")
Back to Journals » Integrated Blood Pressure Control » Volume 7
No association between perfluoroalkyl chemicals and hypertension in children
Authors Geiger S, Xiao J, Shankar A
Received 4 May 2013
Accepted for publication 17 August 2013
Published 13 January 2014 Volume 2014:7 Pages 1—7
DOI https://doi.org/10.2147/IBPC.S47660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Sarah Dee Geiger,1 Jie Xiao,2 Anoop Shankar3
1Department of Public Health, Northern Illinois University, School of Nursing and Health Studies, DeKalb, IL, 2Registration and Records, North Carolina State University, Raleigh, NC, 3Department of Epidemiology, School of Public Health, West Virginia University, Morgantown, WV, USA
Background: Hypertension is a leading cause of cardiovascular disease worldwide. Perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS) are perfluoroalkyl chemicals (PFCs) used in the manufacture of common consumer products and detected in the blood of the majority of Americans. Emerging biological data suggest that PFC exposure may have a role in the development of hypertension. However, the association between PFCs and hypertension has not yet been explored in humans. Therefore, we examined this association in a representative sample of US children.
Methods: A cross-sectional study was performed on 1,655 children from the National Health and Nutrition Examination Survey, 1999–2000 and 2003–2008. The main outcome of interest was hypertension, defined as age, height, and sex specific systolic and/or diastolic blood pressure level at the 95th percentile.
Results: We found no association between serum levels of PFOA and PFOS and hypertension in either unadjusted or multivariable-adjusted analyses controlling for age, sex, race-ethnicity, body mass index, annual household income, moderate activity, total serum cholesterol, and serum cotinine. Compared with the lowest quartile, the multivariable-adjusted odds ratio (95% confidence interval) of hypertension in the highest quartile of exposure was 0.69 (0.41–1.17) for PFOA and 0.77 (0.37–1.61) for PFOS (all P-trend values >0.30).
Conclusion: Our findings indicate that exposure to PFOA or PFOS is not significantly associated with hypertension in children at the lower PFC exposure levels typical of the general population.
Keywords: perfluorooctanoic acid, perfluorooctane sulfonate, perfluoroalkyl chemicals, blood pressure, children
Introduction
Perfluoroalkyl chemicals (PFCs) are detectable in the blood of more than 98% of the US population.1 They persist in the environment, bioaccumulate, biomagnify along food chains, and have been shown to cause developmental, endocrine, and other adverse health outcomes in laboratory animals.2,3 PFCs are found in surfactants, lubricants, polishes, paper and textile coatings, food packaging, and fire-retarding foams, among many other consumer products. Perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS) are two of the most studied PFCs.
Hypertension is present in 29.0% of the adult US population and 3.2% of adolescents aged 11–17 years.4 It is also the leading cause of cardiovascular disease worldwide.5 Hypertension accounted for 56.5% of all-cause mortality in 2006, and death rates from hypertension increased by 19.5% from 1996 to 2006.6 While traditional factors such as weight gain,7,8 smoking,9 and lack of physical activity10 have been shown to be positively associated with hypertension, emerging literature suggests a role for common environmental exposures, including other manmade organic compounds,11–15 in the development of hypertension.
A positive association between exposure to PFCs and hypertension is plausible. In a 2012 study, PFOA was reported to be linked to pregnancy-induced hypertension; this represents the only known epidemiologic study examining the association between PFOA and any form of high blood pressure.16 However, PFCs such as PFOA and PFOS have been linked to higher cholesterol levels,17 hyperuricemia,18,19 metabolic syndrome,20 insulin resistance,20 and high serum gamma-glutamyl transpeptidase29 in previous epidemiologic studies,21–24 all of which are factors reported to be independently related to hypertension.18,25–28 In vitro studies have shown PFC exposure to be associated with oxidative stress29,30 and endothelial dysfunction.31,32 To our knowledge, the association between PFCs and hypertension has not been explored in children. Therefore, we sought to examine the association between PFCs and blood pressure levels in children using data from the nationally representative National Health and Nutrition Examination Survey (NHANES).
Materials and methods
Study population
This study uses 8 years of merged data from the NHANES, years 1999–2000, 2003–2004, 2005–2006, and 2007–2008. PFC data were not available for years 2001–2002. Data collection methods for NHANES have been published and are available online.33 NHANES included a stratified multistage probability sample, representative of the noninstitutionalized civilian US population. Selection was based on counties, census blocks, households, and individuals within households, and included the oversampling of non-Hispanic Blacks and Mexican Americans in order to provide stable estimates of these groups. Subjects were required to sign a consent form before their participation, and approval was obtained from the Human Subjects Committee in the US Department of Health and Human Service. The survey also includes biomonitoring for select environmental chemicals, including PFCs, in a random one third subsample of participants by the National Center for Environmental Health.
The central variables for this analysis are laboratory measurements of PFOA, PFOS, and blood pressure, and the study sample consisted of children 18 years of age and younger who took part in both the interview and examination components. Because PFC levels are not sampled for children under the age of 12 years, the age range for this study was children 12–18 years (n=1,788). We additionally excluded those with missing values for covariates used in the multivariable model, including age, sex, race-ethnicity, annual household income, physical activity, total serum cholesterol, and serum cotinine (n=133). The final sample size of children included in this analysis was n=1,655.
Main outcome of interest: blood pressure
The main outcome of interest was systolic and diastolic blood pressure and the presence of hypertension. Blood pressure was measured in the examination component of the survey. The mean of up to three blood pressure readings was used for both systolic and diastolic blood pressure. Seated blood pressure was taken by a physician using a mercury sphygmomanometer following 5 minutes of rest according to American Heart Association and JNC7 (Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure) guidelines.34,35 Details of blood pressure measurement and quality control procedures are available online.36 Subjects were considered hypertensive if they had an average blood pressure level at the 95th percentile or greater, adjusted for age, height, and sex, as recommended by the National High Blood Pressure Education Program Working Group on Hypertension Control in Children and Adolescents.37,38
Exposure measurements
Sex, age, race/ethnicity, education level, physical activity, and annual household income were assessed by a standardized interview. Body mass index was calculated using the formula weight (kg)/height (m2). Moderate physical activity was defined as participation in any moderate recreational physical activity. NHANES participants also provided blood samples for various laboratory measurements. Details of blood collection and analysis are provided in the NHANES Laboratory/Medical Technologists Procedures Manual.39 Briefly, serum total cholesterol was measured enzymatically. Perfluoroalkyl chemicals were measured in serum by the National Center for Environmental Health using automated solid-phase extraction coupled with isotope dilution high-performance liquid chromatography-tandem mass spectrometry. Our study focused on PFOA and PFOS, two specific PFCs. Both were detected in the serum of over 98% of participants; values below the limit of detection were reported by NHANES as the limit of detection divided by the square root of 2.39
Statistical analysis
Serum PFOA and PFOS were analyzed as continuous and categorical variables. For analysis as a continuous variable, PFC values were log-transformed (base e) to correct skewed distributions. For analysis as a categorical variable, we categorized PFOA and PFOS into quartiles of increasing exposure. Linear regression models were used to examine mean change in blood pressure with increasing category of PFC, using the lowest PFC quartile as the referent. We ran two nested models: unadjusted and multivariable-adjusted, controlling for age (<18 years), sex (male, female), race-ethnicity (non-Hispanic White, non-Hispanic Black, Mexican American, other), body mass index (underweight, healthy weight, overweight, obese), annual household income categories (<$4,999, $5,000–$9,999, $10,000–$14,999, $15,000–$19,999, $20,000–$24,999, $25,000–$34,999, $35,000–$44,999, $45,000–$54,999, $55,000–$64,999, $65,000–$74,999, >$75,000), moderate activity (absent, present), and serum total cholesterol (mg/dL). We also ran unadjusted and multivariable-adjusted logistic regression models to calculate the odds ratio (95% confidence interval) of hypertension for each PFC quartile, using quartile 1 as the referent. Trends in the odds ratio of hypertension across increasing serum PFC quartiles were determined by modeling the PFCs as ordinal variables. In a series of supplemental analyses, we explored the possibility of a nonlinear relationship between PFOA, PFOS, and blood pressure levels. We conducted nonlinear regression modeling using the NLIN procedure.40,41
Sample weights that account for unequal probabilities of selection, oversampling, and nonresponse in the NHANES survey were applied for all analyses, as recommended by the National Center for Health Statistics.42 Analyses were conducted using SAS (version 9.2, SAS Institute Inc., Cary, NC, USA) software. Standard errors were estimated using the Taylor series linearization method.
Results
Characteristics of the study population (n=1,655) are shown in Table 1. Nearly half of the study population was female and the mean age of 15.1 years had a standard error of only ±0.1. The majority of the sample was non-Hispanic White, but Blacks (14.3%) and Mexican Americans (11.8%) were represented as well. Nearly half of study participants fell into the highest household income category and almost 37.0% of the children were overweight or obese.
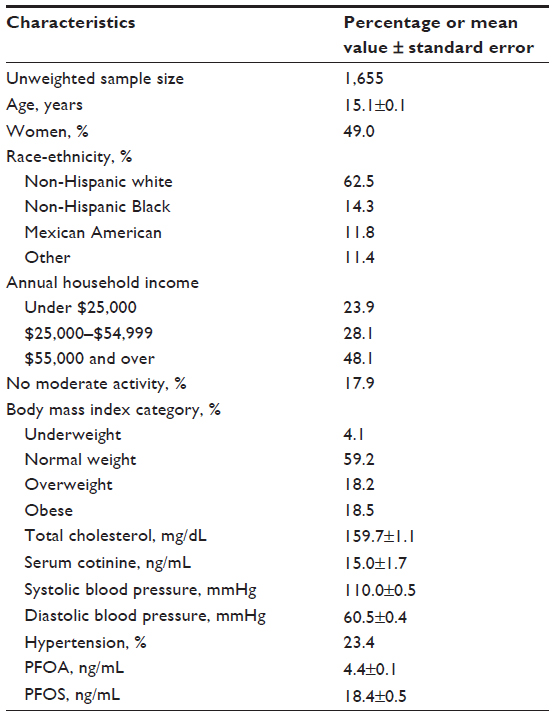 | Table 1 Characteristics of study population |
Our first multivariate analysis consisted of linear regression modeling to study the association between increasing quartiles of serum PFOA and PFOS and the mean change in serum systolic (Table 2) and diastolic (Table 3) blood pressure level in mmHg. The association between PFCs and blood pressure was not significant in either model (all P-trend values >0.30). The relationship was also not significant in either model for log-transformed PFOA or PFOS.
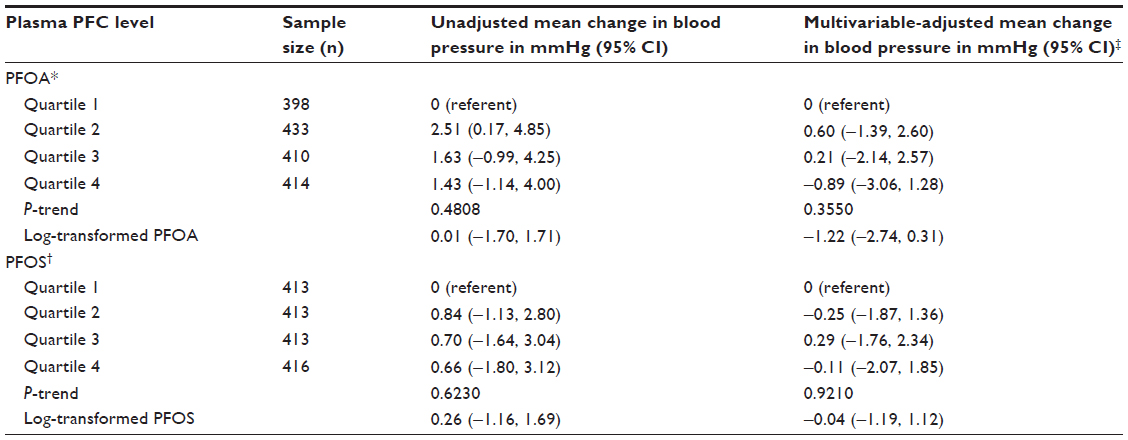 | Table 2 Association between serum PFOA, PFOS levels, and systolic blood pressure |
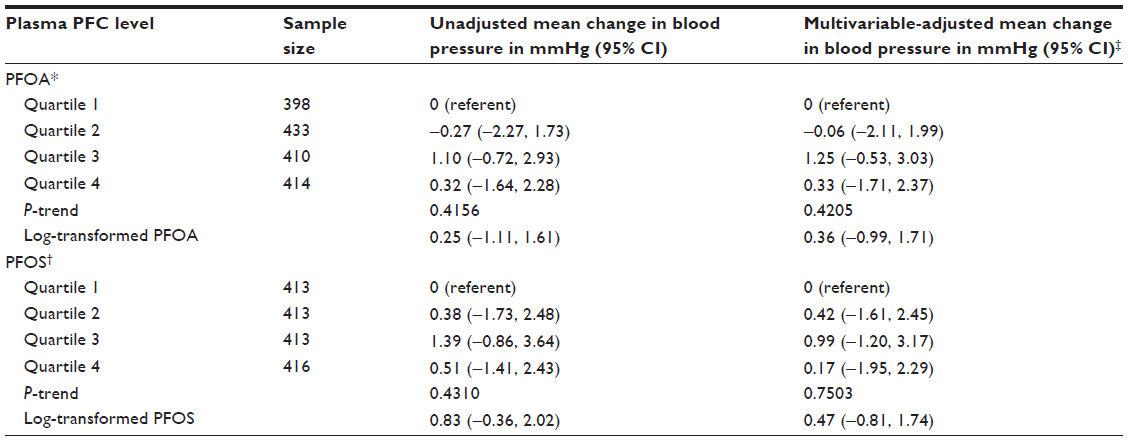 | Table 3 Association between serum PFOA, PFOS levels, and diastolic blood pressure |
In addition, we also analyzed the putative association between increasing quartiles of serum PFOA and PFOS and the presence of hypertension using logistic regression models (Table 4). Results were similar to those of the linear regression analysis in that we did not observe an association between PFOA or PFOS and hypertension in any model (all P-trend values >0.30). The relationship was also not significant in either model for log-transformed PFOA or PFOS.
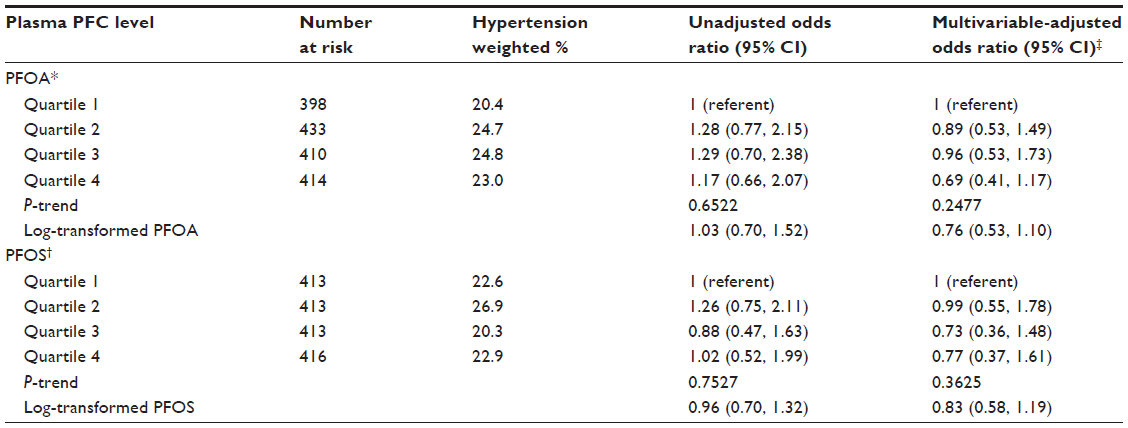 | Table 4 Association between plasma PFOA, PFOS levels, and hypertension |
Nonlinear regression analyses were consistent with linear and logistic regression modeling. No association was observed between PFOA or PFOS and blood pressure levels.
Discussion
We did not find a positive association between exposure to PFOA and PFOS and elevated blood pressure levels in a nationally representative sample of children. Multivariable models controlled for age, sex, race-ethnicity, body mass index, annual household income, physical activity, serum total cholesterol levels, and serum cotinine levels. Our analysis contributes to the extant literature by being the first to examine the association between PFC exposure and hypertension in humans.
Hypertension is a common condition which is also a strong, independent risk factor for cardiovascular disease.5 The pathophysiology of hypertension is incompletely understood, but several factors have been implicated, including psychosocial stress, excessive sodium-retaining hormone production, increased sympathetic nervous system activity, and vasodilator deficiency.43 Hypertension remains a major public health problem despite substantial advances in our understanding of its etiology, pathophysiology, and effective treatment.44
No previous study has examined the association between PFCs and hypertension. In relation to our hypothesis, one recent study analyzed the relationship between PFCs and pregnancy-induced hypertension, a condition of high blood pressure seen in pregnancy that can lead to potentially severe health risks to the mother as well as to the fetus.16 This study was conducted by a team of scientists who were appointed by the court to study the health effects of PFC exposure following litigations between DuPont Chemical Works and more than 69,000 plaintiffs exposed to high levels of PFOA in drinking water due to a chemical leak from this plant. This panel of scientists has recently publicly announced several findings, including a positive association between PFOA and pregnancy-induced hypertension; however, these findings have not yet been subjected to scientific peer review. In addition, there is indirect evidence supporting our hypothesis of a putative association between PFC exposure and hypertension.
Several factors that are known to be associated with increased risk of hypertension,25–27 including elevated cholesterol,28 hyperuricemia,19 oxidative stress,29,30 endothelial dysfunction,31 insulin resistance,20 weight gain,45 and elevated serum gamma-glutamyl transpeptidase,29 have been shown to be independently related to PFC exposure. Low-level exposure to PFCs has also been shown to be significantly associated with other health outcomes such as dyslipidemia,24 hyperuricemia,46 thyroid disease,47 and changes in liver enzymes,20 and therefore may be deleterious to public health even in the absence of an association with hypertension. Finally, high-level PFC exposure is known to be linked to a host of negative health outcomes, including dyslipidemia,17 hyperuricemia,19 early menopause,48 and osteoarthritis,49 among others. Despite these leads, our study did not find an association between PFC exposure and the presence of hypertension in a multiethnic, representative sample of children.
In a recent population-based study, Seals et al50 demonstrated that PFOA has a concentration-dependent half-life of 2.9 years at higher serum levels and 8.5 years at lower levels, suggesting that at lower serum levels PFCs persist in the body for a longer period of time. Given that PFCs are present in the blood of the majority of Americans only at low levels,3 the current study of the relationship between PFC exposure and hypertension in the representative NHANES sample renders our results to be more generalizable and relevant than studies from high PFC exposure groups, such as the study linking PFCs to pregnancy-induced hypertension.16 Also, children are an ideal sample in which to study environmental cardiovascular risk factors because there is now an emerging consensus that the development of cardiovascular disease in adulthood is preceded by metabolic changes occurring in childhood,51–53 and compared with adults, children tend to have limited cumulative exposure to lifestyle/behavioral risk factors for chronic diseases such as smoking and alcohol intake, and therefore the potential for confounding by these factors tends to be limited.
Other strengths of our study include its relatively large sample size, availability of detailed data on confounders, and standardized, high-quality data collection. The primary limitation is the cross-sectional nature of the study, which prohibits drawing conclusions about the temporal nature of the PFC-blood pressure association.
In summary, we found no association between serum PFC levels and blood pressure in a representative, multiethnic sample of US children. Results were consistent across regression models in separate analyses for PFOA and PFOS. Future research should be conducted to confirm or disprove our results.
Acknowledgment
This publication was made possible by grants from the National Institutes of Health (5T32 HL090610-04, 5R03ES018888-02).
Disclosure
The authors report no conflicts of interest related to this paper.
References
Calafat AM, Wong LY, Kuklenyik Z, Reidy JA, Needham LL. Polyfluoroalkyl chemicals in the US population: data from the National Health and Nutrition Examination Survey (NHANES) 2003–2004 and comparisons with NHANES 1999–2000. Environ Health Perspect. 2007;115(11):1596–1602. | |
Lau C, Anitole K, Hodes C, Lai D, Pfahles-Hutchens A, Seed J. Perfluoroalkyl acids: a review of monitoring and toxicological findings. Toxicol Sci. 2007;99(2):366–394. | |
Steenland K, Fletcher T, Savitz DA. Epidemiologic evidence on the health effects of perfluorooctanoic acid (PFOA). Environ Health Perspect. 2010;118(8):1100–1108. | |
McNiece KL, Poffenbarger TS, Turner JL et al. Prevalence of hypertension and pre-hypertension among adolescents. J Pediatr. 2007;150(6):640–644. | |
Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303(20):2043–2050. | |
Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: final data for 2006. Natl Vital Stat Rep. 2009;57(14):1–134. | |
Garrison RJ, Kannel WB, Stokes J III, Castelli WP. Incidence and precursors of hypertension in young adults: the Framingham Offspring Study. Prev Med. 1987;16(2):235–251. | |
Leitschuh M, Cupples LA, Kannel W, Gagnon D, Chobanian A. High-normal blood pressure progression to hypertension in the Framingham Heart Study. Hypertension. 1991;17(1):22–27. | |
Howard G, Wagenknecht LE, Burke GL, et al. Cigarette smoking and progression of atherosclerosis: the Atherosclerosis Risk in Communities (ARIC) Study. JAMA. 1998;279(2):119–124. | |
Nelson L, Jennings GL, Esler MD, Korner PI. Effect of changing levels of physical activity on blood-pressure and haemodynamics in essential hypertension. Lancet. 1986;2(8505):473–476. | |
Chen Y, Factor-Litvak P, Howe GR, et al. Arsenic exposure from drinking water, dietary intakes of B vitamins and folate, and risk of high blood pressure in Bangladesh: a population-based, cross-sectional study. Am J Epidemiol. 2007;165(5):541–552. | |
Hu H, Aro A, Payton M, et al. The relationship of bone and blood lead to hypertension. The Normative Aging Study. JAMA. 1996;275(15):1171–1176. | |
Park SK, Mukherjee B, Xia X, et al. Bone lead level prediction models and their application to examine the relationship of lead exposure and hypertension in the Third National Health and Nutrition Examination Survey. J Occup Environ Med. 2009;51(12):1422–1436. | |
Shankar A, Teppala S. Urinary bisphenol A and hypertension in a multiethnic sample of US adults. J Environ Public Health. 2012; 2012:481641. | |
Siddiqui MK, Nigam U, Srivastava S, Tejeshwar DS, Chandrawati. Association of maternal blood pressure and hemoglobin level with organochlorines in human milk. Hum Exp Toxicol. 2002;21(1):1–6. | |
C8 Science Panel. Probable link evaluation of pregnancy induced hypertension and preeclampsia. Available from: http://www.c8sciencepanelorg/pdfs/Probable_Link_C8_pregnancy-induced%20hypertension_5Dec2011%20pdf. Accessed February 1, 2012. | |
Frisbee SJ, Shankar A, Knox SS, et al. Perfluorooctanoic acid, perfluorooctanesulfonate, and serum lipids in children and adolescents: results from the C8 Health Project. Arch Pediatr Adolesc Med. 2010;164(9):860–869. | |
Shankar A, Xiao J, Ducatman A. Perfluoroalkyl chemicals and elevated serum uric acid in US adults. Clin Epidemiol. 2011;3:251–258. | |
Steenland K, Tinker S, Shankar A, Ducatman A. Association of perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS) with uric acid among adults with elevated community exposure to PFOA. Environ Health Perspect. 2010;118(2):229–233. | |
Lin CY, Chen PC, Lin YC, Lin LY. Association among serum perfluoroalkyl chemicals, glucose homeostasis, and metabolic syndrome in adolescents and adults. Diabetes Care. 2009;32(4):702–707. | |
Sakr CJ, Leonard RC, Kreckmann KH, Slade MD, Cullen MR. Longitudinal study of serum lipids and liver enzymes in workers with occupational exposure to ammonium perfluorooctanoate. J Occup Environ Med. 2007;49(8):872–879. | |
Sakr CJ, Kreckmann KH, Green JW, Gillies PJ, Reynolds JL, Leonard RC. Cross-sectional study of lipids and liver enzymes related to a serum biomarker of exposure (ammonium perfluorooctanoate or APFO) as part of a general health survey in a cohort of occupationally exposed workers. J Occup Environ Med. 2007;49(10):1086–1096. | |
Olsen GW, Zobel LR. Assessment of lipid, hepatic, and thyroid parameters with serum perfluorooctanoate (PFOA) concentrations in fluorochemical production workers. Int Arch Occup Environ Health. 2007;81(2):231–246. | |
Nelson JW, Hatch EE, Webster TF. Exposure to polyfluoroalkyl chemicals and cholesterol, body weight, and insulin resistance in the general US population. Environ Health Perspect. 2010;118(2):197–202. | |
Shankar A, Li J. Association between serum gamma-glutamyltransferase level and prehypertension among US adults. Circ J. 2007;71(10):1567–1572. | |
Mazzali M, Hughes J, Kim YG, et al. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension. 2001;38(5):1101–1106. | |
Grundy SM, Brewer HB Jr, Cleeman JI, Smith SC Jr, Lenfant C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004;109(3):433–438. | |
Sesso HD, Buring JE, Chown MJ, Ridker PM, Gaziano JM. A prospective study of plasma lipid levels and hypertension in women. Arch Intern Med. 2005;165(20):2420–2427. | |
Liu C, Yu K, Shi X, et al. Induction of oxidative stress and apoptosis by PFOS and PFOA in primary cultured hepatocytes of freshwater tilapia (Oreochromis niloticus). Aquat Toxicol. 2007;82(2):135–143. | |
Yao X, Zhong L. Genotoxic risk and oxidative DNA damage in HepG2 cells exposed to perfluorooctanoic acid. Mutat Res. 2005;587(1–2):38–44. | |
Qian Y, Ducatman A, Ward R, et al. Perfluorooctane sulfonate (PFOS) induces reactive oxygen species (ROS) production in human microvascular endothelial cells: role in endothelial permeability. J Toxicol Environ Health A. 2010;73(12):819–836. | |
Hu W, Jones PD, DeCoen W, et al. Alterations in cell membrane properties caused by perfluorinated compounds. Comp Biochem Physiol C Toxicol Pharmacol. 2003;135(1):77–88. | |
National Center for Health Statistics-CDC. National Health and Nutrition Examination Survey 2003–2004: reference manuals and reports. Available from: http://www.cdcgov/nchs/nhanes/nhanes2003-2004/nhanes03_04.htm. Accessed October 22, 2010. | |
Perloff D, Grim C, Flack J, et al. Human blood pressure determination by sphygmomanometry. Circulation. 1993;88(5 Pt 1):2460–2470. | |
Chobanian AV, Bakris GL, Black HR, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42(6):1206–1252. | |
National Center for Health Statistics-CDC. Plan and Operation of the Third National Health and Nutrition Examination Survey, 1988–1994. Rockville, MD: US Department of Health and Human Services (Publication 94-1308); 1994. Available from: Plan and Operation of the Third National Health and Nutrition Examination Survey, 1988–1994. Rockville, MD: US Department of Health and Human Services (Publication 94-1308); 1994. Accessed September 26, 2013. | |
Update on the 1987 Task Force Report on High Blood Pressure in Children and Adolescents: a working group report from the National High Blood Pressure Education Program. National High Blood Pressure Education Program Working Group on Hypertension Control in Children and Adolescents. Pediatrics. 1996;98(4 Pt 1):649–658. | |
Sorof JM, Lai D, Turner J, Poffenbarger T, Portman RJ. Overweight, ethnicity, and the prevalence of hypertension in school-aged children. Pediatrics. 2004;113(3 Pt 1):475–482. | |
National Center for Health Statistics-CDC. Procedures for laboratory components of NHANES. Available from: http://www.cdcgov/nchs/data/nhanes/nhanes_03_04/blood03_04pdf. Accessed October 22, 2010. | |
Hung H-M. Nonlinear regression analysis for complex surveys. Commun Stat Theory Methods. 1990;19(9):3447–3470. | |
Erdman D, Little M. Nonlinear regression analysis and nonlinear simulation models. Cary, NC: SAS Institute Inc. Available from: http://support.sas.com/rnd/app/ets/papers/nonlinearmodels.pdf. Accessed September 25, 2013. | |
National Center for Health Statistics-CDC. Analytical and reporting guidelines for NHANES. Available from: http://www.cdcgov/nchs/data/nhanes/nhanes_03_04/nhanes_analytic_guidelines_dec_2005%20pdf. Accessed October 22, 2010. | |
Oparil S, Zaman MA, Calhoun DA. Pathogenesis of hypertension. Ann Intern Med. 2003;139(9):761–776. | |
Carretero OA, Oparil S. Essential hypertension. Part I: definition and etiology. Circulation. 2000;101(3):329–335. | |
Wang W, Lee ET, Fabsitz RR, et al. A longitudinal study of hypertension risk factors and their relation to cardiovascular disease: the Strong Heart Study. Hypertension. 2006;47(3):403–409. | |
Geiger S, Xiao J, Shankar A. Positive association between perfluoroalkyl chemicals and hyperuricemia in children. Am J Epidemiol. 2013; 177(11):1255–1262. | |
Melzer D, Rice N, Depledge MH, et al. Association between serum perfluorooctanoic acid (PFOA) and thyroid disease in the US National Health and Nutrition Examination Survey. Environ Health Perspect. 2010;118(5):686–692. | |
Knox SS, Jackson T, Javins B, et al. Implications of early menopause in women exposed to perfluorocarbons. J Clin Endocrinol Metab. 2011;96(6):1747–1753. | |
Innes KE, Ducatman AM, Luster MI, et al. Association of osteoarthritis with serum levels of the environmental contaminants perfluorooctanoate and perfluorooctane sulfonate in a large Appalachian population. Am J Epidemiol. 2011;174(4):440–450. | |
Seals R, Bartell SM, Steenland K. Accumulation and clearance of perfluorooctanoic acid (PFOA) in current and former residents of an exposed community. Environ Health Perspect. 2010;119(1):119–124. | |
Lee MS, Wahlqvist ML, Yu HL, Pan WH. Hyperuricemia and metabolic syndrome in Taiwanese children. Asia Pac J Clin Nutr. 2007; 16 Suppl 2:594–600. | |
Robinson R. The fetal origins of adult disease. BMJ. 2001;322(7283):375–376. | |
Solomons NW. Programme and policy issues related to promoting positive early nutritional influences to prevent obesity, diabetes and cardiovascular disease in later life: a developing countries view. Matern Child Nutr. 2005;1(3):204–215. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.