")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Metacognitive Reflection and Insight Therapy: A Recovery-Oriented Treatment Approach for Psychosis
Authors Lysaker PH , Gagen E , Klion R, Zalzala A, Vohs J, Faith LA, Leonhardt B, Hamm J, Hasson-Ohayon I
Received 25 November 2019
Accepted for publication 15 February 2020
Published 2 April 2020 Volume 2020:13 Pages 331—341
DOI https://doi.org/10.2147/PRBM.S198628
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Paul H Lysaker,1,2 Emily Gagen,3 Reid Klion,4 Aieyat Zalzala,5 Jenifer Vohs,2 Laura A Faith,1,6 Bethany Leonhardt,2,7 Jay Hamm,7 Ilanit Hasson-Ohayon8
1Richard L. Roudebush VA Medical Center, Indianapolis, IN, USA; 2Indiana University School of Medicine, Indianapolis, IN, USA; 3Providence VA Medical Center Department of Psychology, Providence, RI, USA; 4MERIT Institute, Boulder, CO, USA; 5Institute of Living, Hartford, CT, USA; 6University of Missouri - Kansas City, KS, USA; 7Eskenazi Health- Midtown Community Mental Health, Indianapolis, IN, USA; 8Bar Ilan University, Ramat-Gan, Israel
Correspondence: Paul H Lysaker
Richard L. Roudebush VA Medical Center, Department of Psychiatry 116A, 1481 West 10th Street, Indianapolis, IN IN 46202, USA
Email [email protected]
Abstract: Recent research has suggested that recovery from psychosis is a complex process that involves recapturing a coherent sense of self and personal agency. This poses important challenges to existing treatment models. While current evidence-based practices are designed to ameliorate symptoms and skill deficits, they are less able to address issues of subjectivity and self-experience. In this paper, we present Metacognitive Insight and Reflection Therapy (MERIT), a treatment approach that is explicitly concerned with self-experience in psychosis. This approach uses the term metacognition to describe those cognitive processes that underpin self-experience and posits that addressing metacognitive deficits will aid persons diagnosed with psychosis in making sense of the challenges they face and deciding how to effectively manage them. This review will first explore the conceptualization of psychosis as the interruption of a life and how persons experience themselves, and then discuss in more depth the construct of metacognition. We will next examine the background, practices and evidence supporting MERIT. This will be followed by a discussion of how MERIT overlaps with other emerging treatments as well as how it differs. MERIT’s capacity to engage patients who reject the idea that they have mental illness as well as cope with entrenched illness identities is highlighted. Finally, limitations and directions for future research are discussed.
Keywords: schizophrenia, psychosis, metacognition, rehabilitation, psychotherapy, recovery
Introduction
The past several decades have seen a resurgence of interest in understanding the experience and course of psychosis. This has included quantitative and qualitative studies, longitudinal and cross cultural research, work taking place in traditional academic centers as well as community-led and grass roots movements focused on first person experiences of psychosis.1–3 Taken as a whole, this work has cast considerable doubt on many long-standing assumptions. For example, the once axiomatic belief that psychosis has necessarily a progressively negative and detrimental course has been categorically rejected. In its place, assertions have arisen that recovery is an attainable outcome for many.4
Ideas about the processes that promote recovery have also evolved. The belief that recovery largely results from improvements in insight and compliance with pharmacological treatment5 has been challenged by a growing body of evidence that recovery is enabled by connections with one’s community6 and not necessarily continuous pharmacological treatment.7,8 The essence of what defines and constitutes recovery has been recognized as far more complex than the absence of disorder and disability.3 The concept of recovery has been expanded to explicitly include, for example, changes in how persons experience themselves as beings in the world. To some, recovering can mean recapturing of a sense of agency and a cohesive sense of self.2,9 Recovery can include experiences that are difficult to quantify or observe by others, because as fundamentally subjective matters they can only be known by the recovering person.10–12
This growing work on recovery has pointed to the need to revisit the purposes and mechanisms of mental health treatment. If deeply subjective change is at issue, then teaching skills and reducing symptoms may not go far enough in promoting recovery. But how could outcomes such as subjective changes in sense of agency and sense of self be addressed? Metacognitive Insight and Reflection Therapy (MERIT),13,14 an integrative form of psychotherapy, is one treatment which has sought to directly address processes which may underpin some of the more subjective aspects of recovery. MERIT focuses on metacognitive capacity, the measurable cognitive processes which enable us to understand ourselves and others in a flexible and evolving fashion and so support a sense of agency and cohesive sense of self. MERIT thus explicitly seeks to enable recovering persons to make sense of and effectively manage challenges they face by promoting metacognitive capacity.15
While previous work has described some formal aspects of MERIT,13,14 the ways in which MERIT attempts to address the issues raised above regarding recovery have not been discussed in great detail. To examine this, the current review will explore the background, practices, and supporting evidence for MERIT. To provide context, we will first offer a brief overview of the issue of subjectivity in recovery from psychosis. We will then detail how MERIT is constructed as an integrated practice and then provide a summary of research supporting its effectiveness in treating psychosis. We next discuss how it converges and diverges from other psychotherapies including emerging forms of cognitive therapy and how it uniquely handles a number of clinical challenges. Finally, we will explore key research issues facing this and other recovery-oriented treatments. We recognize international debate about the usefulness and accuracy of terms such as schizophrenia.16 As a result, we use the term psychosis to capture a broad range of forms of serious mental illness which involve significant disruptions in thought, emotion, behavior and community integration.
The Conceptualization of Psychosis as the Interruption of a Life and Persons’ Experience of Themselves
Persons diagnosed with psychosis may understand recovery in ways that are private, immediate and not directly observable by others. While the recovering person and others around them might both notice a positive change in employment or educational status, the renewal of social relationships, or the absence of inexplicable experiences (i.e., hallucinations), the recovering person alone can notice if something about how they experience themselves in the world has changed. In this way, the recovering person’s self-experience is something only available to them at the moment and not something others can unilaterally make decisions about (e.g., whether or not recovery “has happened”).
William James,17 among the first psychologists to comprehensively explore self-experience, suggested that we do not just experience the world, we experience ourselves experiencing the world. Our self-experience becomes more than just another object we can think about. When we experience ourselves experiencing the world, we also experience ourselves responding to that experience and making interpretations. Our experience of our responses and interpretations are also not negligible abstractions. They are the basis for deciding how to understand and manage what is unfolding before us.
Given this context, what is at issue in psychosis and its resolution is not just what people experience, but also how people experience themselves. Psychosis is more than just strange experiences or social challenges. As noted above, a healthy life following psychosis may not emerge even when ostensible disease markers (e.g., hallucinations) are no longer present or when the individual demonstrates satisfactory “life skills.” Since disorder and disability represent an interruption of a life and how a person experiences themselves as they live that life, recovery is better understood as a resolution of that interruption.
Metacognition, Self-Experience in Psychosis and MERIT
These conceptualizations of recovery offer a formidable set of challenges to mental health treatment and psychotherapy in particular. What do changes in how persons experience themselves represent and what supports those changes? Current evidence-based practices that seek to ameliorate symptoms and skill deficits are often privileged due to their amenability to concrete and measurable outcomes. However, they are not intended to nor do they typically address the question of subjective experience. If our concern is self-experience, what should treatment do beyond offer benevolence and not inhibiting growth?
Of note, there is a history of claims that psychotherapy can address self-experience. For example, Frankl18 proposed a form of psychotherapy that addressed self-experience by focusing on helping individuals to find meaning. While this and other similar therapies allow for considerable therapist creativity, there is concern that these types of interventions lack definition and clear guidelines for fidelity which prevent them from being formally tested.
One potential way to respond to the challenges described above is to develop ways to operationalize the processes that support self-experience; processes which may be disrupted in psychosis and subsequently targeted by treatment. In this vein, MERIT explicitly proposes that metacognitive processes may represent just such a set of quantifiable phenomena which underlie self-experience.19,20 Since its introduction as a psychological construct over 40 years ago, metacognition has been described as a set of multilevel processes involved in thinking about one’s own mental or internal experiences.21,22 MERIT relies on the integrative model of metacognition, which proposes that metacognition can be characterized as a spectrum of mental activities.14 At one end, these metacognitive activities involve noticing specific experiences in isolation, such as being aware of and reflecting upon embodied experiences including tension in one’s lower extremities, emotions such as sadness, or thoughts about discrete things. At the other end, metacognitive activities involve the synthesis of specific experiences into larger accounts or narratives. These could involve understanding why certain thoughts, feelings or embodied experiences arose in a certain moment, or even how there are certain patterns among one’s thoughts, feelings and embodied experience across a lifespan.23 The integrative model of metacognition can account for how we functionally monitor and manage specific thoughts, emotions or desires in a given moment as well as how those experiences are understood in the larger context of our lives. Therefore, it can be the basis for correcting errors, detecting larger patterns and ultimately forging an understanding of personal experience, which in turn allows for interpersonal cooperation and community membership.
This model of metacognition also includes three assumptions which are foundational for MERIT. First, metacognition as a human activity is fundamentally integrative in nature. That is, for persons to be able to form complex ideas about themselves and others, they must have the ability to perceive the constituent elements of an experience which could later be integrated. Concretely, a larger sense of oneself would seem in part contingent upon the recognition of the pieces which will be integrated to create that larger whole.
What follows from this assumption is that failures in more elemental or discrete metacognitive activities or the disruption of awareness of basic mental experiences (e.g., noticing specific cognitive operations in one’s own mind) can leave persons with less and less material to integrate, resulting in less effectively integrated and complex senses of self and others. For example, limitations in the ability to recognize and distinguish emotional states may leave persons relatively unable to form a meaningful understanding of why they tend to feel vulnerable or react strongly in some situations but not others. As such, improving one’s ability to engage in those elemental metacognitive acts may lead to the recovery of integrative metacognitive abilities and thus the availability of a more complex sense of self and others.
The second assumption of the integrative model of metacognition is that metacognition is an intersubjective human activity. The ideas persons form about themselves and others are always created with someone else in mind who might share or be influenced by those ideas.24 The genesis of meaning is always social; there are no isolated human thinkers in any original sense. Thinking always takes its leave from inherited meanings, and meaning is inherited intersubjectively. To that degree, intersubjectivity is a condition for the possibility of metacognition. Thus, the interpersonal nature of psychotherapy and the dynamic between therapist and patient may be particularly influential in addressing metacognitive difficulties.25 This assumption also leads to the possibility that the mechanism of any kind of metacognitively oriented therapy must in part rest upon joint reflection, not one person (i.e., the therapist) transmitting a particular truth or piece of information to another (i.e., the recovering person).26
The third assumption of the integrative model of metacognition is that metacognitive activities naturally vary according to upon what they are focused. Following the work of Semerari et al,27 metacognitive activities can be distinguished based on whether they are primarily concerned with the self, others, one’s community, and/or the use of that unique awareness to respond to challenges and opportunities. Considering this assumption in the context of treatment, there is thus a need to address each of these metacognitive components, and it cannot be assumed that improvement in one area will necessarily translate into improvement in the others.
Metacognitive Reflection Insight Therapy (MERIT): The Elements
An international collaboration including experts with experience in cognitive therapy, psychoanalysis, psychosocial rehabilitation and humanistic/existential therapies for adults diagnosed with psychosis13,14 sought to create a treatment approach that would address metacognitive deficits in psychosis. Their goal was not to produce another standalone treatment for a specialized problem but to create an overarching set of elements that could be utilized by therapists with different backgrounds in order to enhance metacognition. Given the importance of meaning-making in this work, its fundamental connection with metacognition,13 and its representation of a goal that transcends any one specific approach to psychotherapy,28 it was concluded that an integrative approach was critical. A singular approach by contrast was judged to be unable to meet the needs of all patients. It was also assumed that the meanings a patient might identify could never be predetermined. As such, the approach focused on larger-scale procedures and processes rather than a specific curriculum or specified activities.
Based upon the assumption that enhancing metacognitive capacity enables persons to be better able to identify a personally meaningful sense of their challenges, MERIT was purposefully intended to be recovery-oriented, in contrast to problem-focused or symptom-based approaches. The defining structure of the therapy was agreed to be composed of eight therapeutic elements and was later termed MERIT or Metacognitive Reflection Insight Therapy by Dutch colleagues29 who conducted the first clinical trial. Each element was included after it was determined it could be measured and theoretically linked to the growth of metacognitive capacity within any given session based upon the integrative model of metacognition. All elements were understood to be related and to affect one another synergistically while also being identifiable in isolation. Each was also considered sufficiently broad as to be relevant to patients with very different clinical and psychosocial presentations.
The eight elements were divided into three groups (i.e., content, process, and superordinate). The first group, labeled the content elements, is concerned with certain larger matters that the patient should be offered a chance to reflect upon if he or she did not mention them directly. The first of these, Element One, calls for attention to or attempts to elucidate the patient’s agenda. This should involve mutual reflection upon the set of potentially contradictory, complementary or unrelated wishes and needs the patient has at the moment. Element Two concerns the patient’s thoughts and emotions in response to the therapist’s sharing their thoughts about the patient in the session. Element Three focuses on the patient’s experience within narratives or sequences of events which describe the flow of their life, rather than abstractions about that experience. Element Four calls for efforts to mutually identify the set of psychological challenges facing the patient.
The second group of elements is referred to as the process elements. The first of these, Element Five, calls for opportunities to discuss the therapeutic relationship, or specifically the interpersonal environment in which joint reflection within the session is occurring. Element Six requires a discussion of the specific effects, or lack thereof, of the session upon the patient’s embodied, cognitive, or emotional experience. While the first four elements encourage reflection on one’s wishes, desires, reactions at the moment, life experiences and challenges, the second set encourages thoughts about the context in which those reflections are taking place and their impact on the patient.
The final two elements are referred to as the superordinate elements and require that therapist reflections match the patient’s current metacognitive abilities. Specifically, Element Seven requires therapists to offer interventions that stimulate patients to think about themselves or others that match and do not exceed the patients’ metacognitive capacities. Element Eight similarly calls for therapist interventions or reflections about mastery, or how a patient uses metacognitive knowledge to respond to psychosocial challenges that match and do not exceed the patients’ metacognitive capacities for mastery. By employing the eight elements, MERIT is suggested to enhance metacognitive capacity in a manner analogous to what takes place in physical therapy; that is, a reduced ability is regained by practice at increasingly demanding levels. More simply, persons think about their thinking in each session and slowly become more proficient at this. The last two elements then, following this line of thinking, ensure that patients are practicing metacognitive activities at, but not beyond, their maximal metacognitive capacity.
Taken together, these methods are not intended to create certain content or to prescribe a particular course of a session or episode of care. They are not intended to encourage, prod, or convince people to believe specific things. They are supposed to promote the processes that allow persons to form increasingly complex ideas of themselves and others and to make individualized meaning of their experiences. Thus, assessments of outcome do not assess whether a certain “thing” is believed, or a certain “skill” has been attained, but rather whether information can be integrated, allowing broader meaning to emerge within the flow of life. This approach to assessment is discussed below.
Metacognitive Reflection Insight Therapy (MERIT): Tools and Practice
In delivering MERIT, therapists impose little structure initially, asking patients where they wish “to begin” at each session. Therapists then share their thoughts about the patient’s agenda, their own thoughts, ask for narratives, and think with patients about the problems they confront. This occurs fluidly as the dialogue between patient and therapist evolves within session and across sessions. Following this method, there is no need for agreement between therapist and patient or blanket affirmation, just the symbolization through language of what is happening in the mind of the patient and the therapist. Perhaps most important is that the patient can know what is in the therapist’s mind and to reflect upon the relationship.
To enact this, MERIT therapists are tasked with continually assessing a patient’s metacognitive capacity within session in order to offer the appropriate level of intervention, as dictated by Elements Seven and Eight. This is also a means by which therapists can track progress. To guide intervention and track progress, MERIT uses the Metacognition Assessment Scale-Abbreviated (MAS-A),20 a research and clinical tool found to have acceptable reliability and validity.23 The MAS-A is composed of four scales which correspond to the metacognitive domains first identified by Semerari and colleagues.27 These scales are labeled as Self-reflectivity (S), Understanding others (O), Decentration (D) or awareness of one’s place in the larger human community, and Mastery (M) or the use of metacognitive knowledge to understand the challenges one is facing and how to respond effectively. In line with the integrative model of metacognition, higher ratings on each scale reflect metacognitive acts of increasing complexity; each item requires that the participant can perform a metacognitive activity required at the level immediately below it. Therapist assessments of patients’ metacognitive capacities to think about themselves and others using the S and O scale form the basis for choosing appropriate levels of intervention as suggested by Element Seven, while the assessment of a patient’s mastery using the M scale corresponds to interventions dictated by Element Eight. To ensure treatment fidelity, the MERIT Therapist Adherence Scale was created based on operational definitions of therapist adherence for each element.13
To date, work has suggested that the successful supervision of MERIT involves several key elements. One important aspect of supervision is that it should help therapists to notice a patient’s experience of fragmentation at the moment during a session, and not automatically assume higher levels of integration based upon the use of single words or familiar phrases (e.g., the use of an emotion word may reflect a learned response rather than a reflection of a genuine recognition of an emotional state). A second aspect of MERIT supervision is that it should help therapists to join or share in the patient’s experience of fragmentation before attempting to jointly make meaning of it.30 This may call for supervisors to help therapists examine their basic experience of, automatic and visceral responses to, and fundamental beliefs about fragmentation. It has also been suggested that supervision should involve the identification and examination of counterproductive approaches that therapists may commonly take with individuals with psychosis, including declaring what is real and what is not, seeking to bestow knowledge or “facts” upon the patient, or seeking to reduce a patient’s pain, this later stance often stemming from a therapist feeling overwhelmed.31 These stances may appear benevolent, but they can interfere with the mutual understanding and joint meaning-making that is key to MERIT.
MERIT: Supporting Evidence
Research supporting MERIT comes from several sources involving investigations into the role of metacognitive impairments including psychopathology research, clinical trials, and case studies.
Metacognitive Impairment and Psychopathology
The potential importance of metacognitive deficits as a treatment target in psychosis comes from multiple sources. As summarized in recent reviews,19,20 cross cultural studies using the MAS-A have found that persons with psychosis experience deficits in metacognition relative to healthy controls32 and individuals who experience significant medical but not psychiatric adversity. Differing profiles of metacognitive function have also been observed in persons diagnosed with various conditions including schizophrenia,32,33 borderline personality disorder,34 bipolar disorder,35 depression,36 PTSD,37 and substance use disorders.38
Other work highlighting the importance of metacognitive deficits as potential treatment targets includes a meta-analysis reporting a link between metacognitive deficits and impairment in concurrent function across studies39 and a statistical method referred to as network analysis suggesting metacognition is a central node in the network of symptoms, neurocognition and social cognition.40 Deficits in metacognition have also been linked to prospective assessments of behavior including measures of work function, negative symptoms and motivation.20 More recent work has linked metacognition to self-compassion,41 self and rater assessments of social connections42,43 and the link between emotional distress and paranoia.44 Consistent with earlier clinical reports,45 more recent research has also documented how changes in metacognitive capacity are linked with changes over time in social function, neurocognition and social cognition among persons diagnosed with schizophrenia enrolled in rehabilitation.46
Clinical Trials
Initial evidence supporting the delivery of MERIT within clinical settings was found in an open trial of MERIT conducted within a 3-month time frame29 and a second open trial of a closely related treatment consistent with MERIT offered over a period of one year.47 Both found high rates of patient acceptance, no adverse effects, and significant improvements in metacognitive function. In the latter trial, treatment effects were detectable several years following the cessation of therapy.48 This is consistent with a recent analysis of ten treatment completers within a MERIT trial that found significant improvement in metacognitive capacities.49
Two randomized-controlled trials have also reported positive outcomes and good patient acceptance rates without evidence of adverse effects. In one trial, 20 participants with first episode psychosis and poor insight were randomized to receive 6 months of MERIT or treatment as usual. Eight of the 10 participants assigned to MERIT completed the treatment and significant improvements in clinical insight were found in this group compared to the treatment as usual group at the completion of the trial.50 In a second trial for a broader variety or patients diagnosed with schizophrenia, 18 of 26 participants completed an 8-month course of treatment with measurable gains detected in the metacognitive domains of self-reflectivity and mastery.51 Subsequent analysis of this study revealed that higher levels of clinical insight at baseline were associated with greater metacognitive gains.52 Additional evidence of the impact of this treatment was found in qualitative interviews of participants who received MERIT who reported that it promoted their own personal sense of recovery by helping them to think more clearly about themselves and experiences across their lives.53 These findings closely mirror an older qualitative study of patients diagnosed with psychosis enrolled in MERIT in a clinical setting.54 This study found that in contrast to patients receiving supportive services, patients receiving MERIT reported the treatment uniquely led to a greater sense of agency, a sense of temporal coherence across their lives, and a better ability to tolerate and manage emotional distress.
Case Studies
A final source of evidence for MERIT comes from published case studies.55–70 While susceptible to selection and confirmation bias, case studies present important idiographic and clinical information about unique and subjective experiences which can potentially complement other evidence and be synthesized into a larger understanding of this treatment approach. Table 1 presents 15 MERIT case studies (describing 16 individuals in total) which provide rich descriptions of patients’ problems, goals, and treatment outcomes, as well as changes in metacognition as measured by the MAS-A. Patients ranged in age from their 20s to 50s with treatment length ranging from 4 months to 14 years. (Two case studies of persons diagnosed with Borderline Personality Disorder were also included who had experienced transient psychosis and functioned at levels commonly found in persons with psychosis.) There is also an additional case study70 which reported the successful delivery of MERIT to an adult diagnosed with Schizotypal Personality Disorder, again without adverse effects and with clinically significant improvement.
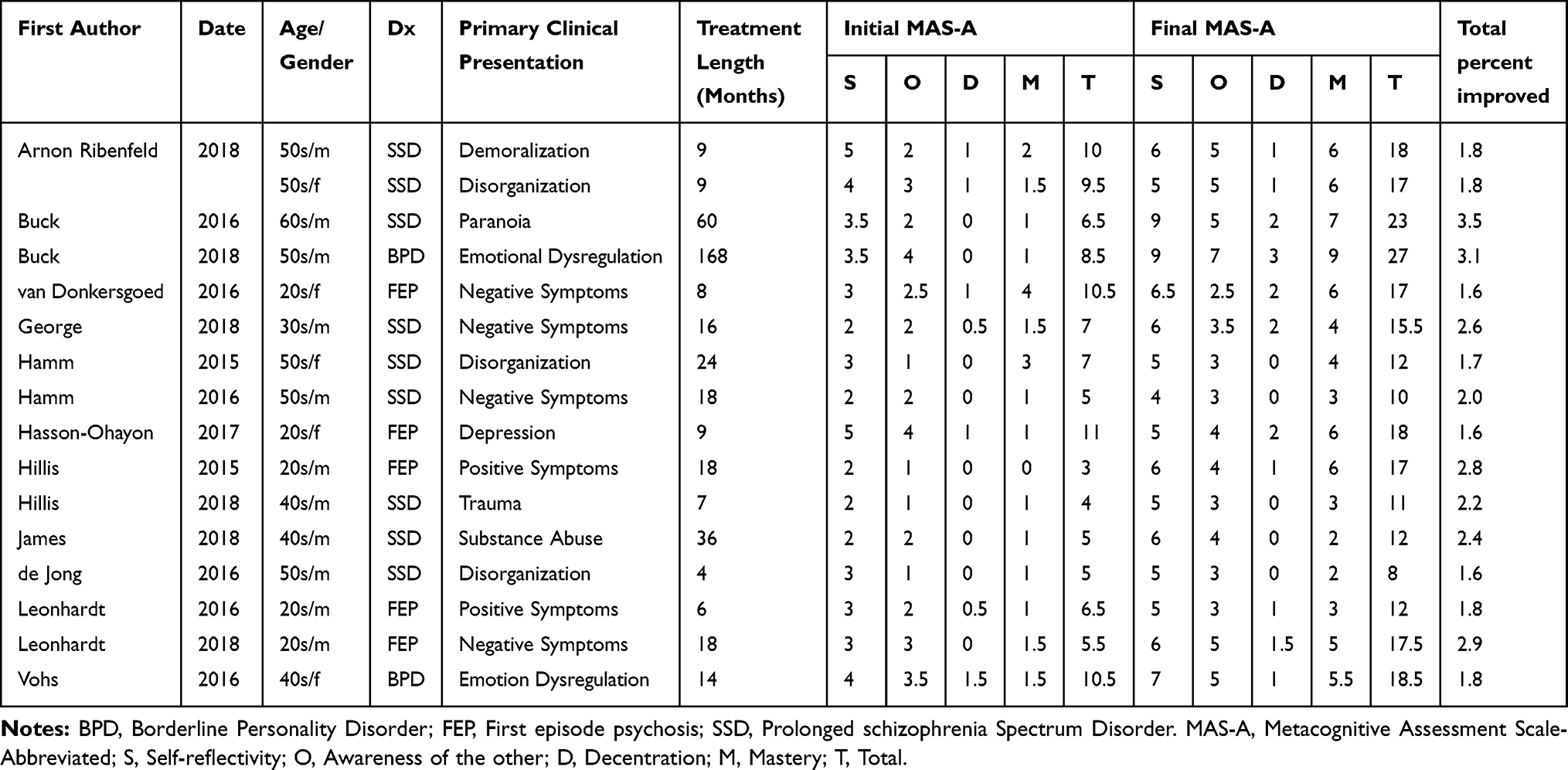 |
Table 1 Meta-Synthesis of 16 Case Reports |
Considered as a whole, the results summarized in Table 1 suggest at least two general conclusions. First, therapists from different backgrounds can successfully deliver MERIT over differing lengths of intervention in routine settings and can adapt the therapy to the unique needs of different patients. This illustrates the potential of MERIT to be flexibly adapted to meet the needs of the truly diverse group of persons who are diagnosed with psychosis. Secondly, the general levels of metacognitive change are notable. On average across the 14 studies, the final MAS-A total score was 2.5 times greater than at initiation of treatment, with the most notable changes generally occurring in self-reflectivity and mastery. While remarkable gains were noted in studies where therapy lasted for years, even if these are excluded, the other reports generally suggest a two-fold increase in metacognitive capacity.
Discussion
MERIT’s ambition is to assist persons diagnosed with psychosis to become better able to form integrated understandings of themselves and others, a capacity essential to making sense of the challenges they face and ultimately directing their own recovery. Quantitative and qualitative research as well as numerous case studies provide evidence to suggest MERIT is a treatment that is well accepted by patients without posing any risks. While considerably more study is needed, these data also provide initial evidence that engagement in MERIT is linked with significant improvements in outcomes that are meaningful to patients.
The research discussed above also suggests that MERIT possesses similarities to a number of other emerging treatments for persons with psychosis, including cognitive behavior therapy for psychosis,71 metacognitive training,72 compassion-focused therapy,73 and mindfulness.74 There appears to be a shared general interest in eliciting and understanding the details of what people think, why they have those thoughts, and their relationship to those thoughts. Indeed, a central tenet of CBT is to collaboratively identify an individual’s automatic thoughts with the goal of eventually linking them to core beliefs about oneself and others.75 As is the case with many therapies, both cognitive and otherwise, there is also an emphasis on creating a shared formulation of a person’s current psychological problems as well as identifying goals for ameliorating these problems. As Moritz et al76 recently noted, it is important not to overestimate the degree of difference between treatments that are all concerned with how human beings with psychosis make sense of their experience.
Nevertheless, at a more nuanced level, at least four features of MERIT standout as potentially unique and worthy of deeper consideration. First, MERIT does not stop when a belief has been identified, but instead requires additional focus on and exploration of context of that belief in order to grasp the larger meaning. Identical beliefs held by two patients may have profoundly different meanings given those patients’ histories, cultural background, personalities, social relationships, etc. Second, MERIT requires that sessions be primarily patient-directed, rather than therapist-directed. The patient’s agenda is primary, even though it may be shifting and opaque. Therapists must insert their own thoughts and reflections and may not support a patient’s given agenda, such as when it has an antisocial quality, but the primary concern is recognizing and jointly reflecting upon that agenda. A third novel feature is that while a MERIT session may appear to be unstructured due to its patient-driven nature, it is significantly structured in terms of therapist activity. Therapists are tasked with implementing all the elements of MERIT and constantly assessing and readjusting interventions as necessary. Finally, the underlying goal of MERIT is to help persons to make better sense of the world and this is necessarily a collaborative, complicated, and fundamentally intersubjective process. Accordingly, making sense of the world is not something that can be taught. Recovery is a matter of self-experience, or how persons experience themselves in the world, and cannot be imparted via a didactic lesson to impart a set of skills.
These differences have important practical implications when applied to clinical work. First, there is a willingness on the part of MERIT therapists to try to engage patients who are unable to identify concrete goals or even agree that they have mental illness. In MERIT, the pursuit of self-reflection is never equated with clinical insight. Clinical insight, which refers to awareness of morbid psychological change77 is not a precondition or necessarily a predetermined outcome in MERIT. Many of the patients in the case studies noted earlier entered therapy with only an awareness of a generalized and diffuse discomfort that often had an implausible explanation. MERIT simply views this as a reflection of a relatively low capacity for Mastery and thus seeks to stimulate its growth, which would allow for both for greater awareness of one’s challenges and an ability to form a working sense of how to manage them. This highlights the importance of jointly considering and defining the problems the patient faces; the issues at hand are not supplied by the therapist, another clinician, or a treatment manual. As noted elsewhere, treatment does not begin with agreement but rather with reflection of how two different people see different things when the patient’s life is the focus.25
Just as insight is not a precondition for engagement, MERIT also treats psychosis as a highly complex phenomenon that is inextricably related to self-experience and not reducible to discrete symptoms. For example, it is not uncommon for persons with psychosis to have embraced the patient role, and have come to experience being “mentally ill” as their occupation. Leaving this role behind as persons move toward recovery can feel like dangerous and like a risk, a topic that is revisited frequently in many of the case studies. While there is no space for a full discussion of this here, we suggest that the case work concretely points to a process that is similar to shared decision-making,78 but that is ultimately more about the risks that lend dignity to life and might be called in MERIT, shared risk taking.
There are important limitations. Additional randomized clinical trials are needed with more diverse patient samples. As is true for many treatment approaches, we lack the long-term follow-up assessments truly needed to document the recovery process. This lack of long-term assessment of the achievement of wellness may also reflect a need to still develop a more nuanced model of how psychosis interrupts a life and identify the key characteristics that define a life as people age.
Mixed methods approaches are also needed to better triangulate the interaction between subjective and objective outcomes. While MERIT is defined by eight elements, research is needed to determine whether all or some of these are related to observable outcomes. Interestingly, one recent study showed that two specific elements, insertion of the therapist’s mind (Element Two) and discussion of the therapeutic relationship (Element Five) were related to better outcome.49
To date, MERIT research has focused exclusively on individual interventions in outpatient settings. Work is needed to explore whether and how these procedures might be expanded to group, family and inpatient settings as well as persons with other conditions including those identified as clinical high-risk as well as other non-psychotic disorders. Another important future direction includes the continued focus on the integrative nature of this treatment and the corresponding need to understand the perspectives of therapists who were previously trained in other orientations. For instance, therapists trained in structured, manualized treatments sometimes report feeling as if they are “breaking the rules”30 by deviating from their earlier training. A broad history also exists of older theories of the phenomenology of fragmentation in psychosis, including, for example, several from different psychoanalytic traditions. As already begun elsewhere, work is needed to systematically consider how those theories may illuminate some of the core processes observed in MERIT.79 Finally, there is a need to broaden and enrich methods for assessment and conceptualization of therapeutic processes. For example, assessing session-by-session changes in addition to pre-post changes will provide rich data on trajectories of improvement.
Fueled by a broader, patient-oriented definition of recovery, this is an exciting time to explore innovative treatment methods for persons with psychosis. While this work is still in an early stage, there is certainly evidence that treatments like MERIT have the potential to significantly improve the lives of persons with psychosis and are worthy of further study and attention.
Summary
People can recover from psychosis. That recovery often requires that they form their own coherent idea of the challenges they face and how they want to manage them. This review presents Metacognitive Insight and Reflection Therapy (MERIT), a form of psychotherapy designed to help persons diagnosed with psychosis make sense of their experiences and then take charge of their own recovery. Preliminary evidence to date suggests it is feasible, acceptable and leads to clinically meaningful change. More research on this method is warranted.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Davidson L, Roe D. Recovery from versus recovery in serious mental illness: one strategy for lessening confusion plaguing recovery. J Ment Health. 2007;16(4):459–470. doi:10.1080/09638230701482394
2. Leonhardt BL, Huling K, Hamm JA, et al. Recovery and serious mental illness: a review of current clinical and research paradigms and future directions. Expert Rev Neurother. 2017;17(11):1117–1130. doi:10.1080/14737175.2017.1378099
3. van Weeghel J, van Zelst C, Boertien D, Hasson-Ohayon I. Conceptualizations, assessments, and implications of personal recovery in mental illness: a scoping review of systematic reviews and meta-analyses. Psychiatr Rehabil J. 2019;42(2):169. doi:10.1037/prj0000356
4. Andresen R, Oades L, Caputi P. The experience of recovery from schizophrenia: towards an empirically validated state model. Aust N Z Psychiatry. 2003;37:586–594. doi:10.1046/j.1440-1614.2003.01234.x
5. Kane JM. Improving patient outcomes in schizophrenia: achieving remission, preventing relapse, and measuring success. J Clin Psychiatry. 2013;74(9):e18–e18. doi:10.4088/JCP.12117tx1c
6. Korsbek L. Illness insight and recovery: how important is illness insight in peoples’ recovery process? Psychiatr Rehabil J. 2013;36(3):222–225. doi:10.1037/prj0000018
7. Moncrieff J. Antipsychotic maintenance treatment: time to rethink? PLoS Med. 2015;12(8):e1001861. doi:10.1371/journal.pmed.1001861
8. Lysaker PH, Hamm J, Hasson-Ohayon I, Pattison ML, Leonhardt BL. Promoting recovery from severe mental illness: implications from research on metacognition and metacognitive reflection insight therapy. World J Psychiatry. 2018;8(1):1–11. doi:10.5498/wjp.v8.i1.1
9. Hamm JA, Leonhardt BL, Ridenour J, Lysaker JT, Lysaker PH. Phenomenological and recovery models of the subjective experience of persons diagnosed with schizophrenia: discrepancies and implications for treatment. Psychosis. 2018;10(4):340–350. doi:10.1080/17522439.2018.1522540
10. Lysaker PH, Zalzala AB, Ladegaard N, Buck B, Leonhardt BL, Hamm JA. A disorder by any other name: metacognition, schizophrenia, and diagnostic practice. J Humanist Psychol. 2019;59(1):26–47. doi:10.1177/0022167818787881
11. Mathur S, Bhola P, Khanam F, Thirthalli J. Restoring the sense of self in the process of recovery in schizophrenia. J Psychosoc Rehabil Ment Health. 2014;1(1):31–35. doi:10.1007/s40737-014-0002-5
12. McCarthy-Jones S, Marriott M, Knowles R, Rowse G, Thompson AR. What is psychosis? A meta-synthesis of inductive qualitative studies exploring the experience of psychosis. Psychosis. 2013;5(1):1–16. doi:10.1080/17522439.2011.647051
13. Lysaker PH, Klion RE. Recovery, Meaning-Making, and Severe Mental Illness: A Comprehensive Guide to Metacognitive Reflection and Insight Therapy. New York, NY: Routledge; 2017.
14. Lysaker PH, Gagen EC, Moritz S, Schweitzer RD. Metacognitive approaches to the treatment of psychosis: a comparison of four approaches. Psychol Res Behav Manag. 2018;11:341–351. doi:10.2147/PRBM.S146446
15. Lysaker PH, Lysaker JT. Metacognition, self-experience and the prospect of enhancing self-management in schizophrenia spectrum disorders. Philos Psychiatr Psychol. 2017;24(2):69–178. doi:10.1353/ppp.2017.0021
16. Guloksuz S, van Os J. The slow death of the concept of schizophrenia and the painful birth of the psychosis spectrum. Psychol Med. 2018;48(2):229–244. doi:10.1017/S0033291717001775
17. James W. The Principles of Psychology. New York, NY: Henry Holt and Company; 1890.
18. Frankl VE. Man’s Search for Meaning: An Introduction to Logotherapy. Boston: Beacon Press; 1992.
19. Lysaker PH, Kukla M, Vohs JL, Schnakenberg Martin AM, Buck KD, Hasson Ohayon I. Metacognition and recovery in schizophrenia: from research to the development of metacognitive reflection and insight therapy. J Exp Psychopathol. 2019;10(1):2043808718814992. doi:10.1177/2043808718814992
20. Lysaker PH, Minor KS, Lysaker JT, et al. Metacognitive function and fragmentation in schizophrenia: relationship to cognition, self-experience and developing treatments. Schizophr Res Cogn. 2019;100142.
21. Flavell JH. Metacognition and cognitive monitoring: a new area of cognitive-developmental inquiry. Amer Psychol. 1979;34(10):906–911. doi:10.1037/0003-066X.34.10.906
22. Moritz S, Lysaker PH. Metacognition – what did James H. Flavell really say and the implications for the conceptualization and design of metacognitive interventions in schizophrenia. Schizophr Res. 2018;201:20–26. doi:10.1016/j.schres.2018.06.001
23. Lysaker PH, Dimaggio G. Metacognitive capacities for reflection in schizophrenia: implications for developing treatments. Schizophr Bull. 2014;40(3):487–491. doi:10.1093/schbul/sbu038
24. Stern DN. The Interpersonal World of the Infant: A View from Psychoanalysis and Developmental Psychology. New York: Basic Books; 2000.
25. Hasson‐Ohayon I, Kravetz S, Lysaker PH. The special challenges of psychotherapy with persons with psychosis: intersubjective metacognitive model of agreement and shared meaning. Clin Psychol Psychother. 2017;24(2):428–440. doi:10.1002/cpp.2012
26. Buck KD, Buck BE, Hamm JA, Lysaker PH. Martin Buber and evidence based practice: can the lion really lie down with the lamb. Psychosis. 2015;8(2):156–165. doi:10.1080/17522439.2015.1055783
27. Semerari A, Carcione A, Dimaggio G, et al. How to evaluate metacognitive functioning in psychotherapy? The metacognition assessment scale and its applications. Clin Psychol Psychother. 2003;10(4):238–261. doi:10.1002/cpp.362
28. Hasson-Ohayon I. Exploring the meaning of visual and auditory hallucinations: a commentary on Pixley’s discussion of the difficulties in addressing hallucinations during psychodynamic therapy. J Psychother Integr. 2012;22:393–396. doi:10.1037/a0030065
29. de Jong S, Donkersgoed RJM, Aleman A, et al. The practical implications of metacognitive psychotherapy in psychosis: findings from a pilot study. J Nerv Ment Dis. 2016;204(9):713–716. doi:10.1097/NMD.0000000000000564
30. Lysaker PH, Buck KD, Pattison ML, Beasley RE, Hillis JD, Hamm JA. Supervision in the psychotherapy of schizophrenia: awareness of and mutual reflection upon fragmentation. Am J Psychoanal. 2019;79(3):284–303. doi:10.1057/s11231-019-09198-y
31. Hamm JA, Buck KD, Vohs J, Westerlund RJ, Lysaker PH. Interpersonal stance and dialogue in psychotherapy for schizophrenia: a supervisory approach. Clin Superv. 2016;35(1):42–62. doi:10.1080/07325223.2016.1140102
32. Hasson-Ohayon I, Avidan-Msika M, Mashiach-Eizenberg M, et al. Metacognitive and social cognition approaches to understanding the impact of schizophrenia on social quality of life. Schizophr Res. 2015;161(2–3):386–391. doi:10.1016/j.schres.2014.11.008
33. Lysaker PH, Vohs J, Hamm JA, et al. Deficits in metacognitive capacity distinguish patients with schizophrenia from those with prolonged medical adversity. J Psychiatr Res. 2014;55:126–132. doi:10.1016/j.jpsychires.2014.04.011
34. Lysaker PH, George S, Chaudoin–Patzoldt KA, et al. Contrasting metacognitive, social cognitive and alexithymia profiles in adults with borderline personality disorder, schizophrenia and substance use disorder. Psychiatr Res. 2017;257:393–399. doi:10.1016/j.psychres.2017.08.001
35. Popolo R, Smith E, Lysaker PH, et al. Metacognitive profiles in schizophrenia and bipolar disorder: comparisons with healthy controls and correlations with negative symptoms. Psychiatr Res. 2017;257:45–50. doi:10.1016/j.psychres.2017.07.022
36. Ladegaard N, Lysaker PH, Larsen ER, Videbech P. A comparison of capacities for social cognition and metacognition in first episode and prolonged depression. Psychiatr Res. 2014;220(3):883–889. doi:10.1016/j.psychres.2014.10.005
37. Lysaker PH, Dimaggio G, Wickett-Curtis A, et al. Deficits in metacognitive capacity are related to subjective distress and heightened levels of hyperarousal symptoms in adults with posttraumatic stress disorder. J Trauma Dissociation. 2015;16(4):384–398. doi:10.1080/15299732.2015.1005331
38. Inchausti F, Ortuño-Sierra J, García-Poveda NV, Ballesteros-Prados A. Metacognitive abilities in adults with substance abuse treated in therapeutic community. Adicciones. 2017;29(2):74–82. doi:10.20882/adicciones.719
39. Arnon-Ribenfeld N, Hasson-Ohayon I, Lavidor M, Atzil-Slonim D, Lysaker PH. A meta-analysis and systematic review of the association between metacognitive abilities, symptoms and functioning among people with schizophrenia. Eur Psychiatry. 2017;46:33–41. doi:10.1016/j.eurpsy.2017.08.002
40. Hasson-Ohayon I, Goldzweig G, Lavie A, Luther L, Lysaker PH. The centrality of cognitive symptoms and metacognition within the network of symptoms, neurocognition, social cognition, and metacognition in schizophrenia. Schizophr Res. 2018;202:260–266. doi:10.1016/j.schres.2018.07.007
41. Hochheiser J, Lundin N, Lysaker PH. The independent relationships of metacognition, mindfulness, and cognitive insight to self-compassion in schizophrenia. J Ner Ment Dis. 2019;208(1):1–6.
42. Bonfils KA, Haas GL, Salyers MP. Emotion-specific performance across empathy tasks in schizophrenia: influence of metacognitive capacity. Schizophr Res Cogn. 2019;19:100139.
43. Fisher MW, Dimaggio G, Hochheiser J, Vohs J, Phalen P, Lysaker PH. Metacognitive capacity is related to self-reported social functioning and may moderate the effects of symptoms on interpersonal behavior. J Ner Ment Dis. 2019. doi:10.1097/NMD.0000000000001117
44. Buck BE, Gagen EC, Luther L, Kukla ME, Lysaker PH. Dynamic relationships between emotional distress, persecutory ideation, and metacognition in schizophrenia. Br J Clin Psychol. 2019. doi:10.1002/jclp.22904
45. Lysaker PH, Buck KD, Ringer J. The recovery of metacognitive capacity in schizophrenia across 32 months of individual psychotherapy: a case study. Psychother Res. 2007;17(6):713–720. doi:10.1080/10503300701255932
46. Kukla M, Lysaker PH. Metacognition over time related to neurocognition, social cognition, and intrapsychic foundations in psychosis. Schizophr Res Cogn. 2019;100149.
47. Bargenquast R, Schweitzer RD. Enhancing sense of recovery and self‐reflectivity in people with schizophrenia: a pilot study of metacognitive narrative psychotherapy. Psychol Psychother. 2014;87(3):338–356. doi:10.1111/papt.12019
48. Schweitzer RD, Greben M, Barenquast R. Long-term outcomes of metacognitive narrative psychotherapy for people diagnosed with schizophrenia. Psychol Psychother. 2017;90(4):668–685. doi:10.1111/papt.12132
49. Lavi-Rotenberg A, Bar-Kalifa E, de Jong S, Ben-Dror L, Lysaker PH, Hasson-Ohayon I. Elements that enhance therapeutic alliance and short-term outcomes in metacognitive reflection and insight therapy: a session by session assessment. Psychiatr Rehabil J. 2020. In press.
50. Vohs JL, Leonhardt BL, James AV, et al. Metacognitive reflection and insight therapy for early psychosis: a preliminary study of a novel integrative psychotherapy. Schizophr Res. 2018;195:428–433. doi:10.1016/j.schres.2017.10.041
51. de Jong S, van Donkersgoed RJM, Timmerman ME, et al. Metacognitive reflection and insight therapy (MERIT) for patients with schizophrenia. Psychol Med. 2019;49(2):303–313. doi:10.1017/S0033291718000855
52. de Jong S, Hasson-Ohayon I, van Donkersgoed RJM, et al. Predicting therapy success from the outset: the moderating effect of insight into the illness on metacognitive psychotherapy outcome among persons with schizophrenia. Clin Psychol Psychother. 2019. doi:10.1002/cpp.2388
53. de Jong S, Hasson-Ohayon I, van Donkersgoed R, Aleman A, Pijnenborg GHM. A qualitative evaluation of the effects of metacognitive reflection and insight therapy: ‘living more consciously’. Psychol Psychother. 2019. doi:10.1111/papt.12212
54. Lysaker PH, Kukla M, Belanger E, et al. Individual psychotherapy and changes in self-experience in schizophrenia: a qualitative comparison of patients in metacognitively focused and supportive psychotherapy. Psychiatry. 2015;78(4):305–316. doi:10.1080/00332747.2015.1063916
55. Arnon-Ribenfeld N, Bloom R, Atzil-Sloman D, Peri T, de Jong S, Hasson-Ohayon I. Metacognitive Reflection and Insight Therapy (MERIT) among people with schizophrenia: lessons from two case studies. Am J Psychother. 2018;71(4):175–185. doi:10.1176/appi.psychotherapy.20180037
56. Buck KD, Vertinski M, Kukla M. Metacognitive reflective and insight therapy: application to a long-term therapy case of borderline personality disorder. Am J Psychother. 2018;71(4):145–154. doi:10.1176/appi.psychotherapy.20180035
57. Buck KD, George SE. Metacognitive reflective and insight therapy for a person who gained maximal levels of metacognitive capacity and was able to terminate therapy. J Contemp Psychother. 2016;46(4):187–196. doi:10.1007/s10879-016-9322-y
58. Van Donkersgoed RJ, de Jong S, Pijnenborg GHM. Metacognitive Reflection and Insight Therapy (MERIT) with a patient with persistent negative symptoms. J Contemp Psychother. 2016;46(4):245–254. doi:10.1007/s10879-016-9333-8
59. George S, Buck KD. Metacognitive reflection and insight therapy for persons with severe negative symptoms of schizophrenia. Am J Psychother. 2018;71(4):135–144. doi:10.1176/appi.psychotherapy.20180036
60. Hamm JA, Leonhardt BL. The role of interpersonal connection, personal narrative, and metacognition in integrative psychotherapy for schizophrenia: a case report. J Clin Psychol. 2016;72(2):132–141. doi:10.1002/jclp.2016.72.issue-2
61. Hamm JA, Firmin RL. Disorganization and individual psychotherapy for schizophrenia: a case report of metacognitive reflection and insight therapy. J Contemp Psychother. 2016;46(4):227–234. doi:10.1007/s10879-016-9326-7
62. Hasson-Ohayon I, Arnon-Ribenfeld N, Hamm J, Lysaker PH. Agency before action: the application of behavioral activation in psychotherapy with persons with psychosis. Psychotherapy. 2017;54(3):245–251. doi:10.1037/pst0000114
63. Hillis JD, Leonhardt BL, Vohs JL, et al. Metacognitive reflective and insight therapy for people in early phase of a schizophrenia spectrum disorder. J Clin Psychol. 2015;71(2):125–135. doi:10.1002/jclp.2015.71.issue-2
64. Hillis JD, Bidlack N, Macobin B. Metacognitive reflection and insight therapy (MERIT) for persons with a schizophrenia spectrum disorder and profound history of interpersonal trauma. Am J Psychother. 2018;71(4):186–195. doi:10.1176/appi.psychotherapy.20180031
65. James A, Leonhardt BL, Buck KD. Metacognitive reflection and insight therapy for schizophrenia: a case study of an individual with a co-occurring substance use disorder. Am J Psychother. 2018;71(4):155–163. doi:10.1176/appi.psychotherapy.20180038
66. de Jong S, van Donkersgoed R, Pijnenborg GHM, Lysaker PH. Metacognitive Reflection and Insight Therapy (MERIT) with a patient with severe symptoms of disorganization. J Clin Psychol. 2016;72(2):164–174. doi:10.1002/jclp.2016.72.issue-2
67. Leonhardt BL, Benson K, George S, Buck KD, Shaieb R, Vohs JL. Targeting insight in first episode psychosis: a case study of metacognitive reflection insight therapy (MERIT). J Contemp Psychother. 2016;46(4):207–216. doi:10.1007/s10879-016-9332-9
68. Leonhardt BL, Ratliff K, Buck KD. Recovery in first episode psychosis: a case study of metacognitive reflection and insight therapy (MERIT). Am J Psychother. 2018;71(4):128–134. doi:10.1176/appi.psychotherapy.20180032
69. Vohs JL, Leonhardt BL. Metacognitive reflection and insight therapy for borderline personality disorder: a case illustration of an individual in a long term institutional setting. J Contemp Psychother. 2016;46(4):255–264. doi:10.1007/s10879-016-9335-6
70. Cheli S, Lysaker PH, Dimaggio G. Metacognitively oriented psychotherapy for schizotypal personality disorder: two cases series. Personal Ment Health. 2019. doi:10.1002/pmh.1447
71. Fowler D, Garety P, Kuipers E. Cognitive Behaviour Therapy for Psychosis: Theory and Practice. Chichester, UK: Wiley; 1995.
72. Moritz S, Andreou C, Schneider BC, et al. Sowing the seeds of doubt: a narrative review on metacognitive training in schizophrenia. Clin Psychol Rev. 2014;34(4):358–366. doi:10.1016/j.cpr.2014.04.004
73. Waite F, Knight MTD, Lee D. Self-compassion and self-criticism in recovery in psychosis: an interpretative phenomenological analysis study. J Clin Psychol. 2015;71:1201–1217. doi:10.1002/jclp.22211
74. Tabak NT, Horan WP, Green MF. Mindfulness in schizophrenia: associations with self-reported motivation, emotion regulation, dysfunctional attitudes, and negative symptoms. Schizophr Res. 2015;168:537–542. doi:10.1016/j.schres.2015.07.030
75. Beck J. Cognitive Behavior Therapy, Second Edition: Basics and Beyond. New York: Guilford Press; 2011.
76. Moritz S, Klein JP, Lysaker PH, Mehl S. Metacognitive and cognitive-behavioral interventions for psychosis: new developments. Dialogues Clin Neurosci. 2019;21(3):309–317.
77. Lysaker PH, Pattison ML, Leonhardt BL, Phelps S, Vohs JL. Insight in schizophrenia spectrum disorders: a review of its relationship with behavior, mood and perceived quality of life, its underlying causes and emerging treatments. World Psychiatry. 2018;17(1):12–23. doi:10.1002/wps.20508
78. Stovell D, Morrison AP, Panayiotou M, Hutton P. Shared treatment decision-making and empowerment-related outcomes in psychosis: systematic review and meta-analysis. Br J Psychiatry. 2016;209(1):23–28. doi:10.1192/bjp.bp.114.158931
79. Pec O, Lysaker PH, Probstova V, Leonhardt BL, Hamm JA, Bob P. The psychotherapeutic treatment of schizophrenia: psychoanalytical explorations of the metacognitive movement. J Contemp Psychother. 2020;1–8.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.