")
Back to Archived Journals » Research and Reports in Biology » Volume 6
Parental roles in the development of obesity in children: challenges and opportunities
Authors Danford CA, Schultz C, Marvicsin D
Received 3 October 2014
Accepted for publication 8 December 2014
Published 13 April 2015 Volume 2015:6 Pages 39—53
DOI https://doi.org/10.2147/RRB.S75369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Zvi Kelman
Cynthia A Danford,1 Celeste M Schultz,2 Donna Marvicsin2
1Department of Health Promotion and Development, University of Pittsburgh, School of Nursing, Pittsburgh, PA, USA; 2Department of Health Promotion/Risk Reduction, University of Michigan, School of Nursing, Ann Arbor, MI, USA
Background: The prevalence of childhood obesity has become a global concern and evolves from the complex interaction of multiple factors. In particular, the influence of socioeconomic status and ethnicity when combined with family dynamics are important, yet remain inconsistent in their association with childhood obesity. Parents, as influential family members, play a primary role in the development of their children’s eating and activity behaviors that may contribute to increased weight. This integrative review 1) examines the parental role in the development of childhood obesity and 2) identifies implications for health programs and policies.
Method: Systematic searches using five databases followed by a lateral search were conducted between April and June 2014. Inclusion criteria included empirical research published in the last 5 years addressing the role that parents with children 12 years and younger play in their child being or becoming obese. Nineteen publications were identified.
Results: Six themes related to the association between parental role and childhood obesity emerged from our review. These themes included parenting style, parent influence on feeding, modeling, self-efficacy, concern, and bidirectional interaction of the parent-child dyad. Parenting style, modeling, and self-efficacy were not consistently associated with childhood obesity. Parental concern, however, was linked to specific feeding practices. Parental restriction and pressure to eat certain foods were both found to be inversely related to a child’s weight status. Parent’s role in promoting activity was infrequently addressed.
Conclusion: When addressing eating and activity behaviors among children, the role that parents play in feeding their child and their concern for their child’s health is critical. Including mothers and fathers as potential “agents of change” and considering their cultural norms are two elements necessary for effective health programming and policy development.
Keywords: parental role, childhood obesity, parenting behaviors
Introduction
The prevalence of childhood obesity has increased considerably during the past 20 years, creating concern for the future health and well-being of millions of children worldwide.1,2 Strategies to help overcome what has come to be known as “the obesity epidemic” remain challenging, given the vulnerability of children and the complex nature of their environment. A child’s early environment, although seemingly limited, is comprised primarily of the family. The family remains an influential force even as the child’s environment expands to include peers and school while the child matures.3 Within the family, parents are key members who influence a child’s behavior. They do so by carrying out their role through parenting. Parenting refers to activities enacted by parents when interacting with their child to facilitate physical, social-emotional, and behavioral health and well-being throughout the child’s lifespan.4 The role that parents play in the development of their child’s healthy behaviors, particularly those related to eating and activity, is critical. In turn, children rely on their parents to structure their environment and promote healthy choices that sustain energy balance and weight throughout childhood into adulthood. Given the role that parents play in the development of eating and activity behaviors, it is not surprising that parents have been referred to as agents of change.5,6 Consequently, parental roles require careful consideration in the prevention and treatment of childhood obesity.
Parental activities vary according to the age and needs of the child and are influenced by the context of the environment, both within and outside the family. Factors such as socioeconomic status (SES) and ethnicity contribute to the complexity of the interaction between parents and children. Additionally, the incidence of obesity and the risk of becoming obese has become a global concern crossing all incomes and ethnicities at various rates. Moreover, it has been documented that the prevalence of obesity in developed nations is inversely related to SES; while, obesity in developing countries is most prevalent among the wealthy.7 For example, in a study in the United States, low family income (ie, < $25,000) during the prenatal period was significantly associated with high body mass index (BMI) during the adult years. Interestingly, an increase of $10,000 in family income reduced the odds of becoming either overweight or obese as an adult.8
In contrast, results from a study with families of preschool-age children in the United States and France did not support the relationship between household income and children’s BMI.9 However, when examining the relationship between maternal employment and children’s BMI, an additional 10 hours of work per week by mothers, particularly for children between the ages of 3 and 11, was found to substantially increase the likelihood of children becoming obese. This risk was greatest among children of single working mothers.10 Unlike Musher-Eizenman et al’s research,9 a study in Japan found that maternal employment was not associated with an increase in children’s BMI even after adjusting for care by grandparents.11
Adding to this paradox, higher SES has been found to be associated with permissive parenting style. This parenting style, when parents relinquish their authority to their child in making decisions about eating and activity, has been shown to be related to an increased weight status among children.12–14
It is also well known that obesity occurs in nearly all ethnic and racial groups with some groups affected more than others.15–17 More specifically, results from the National Health and Nutrition Examination Survey have shown that Hispanic and non-Hispanic black children less than 11 years of age are at greatest risk for being overweight or obese; however, non-Hispanic white and non-Hispanic Asian children are less likely to become overweight or obese.16 These data support the unique variability in the contribution of income and ethnicity to childhood obesity and emphasize the importance of being culturally sensitive when addressing this issue.
Numerous studies have examined the relationships between childhood obesity, SES, and ethnicity, as well as issues associated with parenting.7–17 However, there are no known studies that have synthesized the data on the role of the parent in the development of childhood obesity or discussed the implications for health programs and policy. Thus, the purpose of this integrative review was to focus on identifying and describing parent roles, which may be related to the development of obesity in children and to suggest implications for health programs and policies.
Methods
An integrative review method was selected to accommodate the variety of methodologies used in the research that presented in this search.18
Search criteria
Inclusion criteria
Since the goal of this integrative review was to describe the parental role in child eating and activity behaviors as it relates to obesity, the focus of the search was on empirical evidence including descriptive and predictive research studies. Research with parents of children or with parents and children were included. Children were defined as those aged 0−12 years of age. Finally, due to the large number of articles presenting in the initial review process, the authors agreed that focusing on child weight or childhood obesity as an outcome was appropriate to further narrow the search.
Exclusion criteria
Randomized controlled trials, intervention studies, reviews, and theoretical publications were eliminated from the search. Studies addressing adolescents were also eliminated.
Search strategy and review process
Literature searches were conducted in Cumulative Index to Nursing and Allied Health Literature, the Cochrane Review, PsycINFO, PubMed, and the Web of Science between April and June 2014. Key search terms included: parent, role model, eating, activity, selected synonyms (eg, provider, feeding) and childhood overweight/obesity (Table 1). The initial search resulted in 993 publications (Figure 1). Applying the inclusion and exclusion criteria 918 publications including duplicates were eliminated. Lateral searches were conducted from the remaining 75 publications in the initial search, producing an additional 104 articles. Criteria used to review the initial search were applied to the lateral search, resulting in 56 publications. The first two authors reviewed publications from the combined searches (n=131) for themes relevant to the aim of the manuscript. The themes that emerged from these studies included parenting style, parent influence on feeding, self-efficacy, modeling, concern, and bidirectional influence resulting in 59 publications. To meet the purpose of this review, subsequent screening for empirical research that included child weight or BMI as an outcome further narrowed the search to 19.
 | Table 1 Search process |
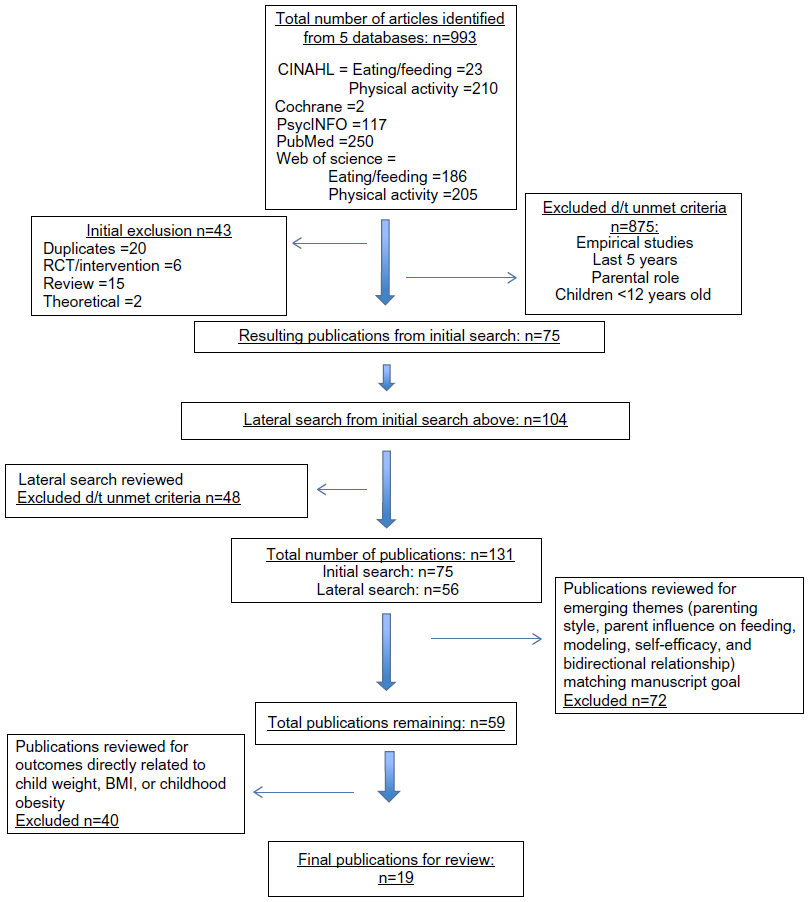 | Figure 1 PRISMA flow diagram for selecting studies. |
Results
Table 2 summarizes the articles included in this integrative review. Most of the studies were quantitative; only two qualitative studies emerged.19,20 Most of the participants in these studies were mothers (n=15). Three studies referred to the participant as a parent or caregiver, but did not specify sex.19,21,22 Six studies identified fathers as participants.23–28 The review includes studies conducted in Australia, Brazil, the Netherlands, Great Britain, and United States, representing diverse ethnic groups, which included Non-Hispanic White, African American, Hispanic, and Mexican American. Various socioeconomic backgrounds were also represented. Six themes emerged from this integrative review: parenting style, parent influence on feeding, self-efficacy, modeling, concern, and bidirectional influence. These themes are discussed in greater detail below.
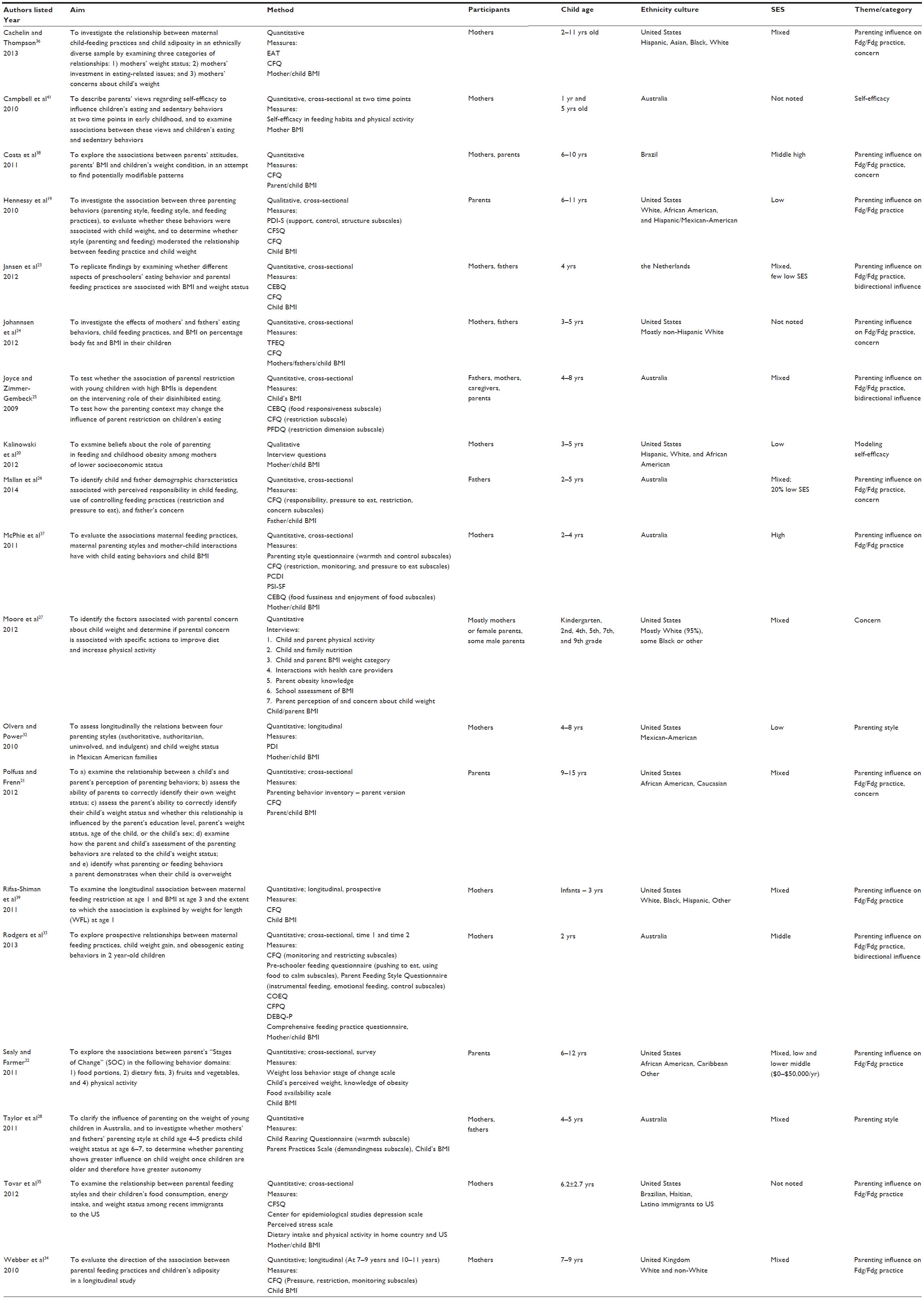 | Table 2 Summary of studies on parent role related to child overweight or obesity (n=19) |
Parenting style
Parenting style generally refers to patterns of parenting that include the degree of involvement and strictness or responsiveness and demandingness, which a parent uses when interacting with his or her child.29,30 Parenting style typologies include: authoritative, authoritarian, indulgent, and neglectful or uninvolved.29 Parenting practices occur in the context of parenting style and involve the actions that parents take in making decisions or interacting with their children. In other words, parenting style refers to the approach or the way that a parent interacts with his or her child; parenting practices refer to the specific behaviors enacted when carrying out the parental role.
In the past, parenting style has been suggested to strongly influence child weight outcomes.31 Yet, more recently, the association between parenting style and childhood obesity has been inconsistent across cultures. Over the past 5 years very little research has been conducted that addresses the association between parenting style and a child’s weight status. In this integrative review, parenting style and its association with childhood obesity and/or children becoming overweight emerged as a focus in two studies. The limited research that presented in our review suggests that parenting style continues to have little influence on the weight status of preschool- and school-age children less than 12 years old.28,32 To illustrate, Taylor et al’s work with mothers and fathers of 4−5 year-old children from Australia suggested that maternal or paternal parenting style may have little influence on child weight status, yet paternal responsiveness and demandingness may contribute to an increased risk for being overweight.28 On the other hand, in a sample of Mexican American families, Olvera and Power found that indulgent mothers were significantly more likely than authoritative or authoritarian families to have children who became overweight or obese.32
Parent influence on feeding
Despite the limited relationship between parenting style and a child’s weight status, parents and the practices that they use have been shown to play an important role in the development of children’s eating behaviors and patterns. Studies in our search focused on feeding practices, parental feeding style, and the socio-emotional climate of the interaction between the parent and child during the feeding/eating experience. Feeding practices were described as specific behaviors employed by parents to manage their child’s dietary intake. These independent, yet mutual practices include control, monitoring, restriction, and pressure.21,23,33,34 Parental feeding styles, like parenting styles, referred to parental demandingness or responsiveness as approaches specifically related to feeding.19,35 For example, an indulgent feeding style (ie, in which the parent allows the child to eat whatever they want, whenever they want) has been found to be associated with higher BMI among children.19 Other terms that researchers have used to describe parents’ influence on eating include, rejection, coercion, and chaos, or warmth responsiveness, structure, and autonomy. These terms reflect the respective negative or positive context of parenting (eg, emotional climate, predictability of the environment, and family routines) that may influence the interaction between the parent and child during feeding and eating.25 Parent influence on feeding, reflected by the behaviors of control, monitoring, pressure to eat, and restriction is further described below.
Control
Five studies explored the feeding practice of control; that is, parental management of when, where, and what children eat.21,24,33,36,37 The use of control, the manner in which it is used, and its influence on a child’s BMI has been shown to vary across cultures and age groups. In a study of 222 toddlers (mean age =2.03 years), researchers proposed that control may be direct or overt, as well as covert.33 Researchers found that African American parents used control more than White parents in managing food intake with their school-age children.21 Given this, it has been suggested that control may interfere with the ability of school-age children to self-regulate food intake.21
Control has also been shown to be negatively associated with maternal weight status. For example, Hispanic and Black mothers who were heavier used less control with their children (2 to 11 years old).36 In contrast, an association of using more control was found with fathers who had daughters aged 2–5 years old with higher BMIs.24 Overall, control has been found to be associated with higher BMI among toddlers and school-age children,21,33 and predictive of BMI in White school-age children,21 but not Australian preschool-age children,37 or Black or Hispanic children.36
Monitoring
Monitoring, another feeding practice, refers to parental tracking of the amount and type of food consumed by children.19,21,22,33,34,37,38 Monitoring has had mixed associations with parental weight and a child’s BMI. Comparing monitoring to control, Costa et al found that monitoring did not differ between parents who were of healthy weight or those who were obese.38 But like control, monitoring was inversely related to 2-year-old children’s acceptance of food and tendency to overeat,33 and positively associated with 2 to 4-year-old children’s BMI.37 Unlike these results, Hennessy et al found neither an association with feeding style nor a moderating effect between feeding style, monitoring, and the weight of White, African American or Mexican rural school-age (6−11 years old) children.19 However, monitoring has been shown to be used more frequently with British school-age (7−9 years old) children who had a higher BMI.34 Interestingly, investigators found that parental use of monitoring decreased over a 3 year period in school-age children who had a larger waist circumference and a higher fat mass index. By the end of the study, monitoring was not associated with the child’s BMI.34
Pressure to eat
Pressure to eat refers to parental behaviors or practices compelling children to eat certain foods.19,21,23,25,26,33,34,37–39 Like monitoring, pressure to eat has not been found to be consistently associated with eating and feeding or outcomes of a child’s weight status. The parental behavior of pressuring children to eat certain foods has been found to be similar between parents of healthy and obese weight status.38 Researchers found that pressure to eat was positively associated with a demanding feeding style among children from the United States,19 and with responsiveness to satiety among Dutch children.23 Yet, maternal pressure to eat had a negative effect on Australian preschool-age (2−4 years old) children’s enjoyment of food.28,37 Pressure to eat was also negatively associated with BMI among Dutch23 and Australian37 children’s BMI. However, pressure to eat was shown to be used less by British parents of children who had high BMI and fat mass indexes over a 3 year period.34
Restriction
Unlike pressure to eat, restriction refers to parental behaviors or practices to limit access to or limit the amount and type of food the child consumes.19,21,23,26,33,34,38,39 Overall, the influence of restriction on feeding and children’s BMI over short periods of time appears to have a negative influence; however, its use over long durations of time has little effect. Restriction scores were found to be higher in Brazilian parents who were heavier.38 In addition, restriction was more likely to be used by younger, less educated and non-White mothers from lower incomes,39 and Australian fathers who were concerned about their young children’s (2−5 years old) weight.26 Restriction was also negatively associated with a responsive feeding style,19 and positively associated with coercion and chaos.25 As such, restriction was positively related to 4 to 8-year-old children’s BMI.23,33,38 Furthermore, Joyce and Zimmer-Gembeck found that parental BMI and chaos partially mediated the relationship between restriction and children’s BMI in this age group.25 Joyce and Zimmer-Gembeck also found that the relationship between restriction and children’s disinhibited eating increased with an increase in parental use of coercion and family chaos.25
Like pressure to eat, parental use of restriction was shown to diminish over a 3 year period. However, the reduction in restriction was not related to a higher BMI or fat mass index like pressure to eat. In addition, no long-term association was found between restriction and child BMI.34 Collectively, restriction and pressure to eat have been suggested to influence dietary intake and interfere with the child’s ability to regulate food intake;21 however, none of these maternal feeding practices have been associated with a change in adiposity over time.24
Self-efficacy
Self-efficacy is a concept used to describe and understand the relationship between an individual’s knowledge and confidence in completing a task.40 If a person reports high confidence about their ability to perform a certain task, then he or she is described as having high self-efficacy for that skill. Two studies were found that described maternal confidence related to their child’s feeding and activity. One, a quantitative study, aimed to describe the differences in toddlers and preschool-age children’s specific eating and sedentary behaviors, and parents’ views regarding their capacity to influence these behaviors during these two periods of early childhood.41 While in another, a qualitative study, mothers described their own confidence in feeding their child.20
Campbell et al measured maternal self-efficacy in four specific domains: 1) promoting healthy eating in children, 2) limiting children’s consumption of non-healthy foods, 3) promoting children’s physical activity to displace viewing TV/DVD/video, and 4) limiting children’s TV viewing.41 The authors found that mothers reported high confidence in their ability to promote healthy eating and encourage physical activity in their toddlers (average age 15 months). However, the mothers of preschool children (5 year-olds) reported significantly less confidence in their ability to limit the child’s consumption of non-healthy foods and TV viewing.
Kalinowski et al conducted individual interviews with mothers of preschool-aged children (3−5 years old) to determine their beliefs about mother’s role in feeding and childhood obesity.20 These mothers reported being confident in their ability to meet their child’s food requests and to create a positive environment in the home around mealtime and food. They described indulgent feeding styles and admitted to using food to create a positive relationship with their children. Mothers highly valued pleasing their children and believed that this allowed for a better maternal-child relationship. In contrast, the confidence reported by Campbell et al was specifically related to pre-defined food groups that were labeled as healthy or non-healthy.41
Modeling
Parental role modeling of healthy eating and activity behavior has been viewed as an important social and environmental factor related to the eating and activity behavior of children.42 Both parental self-report and child report methods have been used for measuring parental eating and activity behaviors. Due to the lack of consistent measurement, a clear understanding of the influence of parental role modeling on eating and activity behaviors of children has not yet emerged. One study was found in this review related to parental role modeling.
Kalinowski et al’s research presented an interesting dichotomy of maternal perception in the role of parents in childhood feeding and obesity.20 When describing their own feeding practices, mothers valued providing foods that their children liked and described this as a positive, indulgent feeding practice. However, when asked to share their perceptions about what caused obesity in children, the majority of the mothers stated that parents were at fault when children were overweight. They believed that childhood obesity and children being overweight was due to inept (versus indulgent) or neglectful parenting. In addition, examples of parents’ role modeling unhealthy behaviors, such as the parent sleeping until noon or watching TV all day, were reported as contributing to childhood obesity by setting poor examples of a healthy lifestyle.
Concern
It has been hypothesized that feeding behaviors or practices may develop in response to parental concern for their child’s weight or their child’s approach and responsiveness to food, satiety, or food avoidance (fussiness).21,23 Concern was discussed in six studies.21,22,24,26,36,38 Hispanic, Black, Asian, and White mothers who had greater concern about the weight of their 2 to 11 year-old children were found to use more control in managing their child’s food intake. This was particularly noted in Hispanic mothers who had higher BMIs.36 Like Hispanic mothers, Australian parents who were heavier scored higher on concern for their child’s weight and their use of restriction.38 These same parents who were from lower economic status were found to be more concerned about their child’s weight than parents who were from higher economic status.38 Fathers who were concerned about their 4 year-old daughters’ higher body fat content and future health were found to use more control in managing their child’s caloric intake.24 In comparison, fathers who were concerned about their 2 to 5 year-old child becoming overweight were shown to use a moderate amount of pressure to eat and a high amount of restriction.26 Unlike parents with young children, African American and White parents who were concerned about their school-age child’s weight used more monitoring.21 In contrast, Sealy and Farmer found no association between parents’ concern and readiness to change in managing their children’s weight status.22
Concern also presented when parents were overseeing their child’s physical activity. Moore et al found that parents who were concerned about their child’s weight limited their screen time and took measures to increase their physical activity.27 However, there was no difference between parents who were concerned and those who were not concerned about their child’s weight when it came to enrolling their child in an organized activity.27
Bidirectional influence
Although parents play a key role in the development of healthy behaviors in children and are instrumental in influencing their behavior, it is important to note that a direct linear or causal relationship between parents and the onset of obesity in children is difficult to confirm. Thus, consideration of bidirectional interaction is important in the parent-child relationship, where successful or unsuccessful interactions drive subsequent interactions and future responses.43 This bidirectional interaction has been studied in the context of self-efficacy,43 and may help explain the interaction between parent and child related to eating and activity behaviors.25 Overall, children’s behaviors can influence parenting in a similar way that parenting behaviors shape children’s behaviors.
Rodgers et al examined the reciprocal relationship between children’s eating behaviors and maternal feeding practices with mother-child (2-year-old) dyads.33 They found that maternal feeding practices became more rigid when children tended to overeat. They also found that mothers indirectly controlled their child’s eating behavior when the child ate in response to their emotions. Additionally, this complex interchange between child (2 to 4 year-olds) eating and parent feeding practices and the association with the child’s BMI was supported by Jansen et al.23 The parent practice of restricting food or pressuring the child to eat correlated with the child’s responsiveness to food and eating behavior, but not consistently. For instance, children whose parents limit excessive food intake, may overeat when access to food is not restricted.23
The complexity of the parent-child relationship as it relates to child weight might also be explained by the mediating effect of the child’s eating behavior. Partial mediation was found by a child’s disinhibited eating behavior and its relationship between restrictive parenting and child weight.25
Discussion
The aim of this integrative review was to synthesize the data on parental role in relationship to the development of childhood obesity. Six themes emerged focusing on parenting style, parents’ influence on feeding practice (control, monitoring, pressuring to eat, and restricting), self-efficacy, modeling, and concern. Parental concern was linked to specific feeding practices, which in turn, may be related to childhood obesity. Parental restriction and pressure to eat or not eat certain foods were found to negatively affect children’s weight status.
This integrative review further highlights the complexity in the interaction between behavior, socioeconomic, and ethnic factors as they contribute to the development of childhood obesity. In addition, human behavior such as parenting styles and practices results from the reciprocal or bidirectional interaction between the parent and child.44 Parenting style reflects an approach used by adults when interacting with their child.6 To further clarify, parenting style is not static nor is the behavior of children. In other words, the style a parent uses may vary from one situation to the next. For example, a parent may be described as being authoritative; however, when presented with an unsafe situation, the parent may use an authoritarian approach. Thus the need to adapt their parenting approach may create difficulty in capturing which parenting style clearly contributes to children being or becoming obese.
Compared to parenting style, parent feeding practices have been found to play an important role in the development of children’s eating behaviors and patterns. Specific behaviors such as restriction and pressure to eat have been found to be negatively associated with children’s BMI.19,21,23,25,33,34,37–39 In contrast, control and monitoring have been shown to influence the child’s acceptance and self-regulation of food intake; however, their relationship to the child’s weight status is equivocal.19,21,23,24–26,33,34,36–39
Unlike parent feeding practices, far fewer studies have examined the effects of parenting feeding styles and the context of parenting during feeding. As a result, outcomes related to these behaviors or their potential moderating effect are less well understood. However, demanding feeding style has been shown to be associated with pressure to eat,19 and restriction has been negatively associated with parental responsiveness and children’s weight status.25
Given this evidence regarding parent influence on feeding, future studies examining the combined effect of feeding practices, feeding style, and the context of the family may be helpful in identifying variables or interactions between variables to explain the development of childhood obesity. Asking parents what they believe to be most challenging with regard to mealtimes, (ie, feeding their child, how they approach feeding, or the family overtones) may help direct providers and parents in developing strategies to address these issues. Longitudinal studies to clarify the effect that growth and development have on these variables may also be helpful.
Concern, a psychological state that may motivate behavior, has been found to be associated with a variety of parental responses. In general, concern has been associated with all parental feeding practices, (ie, control, restriction, pressure to eat, and monitoring). Although concern may motivate behavior, it has not been found to be associated with readiness to change even when children and families are undergoing treatment for childhood obesity.22
Concern was also evident when mothers were asked about their confidence or self-efficacy in their ability to provide food for their child. Mothers were concerned about establishing a healthy positive relationship with their children. They reported being confident in their ability to please their child at mealtime; while, at the same time, building a stronger bond with their child.41 However, the mothers’ focus on pleasing their child may interfere with their ability to realize that unhealthy food choices may in fact negatively influence weight and health status. In addition, mothers reported feeling more confident when feeding their infants or toddlers and reported less confidence as their children became autonomous.41
These results highlight the need for program evaluators to be very specific when asking mothers to report on their confidence in promoting healthy behaviors for their child at mealtime. The concept of self-efficacy could be defined as either confidence in promoting healthy food choices and activity or confidence in establishing a positive parent-child relationship. Inconsistency of self-report may help explain why there has been lack of conclusive evidence that any one specific parenting intervention has been more effective than another in the treatment of childhood obesity.4
These results have clinical implications when working with mothers of young children. Mothers may need to be reassured that they will still have a healthy loving relationship with their child even when they provide limits on less healthy food choices and encourage healthier food options. Furthermore, strategies could be designed for parents of young children to use with their child as they develop more independence. For example, instead of asking a 5 year-old child if he or she wants to have fruit, the parent could be taught to ask the child to choose an apple or orange. This approach may facilitate the development of making healthy choices.
As with confidence or self-efficacy, parental perception becomes an important factor when trying to examine role-modeling. For instance, mothers were able to identify that poor role-modeling or inept parenting by others contributed to childhood obesity; but, when they reflected upon their own role, they saw themselves as being a good and indulgent parent. In addition, mothers did not discuss the possible influence of being indulgent and pleasing their child at mealtime as it related to their child’s weight or health status.20 As stated above, it will be important for health care providers to be sensitive to parental concern about being “good” and loving parents; while at the same time, being able to guide their children in making healthy eating and activity choices.
Strengths and limitations
This review includes research that has been conducted in multiple countries providing rich information regarding the influence of parents, culture, and SES on the development of childhood obesity. Numerous validated measures were used to explore parental role in childhood obesity supporting the complexity of this multifactorial issue. Additionally, most of the articles focused on parental role in influencing a child’s eating behavior.
Furthermore, findings from our integrative review support recommendations from the American Heart Association reinforcing that families should take a positive approach with their children by watching portion sizes versus restricting foods and modeling healthy eating habits.45
Interestingly, there was a paucity of 1) longitudinal studies and 2) research addressing parent role in promoting physical activity. In addition, no literature emerged regarding children’s self-esteem despite the abundance of literature describing the relationship between children’s self-esteem and body weight.44,46–49 The lack of studies that presented in the last 5 years on these topics suggests the need for additional research within and across various cultures so that health care providers have stronger evidence for effective program and policy development.
In addition, findings varied across cultures and were reported to have a minimal effect over time as children became older. These inconsistencies in results may be due to the variations in children’s ages that presented across the studies reviewed (Table 2). Developmentally, children behave differently as toddlers, preschool-age, and school-age children. These developmental variations in children elicit different responses from parents and emphasize the importance of considering the bidirectional nature of their interaction. The variety of cultures presented in this review may have also contributed to inconsistent results. There is an insufficient number of studies presented in this review to determine if findings were consistent within cultures.
Implications for health programming and policy
Current national health policy in the United States has focused on promoting healthy behaviors in the school environment by improving the nutritional quality of school lunches, removing vending machines, and providing opportunities for physical activity.50 Evidence from this review supports the development of programs focusing on parents in their role related to eating and activity using a family focused approach. For instance, health programs may need to focus on assisting parents to understand their children’s eating behaviors and to reflect on their own feeding practices.51 Programs to build parental self-confidence in light of their child’s health may also be beneficial. In one longitudinal study, the children of families who participated in a family intervention that promoted effective parenting skills in early childhood had significantly lower rates of obesity as they approached adolescence compared to children in the control group.52 A collaborative approach between health care providers, parents, and children is important in guiding families to successfully adopt healthier eating and activity behaviors. A summary of recommendations to enhance the parent role in decreasing the risk of childhood obesity for health care providers and parents has been extrapolated from this integrative review and can be found in Table 3.
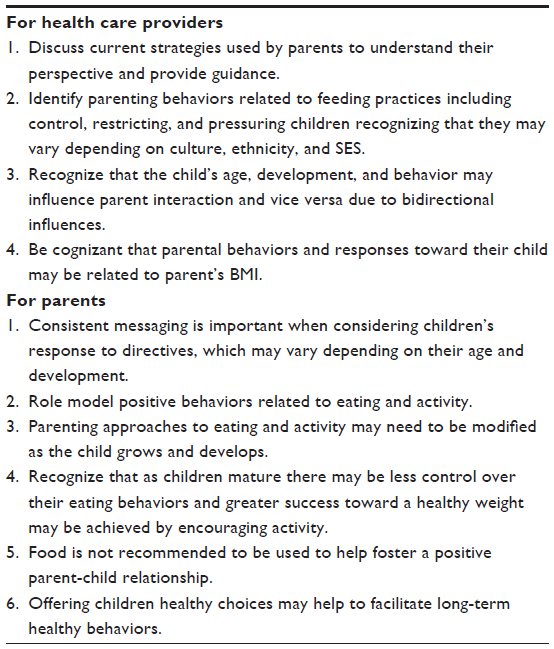 | Table 3 Recommendations |
Conclusion
The complexity in the interaction between parenting style, influence on feeding, concern, self-efficacy, and modeling combined with SES and ethnicity creates a challenge in guiding parents and developing health programs and policies to remedy childhood obesity. Successful program implementation must consider the bidirectional relationship between parents as agents of change and their children. These challenges present opportunities to gain further understanding of this dynamic relationship and trial new strategies.
Acknowledgments
Special thanks to Patricia Morel, BSN student, University of Pittsburgh, School of Nursing for assistance with formatting and to Brian Greene, University of Pittsburgh, School of Nursing, Center for Research and Evaluation for editorial support.
Disclosure
The authors have no personal financial interest in this work, no commercial sponsors, and no conflicts of interest.
References
de Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92(5):1257–1264. | |
World Health Organization. Population-Based Approaches to Childhood Obesity Prevention. Geneva: World Health Organization; 2012. Available from: www.who.int/dietphysicalactivity/childhood/WHO_new_childhoodobesity_PREVENTION_27nov_HR_PRINT_OK.pdf. Accessed July 28, 2014. | |
Davison KK, Birch LL. Childhood overweight: A contextual model and recommendations for future research. Obes Rev. 2001;2(3):159–171. | |
Hoghughi M. Parenting – An introduction. In: Hoghughi M, Long N, editors. Handbook of Parenting: Theory and Research for Practice. London: Sage Publications; 2004:1–18. | |
Faith MS, Van Horn L, Appel LJ, et al. Evaluating parents and adult caregivers as “Agents of Change” for treating obese children: Evidence for parent behavior change strategies and research gaps. Circulation. 2012;125(9):1186–1207. | |
Golan M, Weizman A, Aptar A, Fainaru M. Parents as the exclusive agents of change in the treatment of childhood obesity. Am J Clin Nutr. 1998;67(5):1130–1135. | |
Crawford PB, Story M, Wang MC, Ritchie LD, Sabry, ZI. Ethnic issues in the epidemiology of childhood obesity. Pediatr Clin North Am. 2001;48(4):855–878. | |
Ziol-Guest KM, Duncan GJ, Kalil A. Early childhood poverty and adult body mass index. J Public Health. 2009;99(3):527–532. | |
Musher-Eizenman DR, de Lauzon-Guillain B, Houb SC, Leporc E, Charles M. Child and parent characteristics related to parental feeding practices. A cross-cultural examination in the US and France. Appetite. 2009;52(1):89–95. | |
Courtemanche C. Longer hours and larger waistlines? The relationship between work hours and obesity. Obesity. 2009;12(2):1–33. | |
Watanbee E, Lee JS, Kawakubo K. Associations of maternal employment and three-generation families with pre-school children’s overweight and obesity in Japan. Int J Obesity (Lond). 2011;35(7):945–952. | |
Lane SP, Bluestone C, Burke CT. Trajectories of BMI from early childhood through early adolescence: SES and psychosocial predictors. Br J Health Psychol. 2013;18(1):66–82. | |
Semmler C, Ashcroft J, van Haarsveld C, Carnell S, Wardle J. Development of overweight in children in relation to parental weight and socioeconomic status. Obesity (Silver Spring). 2009;17(4):814–820. | |
Topham GL, Page MC, Hubbs-Tait L, et al. Maternal depression and socio-economic status moderate the parenting style/child obesity association. Public Health Nutr. 2010;13(8):1237–1244. | |
Flegal KM, Ogden CL, Yanovski JA, et al. High adiposity and high body mass index-for age in US children and adolescents overall and by race-ethnic group. Am J Clin Nutr. 2010;91(4):1020–1026. | |
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA. 2014;311(8):806–814. | |
Ogden CL, Lamb MM, Carroll MD, Flegal KM. Obesity and socioeconomic status in children and adolescents: United States, 2005–2008. NCHS Data Brief. 2010;51:1–8. | |
Whittemore R, Knafl K. The integrative review: Updated methodology. J Adv Nurs. 2005;52(5):546–553. | |
Hennessy E, Hughes SO, Goldberg JP, Hyatt RR, Economos CD. Parent behavior and child weight status among a diverse group of underserved rural families. Appetite. 2010;54(2):369–377. | |
Kalinowski A, Krause K, Berdejo C, Harrell K, Rosenblum K, Lumeng JC. Beliefs about the role of parenting in feeding and childhood obesity among mothers of lower socioeconomic status. J Nutr Educ Behav. 2012;44(5):432–437. | |
Polfus M, Frenn M. Parenting behaviors of African American and Caucasian families: Parent and child perceptions, associations with child weight, and ability to identify abnormal weight status. J Pediatr Nurs. 2012;27(3):195–205. | |
Sealy YM, Farmer GL. Parents’ stage of change for diet and physical activity: Influence on childhood obesity. Soc Work Health Care. 2011;50(4):274–291. | |
Jansen PW, Roza SJ, Jaddoe VW, et al. Children’s eating behavior, feeding practices of parents and weight problems in early childhood: Results from the population-based Generation R Study. Int J Behav Nutr Phys Act. 2012;9:130. | |
Johannsen DL, Johansen NM, Specker BL. Influence of parent’s eating behaviors and child feeding practices on children’s weight status. Obesity. 2012;14(3):431–439. | |
Joyce JL, Zimmer-Gembeck MJ. Parent feeding restriction and child weight. The mediating role of child disinhibited eating and the moderating role of the parenting context. Appetite. 2009;52(3):726–734. | |
Mallan KM, Daniels LA, Nothard M, et al. Dads at the dinner table. A cross-sectional study of Australian fathers’ child feeding perceptions and practices. Appetite. 2014;73:40–44. | |
Moore LC, Harris CR, Bradlyn AS. Exploring the relationship between parental concern and the management of childhood obesity. Matern Child Health J. 2012;16(4):902–908. | |
Taylor A, Wilson C, Slater A, Mohr P. Parenting and child body mass index: Longitudinal investigation of maternal and paternal influence. Aust J Psychol. 2011;63(4):198–206. | |
Darling N, Steinberg L. Parenting style as context: An integrative model. Psychol Bull. 1993;113(3):487. | |
Hughes SO, Power TG, Fisher O, Mueller J, Nicklas TA. Revisiting a neglected construct: Parenting styles in a child-feeding context. Appetite. 2005;44(1):83–92. | |
Rhee KE, Lumeng JC, Appugliese DP, Kaciroti N, Bradley RH. Parenting styles and overweight status in first grade. Pediatrics. 2006;117(6):2047–2054. | |
Olvera N, Power TG. Brief report: Parenting styles and obesity in Mexican American children: A longitudinal study. J Pediatr Psychol. 2010;35(3):243–249. | |
Rodgers RF, Paxton SJ, Massey R, et al. Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: A prospective study. Int J Behav Nutr Phys Act. 2013;10:24. | |
Webber L, Cooke L, Hill C, Wardle J. Child adiposity and maternal feeding practices: A longitudinal analysis. Am J Clin Nutr. 2010;92(6):1423–1428. | |
Tovar A, Hennessy E, Pirie A, et al. Feeding styles and child weight status among recent immigrant mother-child dyads. Int J Behav Nutr Phys Act. 2012;9:62. | |
Cachelin FM, Thompson D. Predictors of maternal child-feeding practices in an ethnically diverse sample and the relationship to child obesity. Obesity (Silver Spring). 2013;21(8):1676–1683. | |
McPhie S, Skouteris H, McCabe M, et al. Maternal correlates of preschool child eating behaviours and body mass index: A cross-sectional study. Int J Pediatr Obes. 2011;6(5–6):476–480. | |
Costa FS, Del Pino DL, Friedman R. Caregivers’ attitudes and practices: Influence on childhood body weight. J Biosoc Sci. 2011;43(4):369–378. | |
Rifas-Shiman SL, Sherry B, Scanlon K, Birch LL, Gillman MW, Taveras EM. Does maternal feeding restriction lead to childhood obesity in a prospective cohort study? Arch Dis Child. 2011;96(3):265–269. | |
Bandura A. Self-Efficacy: The Exercise of Control. New York, NY: WH Freeman; 1997. | |
Campbell K, Hesketh K, Silverii A, Abbott G. Maternal self-efficacy regarding children’s eating and sedentary behaviours in the early years: Associations with children ’s food intake and sedentary behaviours. Int J Pediatr Obes. 2010;5(6):501–508. | |
Hood MY, Moore LL, Sundaragan-Ramamurti A, Singer M, Cupples LA, Ellison RC. Parental eating attitudes and the development of obesity in children. The Framingham children’s study. Int J Obes Relat Metab Disord. 2000;24(10):1319–1325. | |
Soliday E. Parenting and children’s physical health. In: Hoghughi M, Long N, editors. Handbook of Parenting: Theory and Research for Practice. London: Sage Publications; 2004:161–180. | |
McAlister AL, Perry CL, Parcel GS. How individuals, environments, and health behaviors interact. In: Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice. San Francisco: Jossey-Bass; 2008:169–188. | |
American Heart Association. Policy Position Statement on the Prevention, Assessment, Diagnosis and Treatment of Child and Adolescent Obesity in the Healthcare Environment. Available from: https://www.heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloadable/ucm_428437.pdf. Accessed November 1, 2014. | |
Hesketh K, Wake M, Waters E. Body mass index and parent-reported self-esteem in elementary school children: Evidence for a causal relationship. Int J Obes Relat Metab Disord. 2004;29(10):1233–1237. | |
French SA, Story M, Perry CL. Self-esteem and obesity in children and adolescence: A literature review. Obes Res. 1995;3(5):479–490. | |
Franklin J, Denyer G, Steinbeck KS, Caterson ID, Hill AJ. Obesity and risk of low self-esteem: a statewide survey of Australian children. Pediatrics. 2006;118(6);2481–2487. | |
Davison KK, Birch LL. Weight states, parent reaction, and self-concept in five-year-old girls. Pediatrics. 2001;107(1):46–53. | |
letsmove.gov [homepage on the Internet]. Let’s Move. America’s Move to Raise a Healthier Generation of Kids. Available from: http://www.letsmove.gov/. Accessed September 7, 2014. | |
Clark HR, Goyder E, Bissell P, Black L, Peters J. How do parents’ child–feeding behaviours influence child weight? Implications for childhood obesity policy. J Public Health (Oxf). 2007;29(2):132–141. | |
Brotman LM, Dawson-McClure S, Huang KY, et al. Early childhood family intervention and long-term obesity prevention among high-risk minority youth. Pediatrics. 2012;129(3):e621–e628. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.