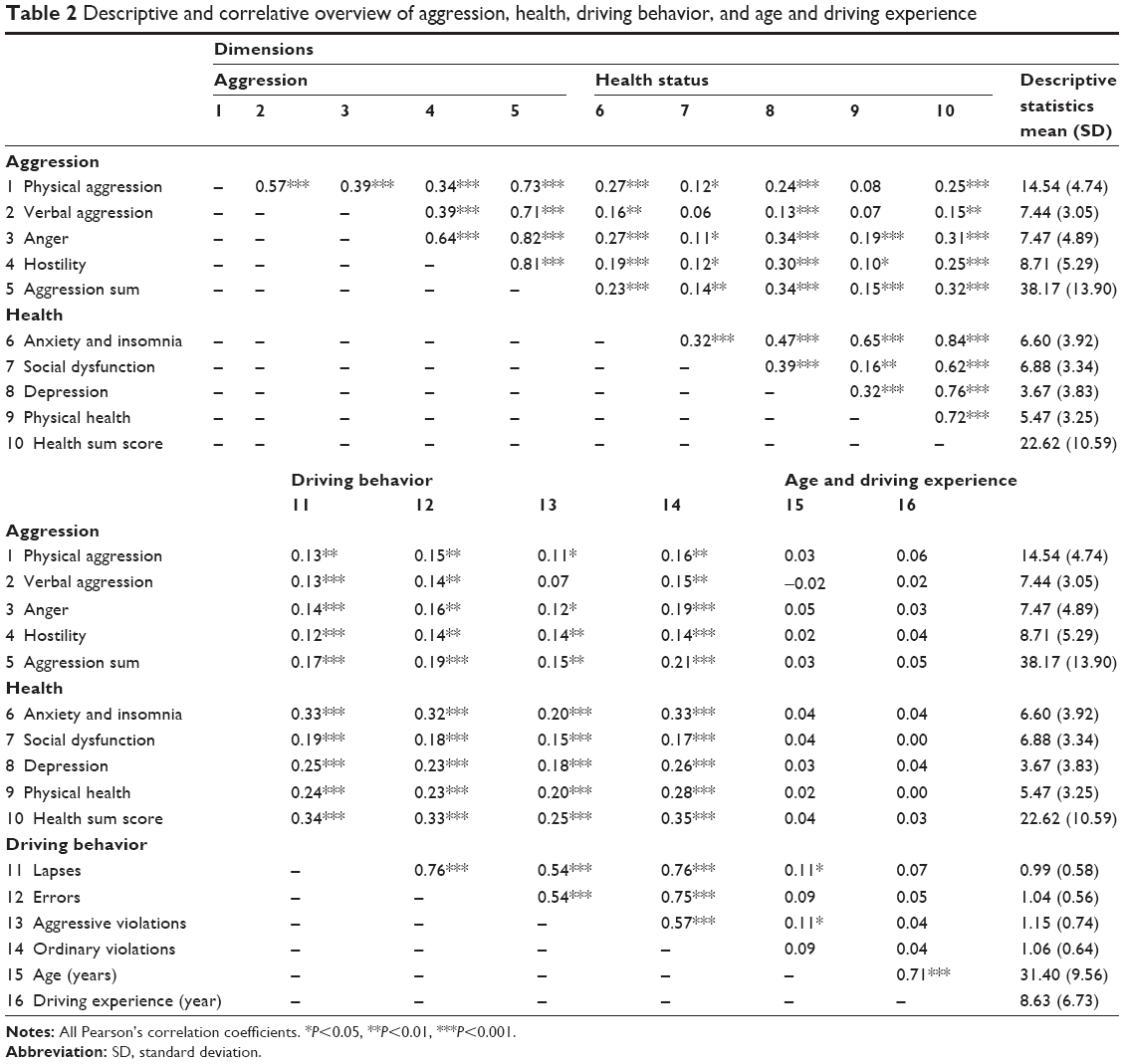 | Table 2 Descriptive and correlative overview of aggression, health, driving behavior, and age and driving experience |
Aggression was associated with poor driving behavior, as was poor health status. Aggression and health status were also associated with each other. Age was statistically unrelated to driving behavior, aggression, and health status.
Predicting driving behavior
To predict driving behavior, a series of multiple regression analyses was performed, with driving behavior as the dependent variable, and aggression traits and health status as predictors.
Poor health status (anxiety and insomnia, depression, social dysfunction, total score; beta =0.35–0.49; r =0.492–0.549; R2 =0.24–0.30; F(1, 441) =26.36–45.98, P<0.001), but not aggression (beta =0.06–0.10; r =0.092–0.120; R2 =0.008–0.014; F(1, 441) =0.92–1.32, P>0.10), independently predicted poor driving behavior (aggressive violations, ordinary violations, errors, lapses).
Educational level, civil status, used vehicle and aggression traits, driving behavior traits, and health status traits
Compared to participants with more education, participants with less education reported more health-related issues, that is, higher scores for anxiety and insomnia, social dysfunction; overall, they had higher total scores for mental health problems (all F>4.56, P<0.01). Aggression and driving behavior did no vary as a function of educational level. For all other sociodemographic dimensions (civil status, vehicle driven) no further significant mean differences were observed (all F<1.2, P>0.30; descriptive and inferential statistics not reported). Driving experience and age were unrelated to health status, aggression, or driving behavior.
Discussion
The key findings of the present study were that among a sample of Iranian male traffic offenders poorer health status and higher aggression were associated with poor driving behavior, though when health status and aggression were entered simultaneously in a multiple regression analysis, poor health status was the only significant predictor of poor driving behavior. In our view, this present pattern of results makes an important contribution to the current literature, in that the health status was introduced as a crucial psychological dimension.
Two hypotheses and two research questions were formulated and each of these is now considered in turn.
First, following Possis et al,20 Morris et al,21 Scott-Parker et al,11,12 and Hilton et al,10 we expected that poorer mental health status would be associated with poorer driving behavior, and this prediction was confirmed. We were able to show that poor mental health status in terms of symptoms of anxiety, depression and insomnia, and social dysfunction was associated with poor driving behavior. We believe that the present pattern of results adds to the current literature in an important way, given that to the best of our knowledge these associations have not previously been investigated or observed, and certainly not among Iranian male traffic offenders.
The data available from this study do not provide any direct insight into the underlying cognitive–emotional processes involved, though in our view the working memory model advanced by Baddeley and Hitch26 may help to explain the association we observed. Briefly, the working memory is part of the human memory system and responsible for keeping current information available, while also retrieving information from long-term memory. Working memory also directs and controls concentration, understood as current capacity to focus cognitive–emotional resources on a specific task. Working memory also elaborates and shifts to consciousness cognitive–emotional processes, so-called current concerns, highly involved in current information elaboration. Current concerns refer to personal needs, thoughts, worries, and often unresolved issues. Following the theoretical framework of Baddeley and Hitch,26 the working memory is limited in the speed, accuracy and amount of information that may be elaborated within a specific time frame. Accordingly, the working memory is unable to store, direct, modulate, elaborate, or focus all informations at the same time. Therefore, it seems plausible that people with higher levels of anxiety, depression, social issues, and poor sleep are less accurate in everyday motor skills and behavior such as driving. In brief, and though we cannot confirm this with the present data, we believe that elevated health difficulties lead to poorer driving behavior due to the limited capacity of working memory. We also note that the performance in neuropsychological assessments is lower in people suffering from psychiatric disorders, and one psychological explanation for this focuses on the impaired capacity of working memory,26,27 leading most probably to the conflict over how to allocate attention between their concerns and the task to be performed.
Our second hypothesis was that higher scores for aggression would be associated with poorer driving behavior, and again this was confirmed. Therefore, the present pattern of results is in accord with and adds to the numerous other studies indicating an association between aggression and driving behavior.14,18,21
The first research question focused on the relative importance of poor mental health and aggression in explaining poor driving behavior, and the results of the multiple regression analyses indicate that only poor health status and not aggression independently explained poor driving behavior. At present, there is no adequate theoretical framework available that can account for this pattern of results. In the absence of such a framework, we advance the following possibility. Drawing on Lazarus and Folkman’s28 concept of coping with stress, aggression and aggressive expression could be regarded as emotion-focused coping strategies (in contrast to problem-focused strategies). Further, symptoms of anxiety, depression, and social dysfunction might also be considered as emotion-focused coping strategies, in that a person seems to be unable to solve problems or to eliminate stressors but tries only to cope with the emotions related to stress. Variance in aggression and aggressive expression may overlap considerably with variance in symptoms of anxiety and depression and aggressive traits may be treated as a specific aspect of health status. Further studies might focus on the extent to which aggressive traits and symptoms of depression, anxiety, and insomnia do indeed share common variance.
The second research question concerned the extent to which sociodemographic variables might systematically affect levels of aggression, health status, and driving behavior. It turned out that lower educational level was associated with higher scores for anxiety and insomnia, and social dysfunction, but was not associated with driving behavior or aggression. Again, the data available could not shed any further light on the underlying mechanisms, and only one study29 has reported that male drivers from disadvantaged socioeconomic backgrounds are at increased risk of poor driving behavior. Further, based on the present results, we conclude that it is not socioeconomic variables, or age, or driving experience but the cognitive–emotional processes underlying poor health status and aggression that are the key determinants of driver behavior.
Although we focused on current psychological states, much of the recent research in this area has focused on personality traits. For example, Mallia et al7 observed associations between excitement seeking and normlessness and aberrant driving behavior among professional bus drivers. Likewise, Edwards et al9 observed a relationship between narcissism and aggressive driving, while, for example, Roberts et al30 claimed that personality traits have the same predictive value for future mortality, divorce, and occupational attainment as cognitive factors, such as IQ, and socioeconomic status. Recently, Beanland et al8 assessed 285 young adults from a university in the southern USA. Participants completed the Manchester DBQ14 and the Personality Inventory for DSM-5. The results showed that antagonism and negative affectivity predicted aggressive violations and ordinary violations, and disinhibition while negative affectivity also predicted error and lapses, whereas we do fully acknowledge the importance and merits of research on personality traits we also have some concerns. First, observations from everyday clinical experience show that, among patients suffering from psychiatric disorders, the set of symptoms are uniform, leading to a precise and observable description of symptoms (see DSM 5 and ICD-10), and that often periods of increased stress trigger the emergence of acute states of psychiatric disorder. Second, recently, we were able to show that, among a large sample of young adults, it was not perfectionism understood as a stable personality trait but underlying poor coping strategies and dysfunctional cognitive–emotional processes that best explained sleep disturbances.31 Accordingly, in the present study, we observed that poor current mental health status as reflected in anxiety and insomnia, social dysfunction, and depression were associated with poor driving behavior; symptoms of anxiety, insomnia, depression, and social dysfunction are by definition not personality traits but are considered state markers, which emerge as a consequence of prolonged stress and the lack of adequate coping strategies (see the so-called diathesis stress model of the emergence and maintenance of psychiatric disorders32). To summarize, the present pattern of results lends support to the idea that current cognitive–emotional constraints are associated with current aberrant driving behavior.
Despite the intriguing findings, several limitations warn against the overgeneralizations of the present results. First, the study is cross-sectional and precludes by definition any conclusions with regard to causal direction in the associations between health status, aggression, and driving behavior. Second, we relied entirely on self-reports. Given that self-reports may be biased, future studies should also include the experts’ ratings. This holds particularly true for psychological health, as it might be expected that psychiatric disorders such as attention-deficit-hyperactivity disorder and substance abuse might affect the driving behavior. Third, the present pattern of results might be due to further latent, but unassessed dimensions, which could have biased two or more variables in the same direction. In this regard, future studies might introduce impulsive behavior/impulse control skills as possible factors. Fourth, given that only males were assessed, we cannot say whether present pattern of results would also hold for female drivers. Fifth, no objective physiological data were collected; such data might have allowed us to illuminate the underlying neurophysiological processes linking aberrant driving behavior, poor health status, and aggression. Sixth, to determine the extent to which the driving behavior of the present sample is more or less dangerous than that of other road users, objective driving behavior, assessments should be included and compared with data from drivers without traffic violations (controls). Seventh, the data do not provide any insight into possible work-related, stress-related or motivational issues underlying current driving behavior, health status, or aggression. Though highly speculative, one might assume that work load, job insecurity, family strain, financial issues, and further stressors might have an impact on the cognitive–emotional processes involved in stress, anxiety, and depression. If we take into account that low educational attainment was associated with poor health status, it is possible that the socioeconomic consequences of lower educational attainment might underlie or at least contribute to higher cognitive–emotional stress, lower health status, and poorer driving behavior. Finally, it might be very strange to find no association with age (Table 2), in that insurance premiums for younger drivers are much higher in most Western countries given clear actuarial evidence of differential risk: younger drivers are much more likely to have accidents. However, we note that the mean age of the present sample was approximately 31.5 years, and that the present sample already consists of male offenders with repeated traffic infractions, and therefore, age did not seem to be an important factor.
Conclusion
The present pattern of results from a sample of Iranian male traffic offenders indicates that poor mental health status, along with aggression, was associated with poorer driving behavior.
Acknowledgment
The present work is the doctoral thesis of Nasrin Abdoli. The authors thank Nick Emler (University of Surrey, Surrey UK) for proofreading the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Moradi S, Khademi A. Survey of victims of car accidents year 1387. J Forensic Med (Persian). 2009;15:21–28. | ||
World Health Organization (WHO). Global Status Report on Road Safety 2013: Supporting a Decade of Action. Geneva, Switzerland: World Health Organisation (WHO); 2013. | ||
Zargar M, Kaji A, Karbkhsh M, Zarei MR. Epidemiology study of facial injuries during a 13 month of trauma registry in Tehran. Indian J Med Sci. 2004;58:109–114. | ||
Montazeri A. Road-traffic-related mortality in Iran. A descriptive study. Public Health. 2004;118:110–113. | ||
Zangooei Dovom H, Shafahi Y, Zangooei Dovom M. Fatal accident distribution by age, gender and head injury, and death probability at accident scene in Mashhad, Iran, 2006–2009. Int J Inj Contr Saf Promot. 2013;20(2):121–133. | ||
Rumar K. The role of perceptual and cognitive filters in observed behavior. In: Evans L, Schwing RC, editors. Human Behaviour and Traffic Safety. New York, NY: Plenum Press; 1985:151–165. | ||
Mallia L, Lazuras L, Violani C, Lucidi F. Crash risk and aberrant driving behaviors among bus drivers: the role of personality and attitudes towards traffic safety. Accid Anal Prev. 2015;79:145–151. | ||
Beanland V, Sellbom M, Johnson AK. Personality domains and traits that predict self-reported aberrant driving behaviours in a Southeastern US University sample. Accid Anal Prev. 2014;72:184–192. | ||
Edwards BD, Warren CR, Tubré TC, Zyphur MJ, Hoffner-Prillaman R. The validity of narcissims and driving anger in predicting aggressive driving in a sample of young drivers. Hum Perform. 2013;26:191–210. | ||
Hilton MF, Staddon Z, Sheridan J, Whiteford HA. The impact of mental health symptoms on heavy goods vehicle drivers’ performance. Accid Anal Prev. 2009;41:453–461. | ||
Scott-Parker B, Watson B, King MJ, Hyde MK. The influence of sensitivity to reward and punishment, propensity for sensation seeking, depression, and anxiety on the risky behaviour of novice drivers: a path model. Br J Psychol. 2012;103:248–267. | ||
Scott-Parker B, Watson B, King MJ, Hyde MK. A further exploration of sensation seeking propensity, reward sensititivy, depression, anxiety, and the risky behaviour of young novice drivers in a structural equation model. Accid Anal Prev. 2013;50:465–471. | ||
Pourabdian S, Azmoon H. The relationship between trait anxiety and driving behavior with regard to self-reported Iranian accident involving drivers. Int J Prev Med. 2013;4:1115–1121. | ||
Reason J, Manstead A, Stradling S, Baxter J, Campbell K. Errors and violations on the road: a real distinction? Ergonomics. 1990;33:1315–1332. | ||
Alves MR, Pereira VM, Machado S, Nardi AE, Oliveira e Silva AC. Cognitive functions in patients with panic disorder: a literature review. Rev Bras Psiquiatr. 2013;35:193–200. | ||
Evans VC, Iverson GL, Yatham LN, Lam RW. The relationship between neurocognitive and psychosocial functioning in major depressive disorder: a systematic review. J Clin Psychiatry. 2014;75:1359–1370. | ||
Qureshi SU, Long ME, Bradshaw MR, et al. Does PTSD impair cognition beyond the effect of trauma? J Neuropsychiatry Clin Neurosci. 2011;23:16–28. | ||
Stephens AN, Sullman MJ. Trait predictors of aggression and crash-related behaviors across drivers from the United Kingdom and the Irish Republic. Risk Anal. Epub 2015 Mar 24. | ||
Buss AH, Perry M. The aggression questionnaire. J Pers Social Psychol. 1992;63:452–459. | ||
Possis E, Bui T, Gavian M, et al. Driving difficulties among military veterans: clinical needs and current intervention status. Mil Med. 2014;179:633–639. | ||
Morris JN, Howard EP, Fries BE, Berkowitz R, Goldman B, David D. Using the community health assessment to screen for continued driving. Accid Anal Prev. 2014;63:104–110. | ||
Oreyzi Samani SHR, Haghayegh SA. Psychometric properties of the Manchester Driving Behavior Questionnaire. Payesh. 2010;9:21–28. | ||
Goldberg DP. Manual of the General Health Questionnaire. Windsor, England: NFER Publishing; 1978. | ||
Malakouti SK, Fatollahi P, Mirabzadeh A, Zandi T. Reliability, validity and factor structure of the GHQ-28 used among elderly Iranians. Int Psychogeriatr. 2007;19(4):623–634. | ||
Zahedi S. Construction and validation of a scale for measuring aggression. J Child Psychol Psychiatry. 2001;3:73–102. | ||
Baddeley AD, Hitch G. Working memory. In: Bower GH, editor. The Psychology of Learning and Motivation: Advances in Research and Theory. New York: Academic Press; 1974:47–89. | ||
Sternberg RJ, Sternberg K. Cognitive Psychology. 6th ed. Belmont, CA: Wadsworth; 2009. | ||
Lazarus RS, Folkman S. Stress, Appraisal and Coping. New York: Springer; 1984. | ||
Tapp A, Pressley A, Baugh M, White P. Wheels, skills and thrills: a social marketing trial to reduce aggressive driving from young men in deprived areas. Accid Anal Prev. 2013;58:148–157. | ||
Roberts BW, Kuncel NR, Shiner R, Caspi A, Goldberg L. The power of personality: the comparative validity of personality traits, socioeconomic status, and cognitive ability for predicting important life outcomes. Persp Psychol Sci. 2007;2:313–345. | ||
Brand S, Kirov R, Kalak N, et al. Perfectionism related to self-reported insomnia severity, but not when controlled for stress and emotion regulation. Neuropsychiatr Dis Treat. 2015;11:263–271. | ||
Monroe SM, Simons AD. Diathesis-stress theories in the context of life stress research: implications for depressive disorders. Psychol Bull. 1991;110:406–425. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.