")
Back to Journals » Risk Management and Healthcare Policy » Volume 8
Perceived risk factors of health decline: a qualitative study of hospitalized patients with multimorbidity
Authors Kuluski K, Tracy CS, Upshur RE
Received 22 December 2014
Accepted for publication 11 February 2015
Published 22 April 2015 Volume 2015:8 Pages 63—72
DOI https://doi.org/10.2147/RMHP.S79720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Frank Papatheofanis
Video abstract presented by Kerry Kuluski
Views: 534
Kerry Kuluski,1,2 C Shawn Tracy,1 Ross E Upshur1–3
1Bridgepoint Collaboratory for Research and Innovation, Bridgepoint Active Healthcare, Toronto, ON, Canada; 2Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada; 3Department of Family and Community Medicine, University of Toronto, Toronto, ON, Canada
Background: Effectively preventing and managing chronic illness are key goals for health systems worldwide. A growing number of people are living longer with multiple chronic illnesses, accompanied by a high degree of treatment burden and heavy use of health care resources. People with multimorbidity typically have to manage their care needs for a number of years, and from this experience may offer valuable perspectives on factors that influenced their health outcome.
Purpose: The purpose of this study was to explore factors that may serve as tipping points into poor health from the perspective of hospitalized patients with multimorbidity.
Participants and methods: Patient interview data were analyzed from 43 hospitalized patients with multimorbidities who indicated that something could have been done to either avoid or slow down their health decline. The study used qualitative description as the analytic method to generate themes from a specific question collected through one-on-one interviews. Two reviewers independently analyzed and thematically coded the data and reached consensus on the final themes after a series of meetings.
Results: According to patient accounts, factors at the personal level (eg, personal behaviors), provider level (eg, late diagnoses), and health care system level (eg, poor care transitions) contributed to their health decline.
Conclusion: This paper focuses on prevention in the context of multimorbidity. While some respondents indicated personal behaviors that impacted health, many pointed to factors outside themselves (providers and the broader health system). The orientation of health care systems, historically designed to support acute and episodic care and not multimorbidity, places patients, at least in some cases, at additional risk of decline. The patient accounts suggest that the notion of prevention should evolve throughout the course of illness. A successful health system would embrace this notion and see the goal as forestalling not only mortality (as achieved for the most part in high socioeconomic nations) but morbidity as well. High rates of multimorbidity and health system challenges suggest that we have not yet achieved this latter aim.
Keywords: Canada, chronic illness, multimorbidity, determinants of health, health service settings, patients
Introduction
Up to 50% of people in developed countries have at least one chronic illness, and up to one-third have multiple simultaneous illnesses,1 referred to as multimorbidity. It is estimated that chronic illness will cost over $30 trillion over the next 20 years, comprising 48% of the global gross domestic product, and increase to 75% when accounting for the cost of mental illness.2 As the number of morbidities increases, so too does the use of health care services and cost.3 In Ontario, Canada, for instance, 5% of the population accounts for 66% of health care costs, and these people are characterized by multimorbidities.4,5 Disproportionate use of health care by a small proportion of the population is a trend found globally.6
Preventing chronic illness and its symptoms (primary prevention), slowing its progression (secondary prevention), and managing the illness to sustain quality of life (tertiary prevention) are key goals across health systems.7 Although a large share of public budgets within industrialized countries is devoted to the health care system, there is clear evidence that our living conditions, such as housing, diet, income, and education, and the policies that impact the way these resources are distributed are the principal factors that influence health outcomes.8,9
Nevertheless, disproportionate attention and funding are devoted to the optimization of health care systems and the management of chronic illness after its occurrence. The health care system which is predominantly acute, curative, and episodic in nature, is ill equipped to manage the needs of our modern population. It is the presence of multimorbidities in particular that often translates into significant treatment burden for patients, families, and care providers. People with multimorbidities tend to interact with many providers and experience poor continuity of care.10 Treatment plans may overlap and contradict each other, and few clinical guidelines exist to support providers in managing multiple conditions in one person.11–15
There is a lack of cohort studies on people with multimorbidities, leaving a poor understanding of risk factors (or “tipping points”) that may lead to health problems in the first place or exacerbations thereafter.16 There is a need to further understand why health problems arise and what predictive factors are amenable to change.14 Understanding the nature of “tipping points” into chronic illness as well as “tipping points” into progressive decline after illness onset can inform both chronic disease prevention and management strategies for not only patients with multimorbidities but all populations at risk. The purpose of this study was to ascertain the factors that may serve as tipping points into poor health from the perspective of hospitalized patients with multimorbidities. The authors explore the results of one-on-one interviews with hospitalized patients with multimorbidities, with specific attention to the response to one interview question that focused on perceived risk factors of health decline. There are no previous studies, to our knowledge, that have elicited perceptions of patients with multimorbidities on their health decline.
Methods
Study setting
The study took place at a complex continuing care and rehabilitation facility based in Toronto, ON, Canada. At this type of facility, patients receive rehabilitation and continuing care to manage multiple chronic health problems following an acute care hospital stay in preparation to transfer to their next point in care (eg, usually home and sometimes facility-based long-term care). In complex continuing care and rehabilitation, patients receive care for a range of ailments, including total joint replacements, advanced diabetes, and neurological and muscular degenerative health problems. These conditions are typically compounded by other morbidities and complications such as osteomyelitis, mobility impairments, and pain. Due to the severity of the conditions and ongoing management required for patients in complex continuing care and rehabilitation, they are referred to as having complex care needs. The research setting provided the researchers with a natural cluster of patients with multimorbidities and complex care needs.
Design and sampling
The study used qualitative description, an analytic approach grounded in naturalistic inquiry. Qualitative description is less interpretative and inferential than other qualitative approaches such as phenomenology and grounded theory, as the intent of the analysis is to stay closer to the surface of words as opposed to reading between the lines and building theories.17 Qualitative description was best suited to this research, given that specific patient interview responses were analyzed.
The study is a component of a broader multimethod study that examined the characteristics, needs, and care experiences of hospitalized patients with complex chronic conditions.18,19 Ethics approval was received on January 26, 2011 from the Joint Bridgepoint–West Park–Toronto Central Community Care Access Centre Research Ethics Board.
Data collection
Research assistants with qualitative research experience who had obtained a Masters or PhD in a health-related discipline conducted the interviews using a structured interview guide. The interview guide was based on a framework developed by the research team and is detailed in a separate paper.20
The interviews were conducted with a convenience sample of hospital inpatients between February and July 2011. The study sample was identified with the assistance of hospital unit care managers. Patients were eligible to participate if they met all of the following criteria: could provide informed consent, could withstand sitting in a one-on-one interview format for at least 15 minutes at a time, and could cognitively understand questions and provide verbal responses. If the capacity of the patient to participate was questioned, then the unit physician was consulted. Patients were informed that their decision to participate would not impact their present or future care at the study setting. As outlined in Figure 1, 158 patients were approached and 119 consented. Reasons for refusal included fatigue and lack of interest. Three of the consenting patients were discharged before the scheduled interview, leaving 116 patients. Interviews typically took just over 1 hour, ranging from 30 minutes to over 2 hours in a few cases. A small number of the interviews occurred over multiple visits to accommodate the patient’s rehabilitation schedule and/or personal preference.
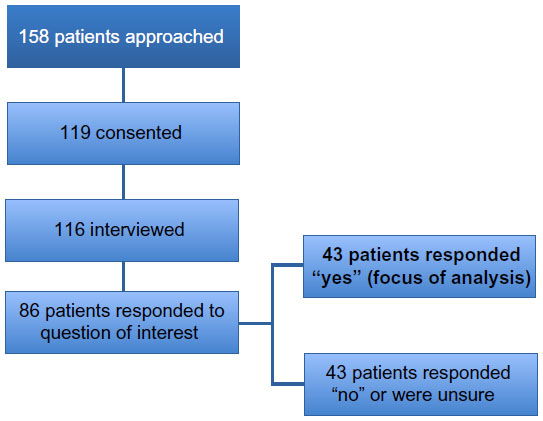 | Figure 1 Sample flow chart. |
For the purpose of the present study, from the full collection of 116 interviews, 86 patient interviews were selected, reflecting the number of patients who responded to the interview question of interest “What, if anything, might have changed how things turned out for you in terms of your health?”. Within the broader interview guide, this question was positioned toward the end, which may account for some of the missing responses (see the “Strengths and limitations of the study” section). Of the 86 responses, 43 patients indicated that something could have been done to prevent their health decline. Given the interest in unpacking chronic disease prevention and “tipping points” into complex health, the paper focuses on these 43 patient responses in addition to descriptive analysis of the demographic differences by response category (those who responded “yes” to the question compared with those who responded “no” or “unsure”).
Data analysis
Answers to the interview question “What, if anything, might have changed how things turned out for you in terms of your health?” were extracted from a database of interviews that were previously stored and analyzed by the lead author (KK). Computer-assisted qualitative data analysis software (NVivo 9) was used to generate a node report detailing all participant responses to the aforementioned question of interest. The node report was read by two of the authors independently (KK and CST). KK and CST are PhD and Masters trained, respectively, with several years of experience in conducting qualitative research, particularly with vulnerable patient populations. KK and CST coded the interview data in two stages: open coding and axial coding. Open coding entails reading through the interview responses and making notations in the margins. After reading through the notations, several codes were derived and similar codes were aggregated into themes (axial coding). Following this, similar themes were merged to eliminate redundancy.21 To ensure consistency in interpretation, the two reviewers met to compare notes, discuss and clarify themes, Consensus was reached on all themes (and the codes within themes) after three meetings that were approximately 2 hours in length. To ensure descriptive validity, the researchers referred back to the full interview transcript and field notes to contextualize the responses that were in the node report. This process allowed the researchers to settle discrepancies and enhance confirmability during the review process. Patients were not contacted to check or verify the findings. Many of the patients had been discharged from hospital by the time the analysis for this study took place, and the researchers did not have ethics approval to contact them again after the study.
The main focus of the paper is on responses from participants who believed that something could have changed their health outcome. The reason for this focus was to illuminate a deeper understanding of factors that may be potentially modifiable. Despite this more refined scope of the paper, we briefly touch upon the participants who indicated that nothing could have changed their health outcome as well as those who were uncertain.
Results
As outlined in Table 1, 86 participants responded to the question of interest within the interview. Participants were predominantly English speaking (90.7%) and over half were female (55.8%) and had more than a high school education (61.9%). Most of the participants (72.9%) were unattached (single, never married, widowed, or divorced) and had an average age of 61.38 years, ranging from 28 to 96 years. The prevalence of multimorbidity was high, with an average of over five chronic conditions per patient (mean =5.3; standard deviation =2.034). The most common admitting diagnosis was musculoskeletal in nature (eg, fractures), followed by neurological conditions (eg, stroke, multiple sclerosis). These proportions are reflective of the broader population (full 116 interviews) reported in a separate paper.18 Some demographic differences were found when comparing participants who fell into different response groups. Participants who felt that something could have been done were more likely to be unattached (widowed, separated, divorced, single/never married), more highly educated, and hospitalized for a neurological condition, compared with their counterparts who responded “no” or “unsure”. The most common admitting diagnosis among the group reporting no difference or uncertainty was musculoskeletal in nature (eg, fractures). No differences between sex and number of health conditions were seen between the two groups, and minimal differences were seen in age and the proportion of patients who reported English as their primary language.
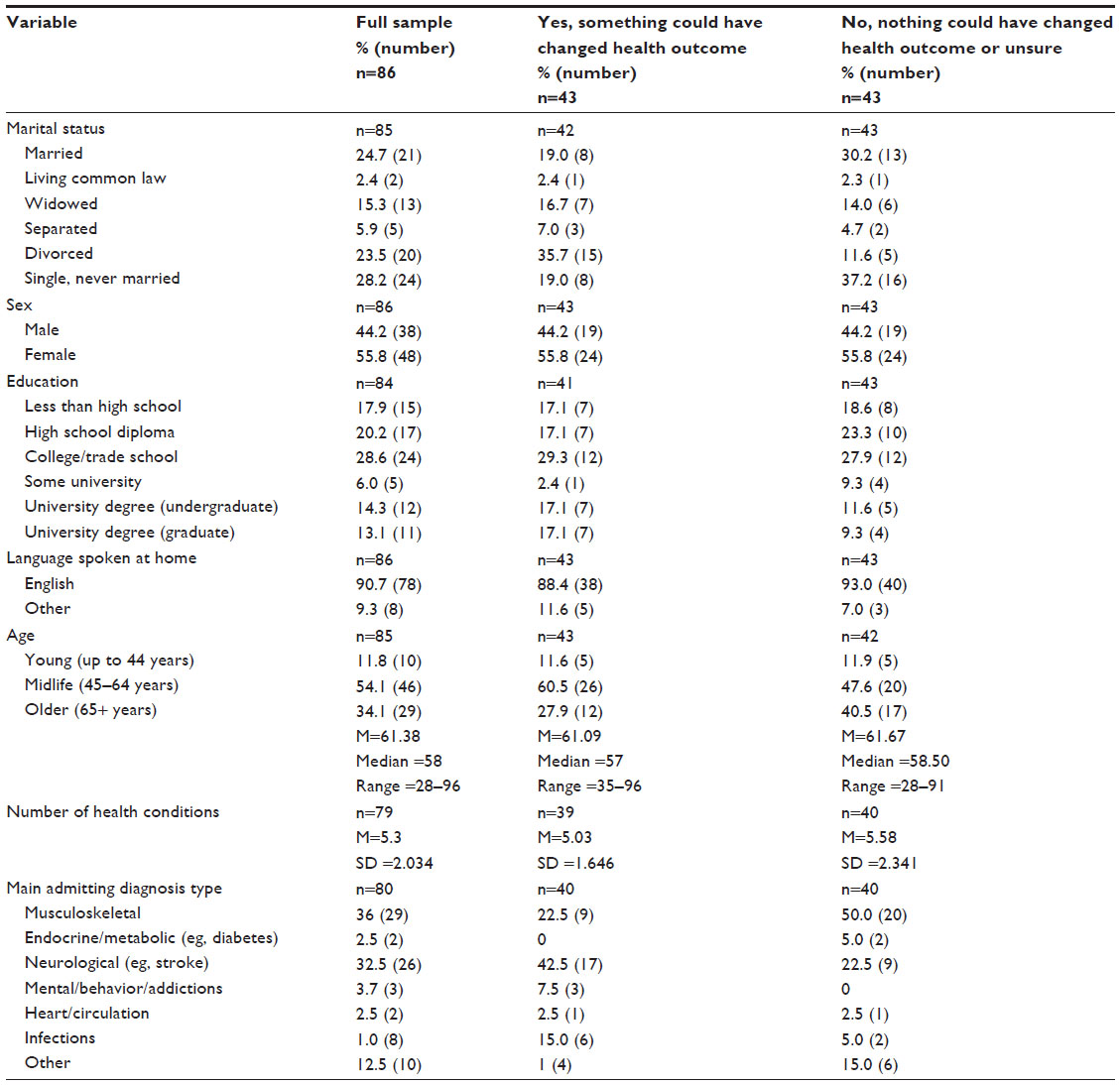 | Table 1 Patient characteristics |
Patient accounts of what might have prevented their current health conditions clustered into three broad themes: personal factors such as engaging in healthier behaviors and making different decisions regarding their health; health care provider factors, including misdiagnoses and poor communication on the part of a physician or other health care professional; and health care system level factors, including poorly executed care transitions, lack of access to needed care, and poor-quality care experiences. While the latter two themes are closely intertwined, the provider theme focuses mainly on clinical decision making and encounters with the patient, while the health care system theme captures consequences of system design (eg, fragmentation and poor transitions). For each theme, example quotes are provided. In the quotes, square brackets with dashes […] signify removal of text that was redundant or unrelated to the point being illustrated. Dashes without brackets signify a pause in the participant’s response.
Personal factors
Some participants felt that they could have potentially altered the course of their illness trajectory through their own personal behaviors. This included engaging in healthier behaviors and responding to health advice given by doctors and family members.
More specifically, some patients blamed their current health problems on their unhealthy weight, alcohol consumption, smoking, and (in one case) use of illegal drugs. A patient in her late 50s was in hospital due to alcohol-induced acute pancreatitis, liver disease, and a urinary tract infection. When asked if she felt that anything could have been done to prevent or change her health problem, she shared:
Yes. Not drinking. That’s exactly … And probably admitting to myself two things. You know, there are life circumstances that are beyond you. So you know, a death, an illness in a family. You know, a partner leaving you. And you have to learn to accept and cope. But I should have realized sooner about work. You know, saying I really just don’t like this and I need to do something about it. That would have helped. (Patient #43)
This participant went on to recount how she self- medicated with alcohol to deal with workplace stress. Similarly, other patients described their behavior as a response to work- or family-related issues. A number of patients provided less context and were quite matter of fact in their responses; for example, one patient noted: “If I hadn’t drank so much, I wouldn’t be here.” (Patient #91).
In another case, a patient with MS, wounds, and anxiety said:
I wish I worked out more before I got here. I absolutely do. Working out is what I needed. And this is why I think I’m in this state today. But I’ll be alright. (Patient #11).
As patients reflected on the causes of their conditions, some felt that they were not proactive in seeking medical advice. A patient who was recovering from her second knee replacement accompanied by high blood pressure, gastrointestinal disease, and cardiac dysrhythmia, among other ailments, noted feeling “very, very depressed” and felt she “let [the depression] go for too long”. (Patient #115). A 72-year-old patient with chronic obstructive pulmonary disease, osteoporosis, paraplegia, and signs of depression noted that her family members encouraged her to seek medical help sooner. She noted that if she “hadn’t been quite so stubborn”, things may have turned out differently (Patient #26).
A number of patients reflected that they should have accepted advice from their care providers and families. A 67-year-old patient with acute osteomyelitis had been dealing with multiple sclerosis for 35 years at the time of the interview. She explained that her bed sores were the factor that tipped her into poor health. When she reflected on her illness experience, she felt that she could have complied with recommendations from health providers to ease the severity of her wounds. She noted: “If I had listened. I think. They wanted to change my cushion [but] I was so comfortable, I didn’t want to change it.” (Patient #5).
Health care provider factors
Many patients shared stories of poor care experiences when responding to the question of what factors may have changed their health outcome. The issues mentioned included lack of communication with their care providers, dismissal of symptoms by health care professionals, and delayed diagnoses. An 84-year-old patient with back pain, lupus, osteoarthritis, and fibromyalgia shared the following:
Well, getting a quicker diagnosis for my knee might have changed quite a few things. It might have even changed where I stayed. I don’t know about that. Had they diagnosed it properly, they might have kept me there instead of sending me to [hospital] because they thought [hospital] would do therapy right away. And that wasn’t true. I just laid there for quite a while. (Patient #45)
Likewise, a 56-year-old patient with an ulcer, cellulitis, arthritis, hypertension, and diabetes felt that her concerns were not taken seriously by her physician, despite her persistence:
My personal physician. […] Definitely he didn’t catch it in time […] Because I didn’t keep persisting upon it or anything. I should have been more proactive with it. And so should have he. He didn’t really do anything until it got really bad. And I don’t understand why. Like I had to tell him a few times, “It’s getting worse. It’s getting this.” And he would look at it and give me some cream. And then finally he looked at it and said, “Make an appointment at [name of hospital].” No, finally he said, “You need … This needs more care than what I can do because it needs a wrap and everything.” So he referred me to [name of homecare agency]. (Patient #12)
Another patient, who was 53 years of age with a rare genetic disorder, hypertension, and depression, noted:
It would not be preventable, but it probably could have been slowed down if you had the proper physiotherapist and the occupational therapist to work with you, to work with the patient. (Patient #9).
Health care system level factors
Health care system level factors included poorly executed transitions, lack of timely access to care, and poor quality of care. Individuals with multimorbidities often undergo many transitions between health sectors to seek treatments from different care providers. Many experiences of poor care were articulated regarding these transition points. Poorly executed transitions can have deleterious effects on health, as is seen in the case of this 55-year-old patient with infected wounds, a knee prosthetic, osteoarthritis, and gastrointestinal disease:
My wounds were bad but manageable, needing treatment once a day while I was out. They were starting to look a little ugly, looking like I might have a pseudomonas infection. I always get pseudomonas in these things. And I was about to see my family doctor to get a topical antibiotic prescription. Unrelated to that, I developed very rapidly a different kind of infection in my knee, and landed in the hospital. Because I hadn’t yet got the antibiotic for my ankle, they didn’t give it to me when I got into the hospital. And it took over a week for them to get around to agreeing I needed it and could get it. When they agreed that I needed it, it was on a weekend and it would take until Monday. And by the time they were just about to give it to me but hadn’t yet, I was switched to [a different hospital]. And then another week going through the same thing. Two weeks of inadequate care. The wounds went way out of control, and that’s why I can’t walk. (Patient #75)
After his wounds worsened, care staff recommended admission to a long-term care facility (ie, nursing home), which he refused, given that he was the primary breadwinner in his household and had a partner at home who also had health problems.
A 55-year-old patient who felt depressed following his divorce while contending with multiple sclerosis and cellulitis shared the following when asked if anything could have been done to prevent or change his health outcome:
Yes, maybe if I had more money and more support, yes, it would have definitely been better. Because I had nobody really to help me out. My father, he used to come visit me about once a week, sometimes once every two weeks. But yes, I would have been better off if I had more money and more support. But I didn’t know where to access it. (Patient #19)
Similarly, in relation to access to care in the community, a patient in her thirties who was in hospital due to hip replacement complications stated: “Basically maybe if the government would let up on some of the physio places, there wouldn’t be a waiting list so long. […] you know how the physio was before all these cutbacks with the government … maybe there wouldn’t be a lot of people at [hospital].” (Patient #16).
Finally, a 63-year-old patient with type 2 diabetes, osteoarthritis of the lumbar spine, and hypertension talked about a lack of patient-centered care among other health system challenges:
There isn’t enough money. There isn’t enough staff. There is no monitoring of staff. It requires a serious revision of the health system. I believe now it’s called patient-centred care. It’s astonishing that it was ever something else centred care. I call it the health system, not the health care system. There’s very little care. (Patient #96)
While the focus of this paper is on the responses from patients who felt that something could have been done to change their health outcome, we reflect briefly on the responses from patients who felt that nothing could have changed their current circumstances or were unsure. In these cases, illness was often attributed to “bad luck”, particularly if hospitalization was a result of an injury from an accident. A man in his late forties who fell down the stairs and fractured his neck stated: “It was an accident, period.” Others felt that their chronic disease(s) or associated complications were inevitable. A patient in her late 50s had been dealing with osteoarthritis in her knees since she was in her 30s and noted: “No. Life is life …. my cards were dealt and I didn’t win blackjack.” (Patient #55).
Others were unsure. A patient who had been suffering from diabetes for the last 40 years noted:
I don’t know. Right now, I don’t know. My daughter does everything for me right now. She did everything for me so I wouldn’t know. (Patient #33).
In other cases, participants wavered, contemplating that perhaps something could have been done, but were less definitive in the connection. An 82-year-old patient contemplated the question and concluded:
Well, the health condition really is the arthritis. I could have had my knees operated on, got new knees which probably would have helped, but I didn’t. But outside of that I don’t know. I don’t take much medication for arthritis. (Patient #110).
Discussion
People with multimorbidities who are ongoing users of the health care system can offer important insights into factors that impact health outcomes. In this study, we analyzed interview responses from people receiving care in a complex continuing care hospital. These participants were asked if anything could have changed their health outcomes. People in this care environment are characterized by multimorbidities and require intensive oversight to manage their conditions.
Patient accounts pointed to factors at the personal, provider, and health care system level that impacted their health outcomes. In this discussion, we illustrate these three themes under subheadings from direct patient quotes.
“It’s all my fault”
Some patients pointed to their own behaviors as contributing to their health problems. In some of these cases, patients linked their behaviors as a response to stress experienced in their home or work environments. Linkages between stress and poor health are well documented in the literature and may surface only after a number of years.22 Individuals who attribute personal responsibility for poor health may also delay seeking medical care and subsequently experience severe and unnecessary exacerbations in health.23 On the other hand, when patients do enter the health care system, these underlying stressors, which often relate to the social determinants of health (housing, income, work), that precipitate illness may go unrecognized and untreated and be excluded from clinical assessments.20 Needless to say, understanding and addressing the factors in people’s environment that precipitate illness are required yet typically fall outside the scope of traditional health care services.
Some patients wished that they had sought help sooner, or only realized in hindsight that they should have heeded advice provided by care providers, family, and friends. Some of these patients had been dealing with poor health for some time, with an added symptom suddenly tipping them into a more complex state.
It is critical for health care professionals and patients to work together to unearth barriers to the uptake of self-management strategies as well as anticipate and prepare for illness decline. This fundamental relationship between the care provider(s) and patient is the foundation of Wagner et al’s24 chronic care model (CCM). The CCM outlines components of health systems that lend to better chronic illness care, and is detailed more explicitly elsewhere.24 Our data provide insight on the conversation that needs to take place within this relationship (ie, identifying self-management barriers, formulating potential solutions, and anticipating future needs), with the overall goal of mitigating decline. In this light, our findings also have implications for enhanced chronic disease management models such as the expanded chronic care model developed by Barr et al,25 which focuses on chronic disease prevention and the broader system of care surrounding the patient.
“They didn’t listen to me”
Further to our argument on improving the patient-provider relationship, some participants were frustrated with care providers for missed or late diagnoses and complained about “not feeling heard” during clinical consultations. Effective, ongoing, two-way communication characterized by shared decision making, self-management support, and goal setting is the foundation of a robust patient–provider relationship.26–28 Creating a space for patients, their families, and care providers to have these conversations is critical yet does not always occur.29,30
The solution is complicated by the constraints that providers experience in practice. A systematic review and synthesis conducted by Sinnott et al14 in 2013 examined key issues experienced by primary care providers in providing care for persons with multimorbidity. These issues included the fragmentation of health care services characterized by the involvement of several medical specialists who failed to effectively communicate with each other and to the primary care provider; the insufficiency and lack of clinical guidelines; the difficulty in addressing the wider needs of patients, including their psychosocial needs; and the issues related to shared decision making. To this latter point, giving patients choice at times led to patient distress. Much attention is needed to discern what a quality care experience looks like for people with multimorbidity and how to appropriately equip providers to enable this experience.
“I call it the health system, not the health care system. There’s very little care”
During health encounters, patients in our study commented on the lack of patient-centered care. As noted in the literature, patient-centered care in the context of a clinical encounter has several components, including exploring the patient’s main need or concerns; seeking a full understanding of the patient, including their emotional needs; finding common ground and mutually agreeing on how to manage the identified challenges; incorporating prevention and health promotion; and having a continuous relationship.31 A key component of this definition is the patient as a partner in their care. As can be seen in our findings, the patient perspective was not always considered during health encounters, and this may have led to potentially preventable adverse events and was particularly heightened during care transitions.
Health services researchers have pinpointed transitions as an area that requires reform, particularly for people with complex care needs. Patients, the common denominator amid the varied settings and providers encountered, should be included as a partner in care to facilitate a smoother process and enhance informational continuity.32 Transitions, however, require more than a simple “checklist”. An understanding of the needs and concerns of patients and their families as they move to the next point of their care journey needs to be part of a well-coordinated transitions plan. Patients are embedded in a complex social structure that must be considered in order to provide care that is in line with the principles of patient-centered care. This includes not only the needs and values of patients but also the capacity of, and impact on, the families of patients. Furthermore, the orientation of health care systems, historically designed to support acute and episodic care and not multimorbidity, places patients, at least in some cases, at additional risk of decline.
Although the study focused on people who identified factors that influenced their health outcomes, we note some interesting sociodemographic differences between those who reported factors that potentially altered their health outcome and those who felt that nothing could have been done. The most notable difference was found when comparing marital status between the two groups. Patients who felt that something could have been done to change their health outcome were less likely to be married or have a partner. Marital status provides some indication of one aspect of the patient’s social support network. Previous research has shown differences in health perceptions and health outcomes between those who are married/have a partner and those who are unattached.33 The absence of a partner, who may have assumed the role of the caregiver, confidante, and/or navigator for the patient, could have, to some degree, influenced the persons health trajectory. Other people in the patient’s social support network, such as next of kin, neighbors, friends, and volunteers, likely played a role in the overall care experience of the patient but were not captured in this study. Furthermore, it is insufficient to examine presence of social support (such as a partner) without also understanding the quality of that relationship. Further research is required to tease out the relationships between marital status, the quality of social support, other sociodemographic differences and the perception of potentially preventable health outcomes. Important limitations regarding this finding are reported in the following section.
Strengths and limitations of the study
The study setting is a stand-alone care facility for individuals with complex care needs, a unique feature of Ontario’s health care system. It provided a rare opportunity to study a high-needs population in one contained setting. A key limitation in our study stems from the length of the interview guide, as the original study was designed for a much broader purpose. The original study intent was to conduct a full assessment of the characteristics, needs, and experiences of hospitalized patients with complex chronic illness. The question of interest for this paper was positioned toward the end of the interview guide, and there is a strong likelihood that interviewer and respondent fatigue may have set in. There were a number of instances when the question was skipped (which at times was a product of the interviewer perceiving fatigue in the respondent). Respondents had the option of breaking up the interview into components to accommodate rehabilitation schedules, needed breaks, and personal preference. Nevertheless, our study may have missed key perspectives among some of the most chronically ill patients. In addition, the sociodemographic differences found in the respondent groups (namely marital status) need to be interpreted with caution. The transferability of findings can be confirmed through further research on other multimorbid populations within similar care settings. Despite these limitations, a rigorous thematic analytic approach was taken by two highly skilled researchers to ensure the credibility and confirmability of thematic findings. From this process, a rich body of data was generated from a highly complex, vulnerable patient population who historically have been excluded from research.
Conclusion
This paper focuses on prevention in the context of multimorbidity and patient experience. The respondents suggest that risk factors operate at the personal, provider, and health system levels, which have particular relevance for secondary and tertiary prevention: ie, how we can consider ways to potentially slow down disease progression and manage complex health issues to sustain quality of life, respectively. In this light, how we think about prevention should evolve throughout the course of illness. A successful health system would embrace this notion and see the goal as forestalling not only mortality (as achieved for the most part in high socioeconomic nations) but morbidity as well. High rates of multimorbidity and health system challenges suggest that we have not yet achieved this latter aim.
Acknowledgments
The authors gratefully acknowledge the management and staff at Bridgepoint Active Healthcare for supporting the research reported in this paper. The authors acknowledge- the team of data collectors and analysts as well as the patient care managers who were instrumental in recruiting patients to participate in the study. Most importantly, the authors thank the patients featured in this paper for sharing their time and experiences. The lead author was supported by the Great West Life, London Life Canada Life New Scientist Fund as well as the Health System Performance Research Network (funded by the Ontario Ministry of Health and Long-term Care). The views reflected in this paper are those of the research team and not the funders.
Author contributions
KK designed the study, analyzed the data, drafted and revised the manuscript. CST analyzed the data and assisted with manuscript revisions. REU provided conceptual insights and edited the manuscript.
Disclosure
The authors declare no conflicts of interest.
References
Schoen C, Osborn R, Doty MM, Bishop M, Peugh J, Murukutla N. Toward higher-performance health systems: adults’ health care experiences in seven countries, 2007. Health Aff (Millwood). 2007;26(6):w717–w734. | |
Bloom DE, Cafiero ET, Jané-Llopis E, et al. The Global Economic Burden of Noncommunicable Diseases. Geneva, Switzerland: World Economic Forum, Harvard School of Public Health; 2011. | |
Charlson M, Charlson RE, Briggs W, Hollenberg J. Can disease management target patients most likely to generate high costs? The impact of comorbidity. J Gen Intern Med. 2007;22(4):464–469. | |
Commission on the Reform of Ontario’s Public Services. Public Services for Ontarians: A Path to Sustainability and Excellence. Toronto, ON: Ontario Ministry of Finance; 2012. | |
Rosella LC, Fitzpatrick T, Wodchis WP, Calzavara A, Manson H, Goel V. High-cost health care users in Ontario, Canada: demographic, socio-economic, and health status characteristics. BMC Health Serv Res. 2014;14:532. | |
Reid R, Evans R, Barer M, et al. Conspicuous consumption: characterizing high users of physician services in one Canadian province. J Health Serv Res Policy. 2003;8(4):215–224. | |
Institute for Work and Health. What Researchers Mean by Primary, Secondary and Tertiary Prevention. At Work. 43 (Winter 2006). Toronto, ON: Institute for Work and Health; 2006:2. | |
Mikkonen J, Raphael D. Social Determinants of Health: The Canadian Facts. Toronto, ON: York University School of Health Policy and Management; 2010. | |
Raphael D. Social determinants of health: an overview of key issues and themes. In: Raphael D, ed. Social Determinants of Health. 2nd edition. Toronto, Ontario: Canadian Scholars’ Press Inc.; 2009:2–19. | |
Salisbury C, Johnson L, Purdy S, Valderas JM, Montgomery AA. Epidemiology and impact of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract. 2011;61(582):12–21. | |
Tinetti ME, Basu J. Research on multiple chronic conditions: where we are and where we need to go. Med Care. 2014;52 Suppl 3:S3–S6. | |
Lugtenberg M, Burgers JS, Besters CF, Han D, Westert GP. Perceived barriers to guideline adherence: a survey among general practitioners. BMC Fam Pract. 2011;12:98. | |
Lugtenberg M, Burgers JS, Clancy C, Westert GP, Schneider EC. Current guidelines have limited applicability to patients with comorbid conditions: a systematic analysis of evidence-based guidelines. PLoS One. 2011;6(10):e25987. | |
Sinnott C, Mc Hugh S, Browne J, Bradley C. GPs’ perspectives on the management of patients with multimorbidity: systematic review and synthesis of qualitative research. BMJ Open. 2013;3(9):e003610. | |
Muth C, Kirchner H, van den Akker M, Scherer M, Glasziou PP. Current guidelines poorly address multimorbidity: pilot of the interaction matrix method. J Clin Epidemiol. 2014;67(11):1242–1250. | |
France EF, Wyke S, Gunn JM, Mair FS, McLean G, Mercer SW. Multimorbidity in primary care: a systematic review of prospective cohort studies. Br J Gen Pract. 2012;62(597):e297–e307. | |
Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–340. | |
Kuluski K, Hoang SN, Schaink AK, et al. The care delivery experience of hospitalized patients with complex chronic disease. Health Expect. 2013;16(4):e111–e123. | |
Kuluski K, Bensimon CM, Alvaro C, Lyons R, Schaink AK, Tobias R. Life interrupted: the impact of complex chronic disease from the perspective of hospitalized patients. Illn Crises Loss. 2014;22(2):127–144. | |
Schaink AK, Kuluski K, Lyons RF, et al. A scoping review and thematic classification of patient complexity: offering a unifying framework. Journal of Comorbidity. 2012;2(1):1–9. | |
Merriam S. Qualitative Data Analysis. Qualitative Research: A Guide to Design and Implementation. San Francisco, CA: Jossey-Bass; 2009:169–207. | |
Evans R, Barer M, Mamor T. Why Are Some People Healthy and Others Not? New York, NY: Aldine de Gruyter; 1994. | |
Richards H, Reid M, Watt G. Victim-blaming revisited: a qualitative study of beliefs about illness causation, and responses to chest pain. Fam Pract. 2003;20(6):711–716. | |
Wagner EH, Bennett SM, Austin BT, Greene SM, Schaefer JK, Vonkorff M. Finding common ground: patient-centeredness and evidence-based chronic illness care. J Altern Complement Med. 2005; 11 Suppl 1:S7–S15. | |
Barr VJ, Robinson S, Marin-Link B, et al. The expanded Chronic Care Model: an integration of concepts and strategies from population health promotion and the Chronic Care Model. Hosp Q. 2003;7(1):73–82. | |
Reuben DB, Tinetti ME. Goal-oriented patient care – an alternative health outcomes paradigm. N Engl J Med. 2012;366(9):777–779. | |
Tracy CS, Bell SH, Nickell LA, Charles J, Upshur RE. The IMPACT clinic: innovative model of interprofessional primary care for elderly patients with complex health care needs. Can Fam Physician. 2013;59(3):e148–e155. | |
Muth C, van den Akker M, Blom JW, et al. The Ariadne principles: how to handle multimorbidity in primary care consultations. BMC Med. 2014;12:223. | |
Gill A, Kuluski K, Jaakkimainen L, Naganathan G, Upshur R, Wodchis WP. “Where do we go from here?” health system frustrations expressed by patients with multimorbidity, their caregivers and family physicians. Healthc Policy. 2014;19(4):73–89. | |
Kuluski K, Gill A, Naganathan G, Jaakkimainen R, Wodchis WP. A qualitative descriptive study on the alignment of care goals between older persons with multi-morbidities, their family physicians and informal caregivers. BMC Fam Pract. 2013;14:133. | |
Belle Brown J, Stewart M, Westen W, Freeman T. Introduction. Patient-Centered Medicine Transforming the Clinical Method. 2nd edition. Abingdon, UK: Radcliffe Medical Press; 2003:3–15. | |
Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003;51(4):549–555. | |
Robards J, Evandrou M, Falkingham J, Vlachantoni A. Marital status, health and mortality. Maturitas. 2012;73(4):295–299. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.