")
Back to Journals » Patient Preference and Adherence » Volume 8
Motivations toward smoking cessation, reasons for relapse, and modes of quitting: results from a qualitative study among former and current smokers
Authors Buczkowski K , Marcinowicz L , Czachowski S, Piszczek E
Received 14 May 2014
Accepted for publication 17 July 2014
Published 1 October 2014 Volume 2014:8 Pages 1353—1363
DOI https://doi.org/10.2147/PPA.S67767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Krzysztof Buczkowski,1 Ludmila Marcinowicz,2 Slawomir Czachowski,1 Elwira Piszczek3
1Department of Family Medicine, Collegium Medicum, Nicolaus Copernicus University, Torun, 2Department of Family Medicine and Community Nursing, Medical University of Bialystok, Bialystok, 3Sociology Institute, Nicolaus Copernicus University, Torun, Poland
Background: Smoking cessation plays a crucial role in reducing preventable morbidity and mortality and is a recognized public-health-policy issue in many countries. Two of the most important factors that affect the efficacy of quitting smoking are motivation and the ability to cope with situations causing relapse.
Aim: The objective of the study reported here was to investigate former and current smokers’ motivations for smoking cessation, reasons for relapse, and modes of quitting.
Methods: We arranged four focus groups with 24 participants (twelve current and twelve former smokers) and eleven semi-structured interviews (five current and six former smokers) with a view to understanding and categorizing their opinions on motivations and the course and process of smoking cessation. The data were next analyzed using descriptive qualitative methods.
Results: Three main themes were identified: (1) motivations to quit smoking, (2) reasons why smokers sometimes relapse, and (3) modes of quitting smoking. Within the first theme, the following six subthemes surfaced: (1) a smoking ban at home and at work due to other people’s wishes and rules, (2) the high cost of cigarettes, (3) the unpleasant smell, (4) health concern, (5) pregnancy and breastfeeding, and (6) a variety of other factors. The second theme encompassed the following subthemes: (1) stress and the need to lessen it by smoking a cigarette, (2) the need to experience the pleasure connected with smoking, and (3) the smoking environment both at home and at work. Participants presented different smoking-cessation modes, but mainly they were unplanned attempts.
Conclusion: Two very important motivations for smoking cessation were a smoking ban at home and at work due to other people’s wishes and rules, and the high cost of cigarettes. The most common smoking-cessation mode was a spontaneous decision to quit, caused by a particular trigger factor. Relapse causes encompassed, most notably: stress, lack of the pleasure previously obtained from smoking, and the smoking environment.
Keywords: motivation, smoking cessation, primary care, qualitative research
Background
It is widely known that cigarette smoking is a large contributor to preventable morbidity and mortality in developed countries.1,2 According to the World Health Organization (WHO), over 1 billion people are addicted to tobacco smoking, and it is estimated that the number of tobacco-related deaths will rise from approximately 6 million deaths per year now to around 10 million per year by 2030.3,4 In the 1970s and 1980s, Poland had one of the highest tobacco consumptions among countries, with the percentage of smokers reaching 70% among working men. Over the last few years, the percentage of smokers has decreased, but it still remains 29% in the adult population.5,6
Although smoking is associated with many diseases and has negative consequences, stopping smoking still allows for smoking-related diseases and deaths to be avoided. In order to improve public-health goals, it is essential to reduce the prevalence of smoking through smoking prevention as well as by increasing successful smoking-cessation attempts.7–9 In short, it is worth emphasizing that benefits resulting from smoking cessation affect all age groups, and the sooner smokers quit, the greater the benefits will be.10
In recent decades, significant reductions in tobacco smoking have been achieved in many countries owing to public-health campaigns, tobacco-control programs, and tobacco-control policies.5,11–13 To this end, the Polish parliament has implemented regulations protecting the public from the consequences of tobacco consumption. These include: a smoking ban in public places, a ban on tobacco advertisements, and the requirement for health-warning labels to be placed on tobacco products. The price of cigarettes has been considerably raised, and many nationwide and local campaigns have been organized to increase awareness about smoking-related health hazards and to reduce the number of smokers.14–16 The public reception of these regulations seems to be positive, because over the last 6 years, the percentage of people in favor of a smoking ban in public places has risen from 79% to 84%.17 All these actions have contributed to a significant increase in people quitting smoking, who, for the most part, have done this without resorting to any drugs or professional help.16 The access to psychological help is limited, as there is no special stop-smoking service. For this reason, it is general practitioners (GPs) and nurses who are the main helpers in smoking cessation. On the other hand, smokers are offered full access to pharmacotherapy. Varenicline and bupropion require a prescription, whereas a nicotine replacement therapy and citisine are available without one.
Smoking is a disease resulting from addiction to nicotine, which activates nicotinic receptors in the brain, especially in the reward system.18,19 Nicotine addiction is the main cause of smoking continuation, and successful abstinence depends a lot on the dependence level.18 Both the dependence level and the duration of addiction have an impact on the occurrence of abstinence symptoms and relapse after an attempt to quit smoking. In order to fully understand the smoking continuation and smoking-cessation process, apart from knowledge about addiction, it is necessary to understand human motivation for behavior change, because motivation triggers cessation attempts. There are several theories describing behavior change.
The “transtheoretical model” assumes that a smoker goes through a series of stages of behavior before quitting successfully.20 These are: precontemplation, contemplation, preparation, action, and maintenance. In each of these stages, the level of motivation is different, and, in order to move through to the subsequent stages, a specific level of motivation must be achieved. In line with this popular model, the type of intervention should be tailored to the motivational stage, which means that patients at different stages of quitting may require different types of support.21
Another interesting theory describing smoking cessation is the “PRIME [plans, responses, impulses, motives, evaluations] Theory of Motivation”.22,23 According to this theory, smokers’ evaluative beliefs about smoking determine the decision about smoking cessation. The motivation, along with internal impulses to smoke and external triggers such as environmental cues, has an impact on subsequent behavior.22,23
On the one hand, the first (transtheoretical) model captures situations where a patient is able to stop smoking in a planned manner; on the other hand, the second (PRIME) model is better at explaining spontaneous smoking cessation.
Theories describing smoking cessation always refer to motivation, which is the basic prerequisite for undertaking a quit attempt. Therefore, it is crucial to know the former and current motivation of the smoker to stop smoking. In recent years, a number of initiatives have been undertaken in many countries to reinforce these motivations – for example, increasing cigarette prices, banning smoking in public places, and campaigns for raising awareness of smoking harm. For this reason, it seemed important to us to explore motivations for quitting in a population where a lot of people have stopped smoking over the last 25 years.
This study is part of a larger research project that aims to investigate factors that influence decisions about an antismoking intervention in primary care, including the role of the GP16 and the role of the nurse, and the patient’s experience of smoking cessation. In the face of an increasing number of smoking-cessation attempts among Polish smokers, the aim of the study reported here was to investigate former and current smokers’ motivations for smoking cessation, the reasons for relapse, and the modes of quitting.
Methods
Two complementary qualitative methods were used, as they seemed the most adequate ones to fully capture the participants’ experiences: focus groups and semi-structured interviews. Focus groups encourage interaction among participants, whereas semi-structured interviews allow for a deeper understanding of the investigated issue. The semi-structured interviews were narrative in form, and the informants could freely express their opinions.24,25
Participants, setting, and data collection
The study was conducted between December 2009 and June 2010. Purposive samples of patients for focus groups and interviews were recruited through the Institute of Sociology of the Nicolaus Copernicus University in Torun and two general practices in Bydgoszcz and Torun, Poland. The advertisements placed at the Institute of Sociology were addressed to anyone willing to participate in the study, irrespective of their age or student status. Advertisements for the research project were also disseminated in the aforementioned two practices, which together provide medical services to around 15,000 patients. Additionally, GPs or nurses informed patients about the opportunity to participate in the project.
A patient who had been smoking for at least 6 months and was a smoker at the time of the study was defined as a current smoker, in line with the WHO criteria.26 A person who had smoked for at least 6 months, and who had not smoked for at least 3 months prior to the study being conducted, was regarded as a former smoker. The smokers were 18 years old or older.
Four focus groups, drawn from a sample of 24 patients (twelve current and twelve former smokers), were arranged: two groups of current smokers and two of former smokers. In addition, eleven semi-structured interviews (five with current and six with former smokers) were conducted. A summary of the participants in the focus groups and at the interviews is presented in Table 1.
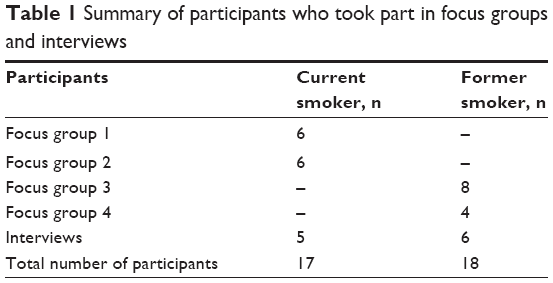 | Table 1 Summary of participants who took part in focus groups and interviews |
There were 35 participants in total, including 13 women and 22 men, with a mean age of 41 years. The average duration of smoking was about 15 years, which was slightly shorter in women (14 years) than in men (almost 17 years). The participants’ characteristics are shown in Table 2.
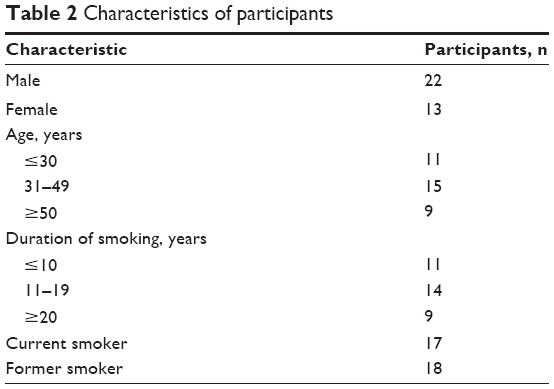 | Table 2 Characteristics of participants |
Focus-group discussions were conducted by an experienced moderator (EP) and the interviews were carried out by EP and KB in line with the topic guide derived from the literature. They began with an opening question followed by prompts, as shown in Table 3. The focus-group discussions lasted from 60 to 90 minutes, whereas the semi-structured interviews lasted from 45 to 60 minutes. They were audio recorded, transcribed verbatim, and then anonymized.
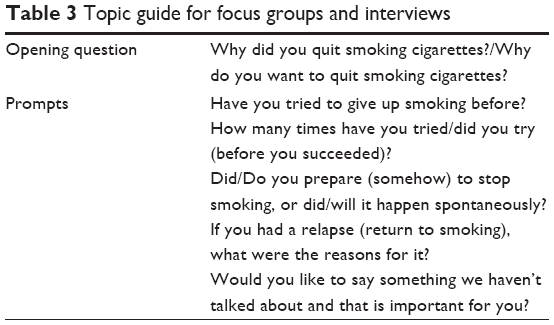 | Table 3 Topic guide for focus groups and interviews |
After the third focus group and the sixth interview, data saturation was achieved. However, because another focus group and further interviews had already been arranged, we decided to conduct them.
Data analysis
This study draws on qualitative content analysis as demonstrated by Graneheim and Lundman,27 Sandelowski,28 and Hsieh and Shannon.29 “Content analysis” is understood here as a technique for ordering and describing data. The semi-structured interview data were analyzed with a view to establishing a straightforward descriptive summary of the informational contents of the data.
The focus-group discussions and interviews were analyzed by a multidisciplinary team (researcher, physician, sociologist).
Two authors (KB, LM) analyzed the transcripts and identified meaning units that described the smokers’ motivations for smoking cessation, reasons for smoking relapse, and modes of stopping smoking. These were subsequently condensed and independently labeled with various codes to express a general understanding of them (Table 4). The codes were finally juxtaposed and formulated into subthemes and themes, after discussion with other researchers (EP, SC). The analysis revealed three major themes, which are described in the “Results” section.
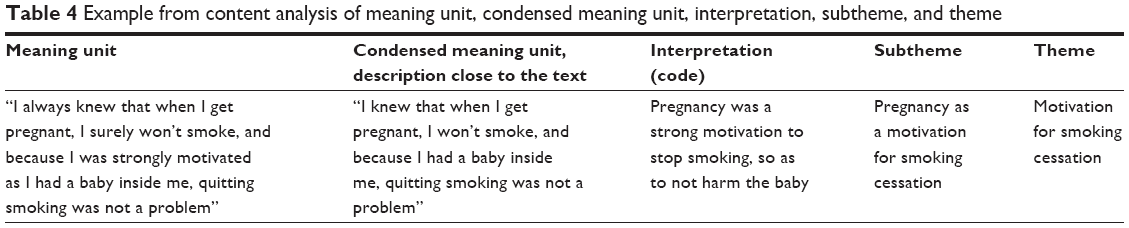 | Table 4 Example from content analysis of meaning unit, condensed meaning unit, interpretation, subtheme, and theme |
Ethical considerations
Ethical approval was granted by the Bioethical Committee of the Collegium Medicum at Nicolaus Copernicus University, Bydgoszcz, Poland. Potential participants were provided with information about the study, and those who decided to participate gave informed consent. Confidentiality was assured, and the anonymity of the participants was protected.
Results
The analysis of transcripts from the focus-group discussions and interviews revealed three themes: (1) motivations to quit smoking, (2) reasons why smokers sometimes relapse, and (3) modes of quitting smoking.
Motivations to quit smoking
The participants, both former and current smokers, unanimously admitted that the right motivation had led them to the decision to quit smoking. In other words, the right motivation played an important role in causing behavior change. The investigated smokers, however, differed in their motivations to quit, which could be classified into the following subthemes: (1) a ban on smoking at home and at work due to other people’s wishes and rules, (2) the high cost of cigarettes, (3) the unpleasant smell, (4) health concern, (5) pregnancy and breastfeeding, and (6) a variety of other factors. These are shown in the excerpts that follow.
One of the most important reasons for quitting smoking was a smoking ban, either a formal ban (for example, at work) or an informal one (for example, at home); it was indicated as a key factor in motivating stopping smoking tobacco. Having no possibility of smoking and a willingness to obey the rules were strong motivations to quit smoking altogether:
I’ve tried. At our home … we can’t smoke. We can’t because there is a child … and this is the main reason. (Current smoker, female, age 43, focus group).
I’ve tried to quit because I work in a food store and there is a ban on smoking … so I tried to quit smoking suddenly, so that I don’t feel the temptation to smoke somewhere there in nooks and crannies. (Current smoker, male, age 53, focus group).
According to the smokers, another disincentive for smoking was the high cost of cigarettes. The rising price of cigarettes means less money in smokers’ pockets each year. The awareness of this fact and the calculations of how much must be spent per month or per year were often said to have led to smoking cessation:
Cigarettes are terribly expensive. And if one thinks how much money a year is spent, it’s terrible. (Current smoker, female, age 43, focus group).
In general, the will to quit, but mainly the money. Me and my wife smoke, she still smokes, when I counted how much money we spent together on cigarettes … it was a huge amount. (Former smoker, male, age 59, focus group).
The investigated patients also pointed to the bad smell as one of the reasons to quit smoking. They were aware that cigarette smell is irritating and unpleasant, and sometimes they received such signals from their family members. The participants decided to give up smoking so as not to expose themselves or others to the tobacco smell:
Because family members urged me to stop … It doesn’t stink. The net curtains don’t stink. Everything is clean, great. (Current smoker, male, age 52, focus group).
It stinks in the car, just like on the staircase; this also annoys me very much. (Former smoker, male, age 48, focus group).
Next, health concern and the patient’s condition were a particularly strong motivation in patients with an already diagnosed disease. In such cases, they were more willing to stop smoking in order to improve their health:
It turned out that I’ve got hypertension and this made me sort the smoking problem out. (Former smoker, female, age 57, focus group).
The first attempt [to quit] was after being diagnosed with throat disease due to smoking. (Former smoker, male, age 48, focus group).
The fear of health loss in the future was also relevant to the smokers, as the majority of them were aware of the health hazards resulting from smoking:
… if I were to stop smoking … surely the health argument would be first and foremost. (Former smoker, male, age 57, focus group).
Also, those who were current smokers pointed to concern about health as the most important motivation:
The only thing that could spur me on to give up smoking is the risk of a serious disease or going down with it. (Current smoker, male, age 28, interview).
Apart from health concern, pregnancy was another important reason to stop smoking. This was reported by both former and current smokers who had not smoked when they were pregnant:
I always knew that when I got pregnant, I surely wouldn’t smoke, and because I was strongly motivated as I had a baby inside me, quitting smoking was not a problem. (Former smoker, female, age 28, focus group).
When I got pregnant, I gave up smoking straightaway. (Former smoker, female, age 30, focus group).
One of the participants strongly emphasized that she had a strong motivation to attempt to quit and maintain nonsmoking only during her pregnancies. Outside those periods, she returned to smoking:
I didn’t smoke twice in my life – when I was pregnant twice; apart from that, I never tried to stop smoking. (Current smoker, female, age 33, focus group).
Another female smoker quit only in the first two pregnancies, but in her third pregnancy she did not succeed:
I gave up smoking in my first two pregnancies, but always returned to it. I smoked even while pregnant during the third time. (Current smoker, female, age 50, interview).
Breastfeeding was also a strong motivation for nonsmoking:
… after the pregnancy, while breastfeeding, I didn’t smoke either, but later somehow. (Current smoker, female, age 29, focus group).
Sometimes the participants underlined the interplay of several factors in smoking cessation. They reported that only a variety of motivating factors coming together from several spheres of life could influence a smoker’s decision to stop smoking. This is illustrated by the following:
In some sense all the arguments start to come to the fore, little by little … because if you think about it, you will find the cost, health aspects, and family … all in one bag. (Former smoker, female, age 57, focus group).
It seems that the majority of the respondents were motivated by multiple factors; however, they usually focused on the most important motivation strictly related to their smoking cessation. This varied depending on each smoker’s personal and financial situation, health, or profession.
Relapse reasons
Another theme that emerged from the analysis of the transcripts was the reasons for relapse of the smokers who had earlier managed to quit. Relapsing is a relevant problem, because smokers make enormous efforts to stop smoking, and, subsequently, under certain conditions, they return to smoking.
These conditions were divided into the following subthemes: (1) stress and the need to lessen it by smoking a cigarette, (2) the wish to experience the pleasure connected with smoking, and (3) the smoking environment both at home and at work.
One of the most frequently reported relapse reasons was stress. In high stress situations, the participants reached for cigarettes. The need to smoke a cigarette was so strong that it caused a relapse. The level of stress that caused the relapse was usually higher than that experienced daily, which the smokers coped with without a cigarette. This is illustrated by the example of a woman who was anxious about the outcome of her child’s operation:
I went with … daughter … for an operation, … I didn’t smoke the whole time, I took her to the operating theatre. … I got so nervous that I … bought … cigarettes and smoked them in 90 minutes. (Current smoker, female, age 52, focus group).
Another smoker described the effect cigarette smoking had on him in a stressful moment and what he experienced that made him relapse:
I returned to smoking because of problems and stress. Cigarettes brought me tranquility and oblivion. They offer a way out when there’s no way out. (Former smoker, male, age 39, interview).
Another frequently reported reason for relapse was the pleasure of smoking and the lack of this in the abstinence period. The need to experience pleasure from smoking caused a relapse, particularly if there were no other restrictions:
Smoking brings pleasure. I know that quitting smoking was quite hard for me. I’m allowed to smoke at work … and it brings me pleasure, so I just smoke. (Current smoker, female, age 33, focus group).
The smoker’s environment played an important role in smoking relapse. It was important whether the people that smokers spent time with at home, work, or while out with were smokers. If the smokers were with other people who smoked, this could result in a relapse to smoking. For example, one of the participants commuted with a smoker and was forced to passively inhale tobacco smoke. This led him to relapse, even though he had managed to quit smoking.
… I started to commute with one guy who smoked constantly on the way, so when I swallowed his smoke, I had to have my own cigarette. (Current smoker, male, age 53, focus group).
Another participant returned to smoking because of his job profile. As soon as he started to work in a bar again, where he was permanently exposed to cigarette smoke, he had a relapse. Earlier, when he held a different job, he succeeded in quitting smoking:
But because I work in a bar now, and I actually began to smoke because of the bar … and I had to come back to work, so I came back to work and started to smoke again. (Current smoker, male, age 24, focus group).
Also, a family environment in which there were smokers turned out to be conducive to smoking relapse. This is illustrated by the following statements:
I returned to smoking because of the company – my sister-in-law, who smokes, talked me into it. (Current smoker, female, age 50, interview).
And it was like this: everyone at home smokes and somehow I returned to smoking. (Current smoker, female, age 29, focus group).
Modes of quitting
The investigated smokers presented different smoking-cessation modes. In the majority of cases, it was a sudden decision. Occasionally, they had mentioned considering quitting, but the moment at which they stopped smoking was accidental and resulted from a strong trigger factor. Only one smoker admitted that, in his case, giving up smoking was a premeditated choice, for which he had been preparing.
One of the smokers, who stopped smoking straight after his son’s birth, put it this way:
… After my son’s birth, my wife asked me why I smoked. … I gave up straightaway. So … it was … an impulse following my wife’s question … I started to calculate … I spend so much money, that I have a son … (Former smoker, male, age 42, focus group).
This example illustrates situations when, at a certain moment, an impulse appears, which next leads to a decision and action (that is, smoking cessation). After making the decision, the smokers looked for arguments that helped them to stick to their decision and abstain from smoking.
Another former smoker drew attention to the fact that he had considered stopping smoking, but only a particular impulse – a conducive situation – made him quit smoking. Such an impulse acts as a trigger. This is shown by the following example:
I was thinking: if only I could give up these cigarettes.
… What helped was pharyngitis, I felt pain, took antibiotics, and for a week didn’t smoke even a cigarette, so I thought maybe I would try ... and until now it works. (Former smoker, male, age 59, focus group).
In a similar way, another participant admitted that he had been considering quitting smoking, but the final decision was made spontaneously:
It was a long and systematic process of ups and downs. I read a lot about this. I didn’t take any specific medicines. I made the decision spontaneously. (Former smoker, male, age 39, interview).
Spontaneous decision making about ceasing smoking without any prior preparation took place most frequently without any other support methods, including pharmacotherapy. For example, a participant who had stopped smoking 7 years ago described how he made a spontaneous decision and did not fall back on any help:
I gave up cigarettes only once, definitively. It happened spontaneously, I didn’t prepare for this … Swapping a cigarette for a white pill? I absolutely don’t believe in the efficacy of such pills. (Former smoker, male, age 43, interview).
The only investigated smoker who managed to stop smoking in a planned way chose to gradually diminish the number of cigarettes he smoked until it resulted in complete smoking cessation:
I came to the decision little by little. The first step was that I changed a car, and decided I wouldn’t smoke in it … I gave up the four [cigarettes] in the car. I started to smoke less and gradually less and less. (Former smoker, male, age 49, focus group).
Discussion
This study presents former and current smokers’ motivations for smoking cessation, reasons for relapse, and modes of quitting. The main finding is that smoking bans at home, at work, and in public places do motivate smokers to quit smoking. Furthermore, the participants pointed out that the rising price of cigarettes had greatly influenced their decision to stop smoking. This confirms the legitimacy of policies leading to the extension of nonsmoking areas and to the increase of cigarette prices through taxation in order to reduce the number of smokers. The participants of our study pointed to the motivating influence of smoking bans on stop-smoking attempts. Owing to smoking bans in public places and workplaces, which have been gradually introduced over many years, there are fewer and fewer smoking places. Smokers reported that they find it more difficult to obey the rules when they are smokers, and, as a result, they make quit attempts.
In a similar vein, the study by Rose et al has shown that smokers with work and home bans reported more quit attempts than those without restrictions.30 Other studies also prove the effectiveness of smoking bans, which not only protect nonsmokers from the harm of secondhand smoke but are also associated with smoking reduction and cessation.31
More frequently, the reason why smokers gave up smoking tobacco was the price of cigarettes, indicating that motivation for quitting smoking grows with the increase in cigarette prices.32 Raising cigarette prices through taxation has been for many years an important policy approach to reducing smoking and motivating even heavy smokers to stop smoking.33 A similar finding was observed in our study. The investigated smokers stressed that the cost of cigarette smoking was an important motivating factor for them, and the increase in cigarette prices affected their decision to quit. Also, the study conducted by Ross et al in Eastern Europe corroborate the effectiveness of cigarette tax increases in reducing the prevalence of smoking.34
Many smokers were largely motivated by health concern. They had stopped smoking due to tobacco-related diseases or health problems. In this way, they wanted to improve their health condition and alleviate smoking-related afflictions. Besides this, what also motivated the smokers to quit was fear of a future disease, even though they did not suffer from any affliction at the time. This is congruent with the literature, which indicates that health concern is an important reason for quitting smoking.35,36 More precisely, this is supported by studies conducted among former smokers who reported that they quit to protect their health, and current smokers who pointed to health concern as a main motivation for stopping smoking.36 Moreover, concern about one’s health has been found to be the strongest motivator, regardless of age.37,38 In numerous research studies, the most common reason for smoking cessation was fear for one’s health or anxiety about its deterioration in the future.39–42 It should be acknowledged that fear for one’s health is related to smoking-cessation attempts, no matter whether they are successful.43 This can be explained by the awareness of health consequences, which lead to smoking-cessation attempts. However, sometimes this is not enough to maintain a new behavior.44
Another strong motivation for smoking cessation was pregnancy and breastfeeding. Many research studies have pointed to the fact that it is particularly during pregnancy that most women stop smoking.35,45 Once their pregnancy is confirmed, the majority of women make an attempt to quit. The main motivation is concern for the pregnancy and the proper development of the child. Nonsmoking during breastfeeding, which is related to the same concern, also prevents mothers from reaching for a cigarette. The more educated the women are, the more frequent is the decision to stop smoking in pregnancy, which is connected to the awareness of tobacco’s negative influence on pregnancy and the baby.46 Regrettably, after a successful quit attempt with a strong motivation for nonsmoking, a great many women relapse, even while still pregnant.46
While discussing the issue of the motivation to stop smoking, it is worth drawing attention to the fact that smokers are usually motivated by multiple factors; however, in the interviews, they usually focused on the most important one. In our study, only one participant indicated several factors had played a role in motivating him to quit; the others mentioned the most salient motivating factor for them.
Apart from smoking cessation, what is also relevant to reducing the number of smokers is having as few relapses as possible. Maintenance is strictly related to the patient’s satisfaction resulting from smoking cessation.44 As long as the benefits of nonsmoking prevail and the temptation to smoke is overcome, the patient will remain an ex-smoker. However, in certain situations, a complex interplay of multiple factors can affect a former smoker and result in a relapse, particularly in high-risk situations, such as stress, social pressure, or exposure to smoking-related stimuli.47 It is believed that smoking helps people to cope with stress and brings joy.48 This also resurfaced in our study: the participants pointed to stress, pleasure from smoking, and a smoking environment as the conditions that led them to relapse. For this reason, while analyzing smokers’ experiences, in order to prevent relapse, we should pay attention to how former smokers cope with stress and give them advice on how to avoid certain situations while making a quit attempt. Otherwise, these situations will make former smokers more vulnerable to smoking at certain times when circumstances appear to favor this – for example, in stress or depression.49
Besides this, smokers who want to quit should be advised to avoid a smoking environment, which is now easier at work where regulations restricting smoking have been implemented. This seems to be a much more difficult thing to accomplish at home, and, if family members smoke, a former smoker is exposed to the temptation. The environment in which there are household smoking bans is more protective of a relapse.50 This is also corroborated by studies conducted among women who stopped smoking in pregnancy and later had a relapse.51 Relapsing happens much more often when a partner is a smoker than in the cases where a partner has never smoked or is a former smoker. Nevertheless, it should be borne in mind that there is no single universal and effective strategy of relapse prevention. The conducted meta-analyses point to the efficacy of pharmacotherapy in relapse prevention; there is no substantial evidence to prove the efficacy of behavioral intervention in helping smokers who have successfully quit to avoid relapsing.52,53
When it comes to modes of quitting, the majority of smokers intent on giving up succeeded because they acted on an impulse, without prior preparation for smoking cessation. Only one participant in our study stopped smoking in a planned manner, gradually decreasing the number of smoked cigarettes. These findings are congruent with other studies, which demonstrate that most smokers decide to quit smoking without prior preparation.54–56 In a survey conducted among smokers and former smokers, West and Sohal found that almost half made a quit attempt without preplanning it.54 Most smokers at a certain stage of smoking come to the point where the arguments for quitting are stronger than those for continuing smoking.54 At a certain moment during this stage, under the influence of a trigger factor, a smoker actually stops smoking.54 Such actions are no less effective than the planned ones that we deal with occasionally.55 It is worth emphasizing the fact that, in our study, the process of smoking cessation reported by the participants was closer to that captured by the PRIME Theory,22,54 rather than to the transtheoretical model of health-behavior change.20
An important issue in analyzing the process of smoking cessation and maintenance appears to be the recognition of individual differences. Smoking-cessation interventions by health professionals should take into account the specific circumstances of the individual smoker, including their life situation and ability to cope with difficult situations.
Limitations
A possible limitation of this study is the relatively small number of interviews. Even though saturation was achieved, there may be selection biases due to the place of recruitment. More specifically, the primary-care setting could have led to selection biases in that there were more patients presenting with health problems; also, the recruitment process at the Institute of Sociology could have resulted in better-educated participants. Nevertheless, we think the data obtained in our study are sufficiently robust to describe smokers’ motivations for smoking cessation, reasons for relapse, and modes of quitting.
We consider focus-group dynamics another limitation, which may considerably affect the presentation of participants’ experiences. For example, participants may strive for conformity in a group or hide their real personal experiences in order to save face. This limitation is overcome by the semi-structured interviews, during which our participants could freely articulate their opinions, without interaction with the group.
Another limitation, which is difficult to avoid in retrospective research, is recall bias, caused by differences in the accuracy of the memories retrieved by the participants. In our opinion, smokers can accurately remember information relevant to the reason for smoking cessation or relapse; nonetheless, bias can still occur.
Implications for practice and further research
The study confirms the validity of legal actions restricting smoking cigarettes that have been taken over several years in many countries, including Poland. It appears that it is necessary to systematically extend legal restrictions on smoking, as it motivates smoking cessation. Moreover, raising cigarette prices through taxation should be continued, as it also has an impact on decisions about smoking cessation. These actions give patients a chance to make a quick profit from the money saved. Another incentive for smoking cessation may be conformity with a smoking ban at home, which contributes to the health improvement of all residents. In antismoking interventions, especially with younger smokers, it is worth relying on novel incentives, such as online interventions, which are available from different electronic devices. Further measures in this direction could have a strong motivating effect on smokers. Finally, what could further be explored is the issue of age and sex in relation to different motivations, reasons for relapse, or the stages of the cessation process.
This study adds to knowledge about highly motivating factors in stopping smoking. The concern for one’s own health, pregnancy, and breastfeeding can be used as conversation topics, as they highly motivate to quitting. It is particularly important to emphasize health hazards to patients who do not suffer from smoking-related diseases yet, as this group of patients can achieve the best results through early smoking cessation. For those who already suffer from smoking-related disease, it is worth pointing to the connection between the disease and smoking, which can strongly motivate smoking cessation.
Further research should focus on the problem of relapse, especially prevention measures that should be taken. Previous studies have demonstrated that pharmacotherapy can be successful in decreasing the relapse risk. It is worth exploring whether formal smoking restrictions (removal of temptation) can reduce the number of relapses and whether reducing stress (for example, stress-management training) can be applied to people who are intent on giving up smoking and, in the past, have already had a relapse due to stress.
Conclusion
This study reveals smokers’ motivations for smoking cessation, reasons for relapse, and modes of quitting. The study has demonstrated the validity of tobacco-control policies aimed at restricting smoking and increasing cigarette prices, which play an ever more important role in motivating smoking cessation. Moreover, our study has also corroborated that health concern is an important motivation for smoking cessation. Our results also report on smoking-cessation modes, the most common of which was a spontaneous decision, caused by a particular trigger factor. This shows that people living and working with smokers should constantly motivate them to quit, because it is not known when the right moment for smoking cessation is. Relapse causes also remain an important issue. In our study, these encompassed, most notably: stress, lack of the pleasure previously obtained from smoking, and the smoking environment. It appears that it is essential to work out measures for relapse prevention to enhance the number of successful smoking cessation attempts.
Acknowledgments
The study was financially supported by the Nicolaus Copernicus University in Torun. The authors thank all participating patients.
Disclosure
The authors declare no conflicts of interest in this work.
References
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442. | ||
Danaei G, Vander Hoorn S, Lopez AD, Murray CJ, Ezzati M; Comparative Risk Assessment collaborating group (Cancers). Causes of cancer in the world: comparative risk assessment of nine behavioural and environmental risk factors. Lancet. 2005;366(9499):1784–1793. | ||
World Health Organization (WHO). WHO Report on the Global Tobacco Epidemic, 2011: Warning about the Dangers of Tobacco. Geneva: WHO; 2011. Available from: http://whqlibdoc.who.int/publications/2011/9789240687813_eng.pdf?ua=1. Accessed August 28, 2014. | ||
2008 PHS Guideline Update Panel, Liaisons, and Staff. Treating tobacco use and dependence: 2008 update US Public Health Service Clinical Practice Guideline executive summary. Respir Care. 2008;53(9): 1217–1222. | ||
WHO Europe. The Current Status of the Tobacco Epidemic in Poland. Copenhagen: WHO; 2009. Available from: www.euro.who.int/__data/assets/pdf_file/0006/68064/E92470.pdf. Accessed August 27, 2014. | ||
Neroth P. Stubbing out Communist habits. Lancet. 2005;366(9480): 109–110. | ||
Centers for Disease Control and Prevention (CDC). State-specific prevalence of cigarette smoking and smokeless tobacco use among adults – United States, 2009. MMWR Morb Mortal Wkly Rep. 2010; 59(43):1400–1406. | ||
CDC. Smoking-attributable mortality, years of potential life lost, and productivity losses – United States, 2000–2004. MMWR Morb Mortal Wkly Rep. 2008;57(45):1226–1228. | ||
Federico B, Costa G, Ricciardi W, Kunst AE. Educational inequalities in smoking cessation trends in Italy, 1982–2002. Tob Control. 2009;18(5): 393–398. | ||
Edwards R. The problem of tobacco smoking. BMJ. 2004;328(7433): 217–219. | ||
Friend K, Levy DT. Reductions in smoking prevalence and cigarette consumption associated with mass-media campaigns. Health Educ Res. 2002;17(1):85–98. | ||
Levy DT, Chaloupka F, Gitchell J. The effects of tobacco control policies on smoking rates: a tobacco control scorecard. J Public Health Manag Pract. 2004;10(4):338–353. | ||
WHO. The World Health Report 2002: Reducing Risks, Promoting Healthy Life. Geneva: WHO; 2002. Available from: http://www.who.int/entity/whr/2002/en/whr02_en.pdf?ua=1. Accessed August 27, 2014 | ||
Act of Amendment of the Act on Protection of Health Against the Consequences of Consumption of Tobacco and Tobacco Products, April 8, 2010. Available from: http://isap.sejm.gov.pl/DetailsServlet?id=WDU20100810529. Accessed September 12, 2014. Polish. | ||
Amendment of the Act on Protection of Health Against the Consequences of Consumption of Tobacco and Tobacco Products. Poland. Adopted April 8, 2010. Available from: http://data.euro.who.int/Tobacco/Sites/Legislation.aspx?legislatureID=40. Accessed April 2, 2014. | ||
Buczkowski K, Marcinowicz L, Czachowski S, Piszczek E, Sowinska A. “What kind of general practitioner do I need for smoking cessation?” Results from qualitative study in Poland. BMC Fam Pract. 2013; 14:159. | ||
Public Opinion Research Center. Postawy Wobec Palenia Papierosów [Attitudes towards smoking cigarettes]. Warsaw: Public Opinion Research Center; 2012. Available from: http://badanie.cbos.pl/details.asp?q=a1&id=4687. Accessed August 29, 2014. Polish. | ||
Breslau N, Johnson EO, Hiripi E, Kessler R. Nicotine dependence in the United States: prevalence, trends, and smoking persistence. Arch Gen Psychiatry. 2001;58(9):810–816. | ||
Johnson EO, Chase GA, Breslau N. Persistence of cigarette smoking: familial liability and the role of nicotine dependence. Addiction. 2002;97(8):1063–1070. | ||
Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51(3):390–395. | ||
Cahill K, Lancaster T, Green N. Stage-based interventions for smoking cessation. Cochrane Database Syst Rev. 2010;(11):CD004492. | ||
West R. The multiple facets of cigarette addiction and what they mean for encouraging and helping smokers to stop. COPD. 2009;6(4): 277–283. | ||
Uppal N, Shahab L, Britton J, Ratschen E. The forgotten smoker: a qualitative study of attitudes towards smoking, quitting, and tobacco control policies among continuing smokers. BMC Public Health. 2013;13:432. | ||
Kitzinger J. Focus groups with users and providers of health care. In: Pope C, Mays N, editors. Qualitative Research in Health Care. 2nd ed. London: BMJ Books; 1999:20–29. | ||
Kvale S, Brinkmann S. InterViews: Learning the Craft of Qualitative Research Interviewing. 2nd ed Los Angeles, CA: Sage; 2009. | ||
WHO. Guidelines for Controlling and Monitoring the Tobacco Epidemic. Geneva: WHO; 1998. | ||
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. | ||
Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–340. | ||
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. | ||
Rose A, Fagan P, Lawrence D, Hart A Jr, Shavers VL, Gibson JT. The role of worksite and home smoking bans in smoking cessation among US employed adult female smokers. Am J Health Promot. 2011;26(1): 26–36. | ||
Zablocki RW, Edland SD, Myers MG, Strong DR, Hofstetter CR, Al-Delaimy WK. Smoking ban policies and their influence on smoking behaviors among current California smokers: a population-based study. Prev Med. 2014;59:73–78. | ||
Mackillop J, Amlung MT, Blackburn A, et al. Left-digit price effects on smoking cessation motivation. Tob Control. 2013. Epub 2013 July 18. | ||
Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, et al. Differential effects of cigarette price changes on adult smoking behaviours. Tob Control. 2014;23(2):113–118. | ||
Ross H, Kostova D, Stoklosa M, Leon M. The impact of cigarette excise taxes on smoking cessation rates from 1994 to 2010 in Poland, Russia, and Ukraine. Nicotine Tob Res. 2014;16(Suppl 1):S37–S43. | ||
Gallus S, Muttarak R, Franchi M, et al. Why do smokers quit? Eur J Cancer Prev. 2013;22(1):96–101. | ||
McCaul KD, Hockemeyer JR, Johnson RJ, Zetocha K, Quinlan K, Glasgow RE. Motivation to quit using cigarettes: a review. Addict Behav. 2006;31(1):42–56. | ||
Riedel BW, Robinson LA, Klesges RC, McLain-Allen B. What motivates adolescent smokers to make a quit attempt? Drug Alcohol Depend. 2002;68(2):167–174. | ||
Orleans CT, Jepson C, Resch N, Rimer BK. Quitting motives and barriers among older smokers. The 1986 Adult Use of Tobacco Survey revisited. Cancer. 1994;74(7 Suppl):2055–2061. | ||
Halpern MT, Warner KE. Motivations for smoking cessation: a comparison of successful quitters and failures. J Subst Abuse. 1993;5(3):247–256. | ||
Osler M, Prescott E. Psychosocial, behavioural, and health determinants of successful smoking cessation: a longitudinal study of Danish adults. Tob Control. 1998;7(3):262–267. | ||
Yang G, Ma J, Chen A, et al. Smoking cessation in China: findings from the 1996 national prevalence survey. Tob Control. 2001;10(2):170–174. | ||
Klemp P, Robertson MC, Stansfield S, Klemp JA, Harding E. Factors associated with smoking and the reasons for stopping in Maori and Europeans: a comparative study. N Z Med J. 1998;111(1064):148–501. | ||
Eiser JR, van der Pligt J, Raw M, Sutton SR. Trying to stop smoking: effects of perceived addiction, attributions for failure, and expectancy of success. J Behav Med. 1985;8(4):321–341. | ||
Rothman AJ. Toward a theory-based analysis of behavioral maintenance. Health Psychol. 2000;19(1 Suppl):64–69. | ||
Fingerhut LA, Kleinman JC, Kendrick JS. Smoking before, during, and after pregnancy. Am J Public Health. 1990;80(5):541–544. | ||
Kahn RS, Certain L, Whitaker RC. A reexamination of smoking before, during, and after pregnancy. Am J Public Health. 2002;92(11): 1801–1808. | ||
Hendershot CS, Witkiewitz K, George WH, Marlatt GA. Relapse prevention for addictive behaviors. Subst Abuse Treat Prev Policy. 2011;6:17. | ||
McEwen A, West R, McRobbie H. Motives for smoking and their correlates in clients attending Stop Smoking treatment services. Nicotine Tob Res. 2008;10(5):843–850. | ||
Hughes JR. Effects of abstinence from tobacco: etiology, animal models, epidemiology, and significance: a subjective review. Nicotine Tob Res. 2007;9(3):329–339. | ||
Pizacani BA, Martin DP, Stark MJ, Koepsell TD, Thompson B, Diehr P. A prospective study of household smoking bans and subsequent cessation related behaviour: the role of stage of change. Tob Control. 2004; 13(1):23–28. | ||
Prady SL, Kiernan K, Bloor K, Pickett KE. Do risk factors for post-partum smoking relapse vary according to marital status? Matern Child Health J. 2012;16(7):1364–1373. | ||
Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2012;4:CD006103. | ||
Hajek P, Stead LF, West R, Jarvis M, Hartmann-Boyce J, Lancaster T. Relapse prevention interventions for smoking cessation. Cochrane Database Syst Rev. 2013;8:CD003999. | ||
West R, Sohal T. “Catastrophic” pathways to smoking cessation: findings from national survey. BMJ. 2006;332(7539):458–460. | ||
Larabie LC. To what extent do smokers plan quit attempts? Tob Control. 2005;14(6):425–428. | ||
Ferguson SG, Shiffman S, Gitchell JG, Sembower MA, West R. Unplanned quit attempts – results from a US sample of smokers and ex-smokers. Nicotine Tob Res. 2009;11(7):827–832. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.