")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 7
Magnitude of opportunistic infections and associated factors in HIV-infected adults on antiretroviral therapy in eastern Ethiopia
Authors Mitiku H , Weldegebreal F , Teklemariam Z
Received 18 December 2014
Accepted for publication 2 March 2015
Published 12 May 2015 Volume 2015:7 Pages 137—144
DOI https://doi.org/10.2147/HIV.S79545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Shenghan Lai
Habtamu Mitiku, Fitsum Weldegebreal, Zelalem Teklemariam
Haramaya University, College of Health and Medical Sciences, Department of Medical Laboratory Sciences, Harar, Ethiopia
Purpose: The aim of this study was to assess the prevalence of opportunistic infections (OIs) and associated factors among HIV-infected adults on anti-retroviral therapy (ART) in Hiwot Fana Specialized University Hospital, Eastern Ethiopia.
Patients and methods: A hospital-based retrospective study was conducted in 358 HIV-infected adult patients on ART from April to June 2014. Data were collected through review of clinical records. The data was entered and analyzed by using SPSS version 16.0. Univariate and multivariate analyses were performed to determine the association of each independent variable with occurrence of OIs. A 95% confidence interval (CI) and P-value less than 0.05 were considered as significant association.
Results: A total of 358 patients were included in the study, in which majority (68.4%) were females. The mean age of patients was 34 (standard deviation [SD] ±9.8) years. The overall of prevalence of OIs among HIV/AIDS patients on ART was 48%. The highest prevalent rates of OIs observed were tuberculosis (TB) (21.23%), followed by Herpes zoster (11.2%) and oral candidiasis (9.5%). Baseline CD4 cell count <200 cells/mm3 (adjusted odds ratio [AOR] =1.645, 95% CI =2.187, 3.983), baseline World Health Organization (WHO) clinical stage III (AOR =2.801, 95% CI =1.958, 7.165) and IV (AOR =3.856; 95% CI =2.691, 10.390), and not using prophylaxis (AOR =1.912, 95% CI =1.444, 3.824) were found to have strong association with acquisition of OIs.
Conclusion: There was a high prevalence of OIs observed in this study. Baselines CD4 count of <200 cells/mm3, advanced WHO clinical stages, and not using prophylaxis were found to be predictors of OIs. Interventions were aimed at promoting early HIV testing and enrollment of HIV-infected individuals into ART services needed before CD4 count decreased severely.
Keywords: AIDS, CD4, prophylaxis, WHO clinical stage
Introduction
HIV causes progressive depletion of the CD4 T cells, which leads to life-threatening opportunistic infections (OIs) or malignancies during the natural course of the disease.1–5 More than 90% of OIs are responsible for the development of AIDS morbidities and mortalities.1
The most common opportunistic diseases in HIV patients in Ethiopia are oropharyngeal candidiasis and tuberculosis (TB), followed by diseases of the central nervous system (CNS), sepsis, Pneumocystis carini pneumonia (PCP), bacterial pneumonia, Kaposi’s sarcoma, and lymphoma.1 In general, milder infections such as Herpes zoster and other skin infections occur in early World Health Organization (WHO) clinical stages (stages I and II),6 whereas serious, life-threatening infections such as CNS toxoplasmosis and cryptococcal meningitis occur in later WHO clinical stages (stages III and IV) with severe immunity suppression. Some life-threatening infections, such as pneumonia and TB, may occur in early as well as in later WHO clinical stages.1,2 The risk for the development of OIs in HIV patients depends on exposure to potential pathogens, virulence of the pathogens, the degree of host immunity, and the use of antimicrobial prophylaxis.3
Antiretroviral therapy (ART) increases the length and quality of life and productivity of patients by improving survival, and decreases the incidence of OIs in HIV-infected people through reduction of the viral load and increasing the level of CD4 cells.4 The widespread use of ART has had the most profound influence on reducing OI-related mortality in HIV-infected persons in those countries in which these therapies are accessible and affordable.5,7 Worldwide, it is estimated that between 250,000 and 350,000 deaths were averted in 2005 as a result of increased treatment access.4 However, OIs continued to cause morbidity and mortality in HIV/AIDS patients even after receiving ART. This mortality occurs because some patients do not have a sustained response to antiretroviral agents for multiple reasons including poor adherence, drug toxicities, drug interactions, or initial acquisition of a drug-resistant strain of HIV-1.8,9
Despite the fact that different studies have been conducted on the prevalence of individual OIs among HIV-infected patients on ART in Ethiopia, information about the magnitude and spectrum of OIs is scarce in eastern Ethiopia. Therefore, this study tried to assess the prevalence of OIs and identify associated factors in patients taking ART drugs in Hiwot Fana Specialized University Hospital, Eastern Ethiopia.
Materials and methods
Study area, design, and period
Harari People’s National Regional State is located in the Eastern part of the Ethiopia, which is 515 kilometers away from the capital city Addis Ababa. It had a projected total population of 203,438 people in the year 2010. There are six hospitals and eight health centers in the region (Harari Peoples’ National Regional State health bureau, unpublished data, 2010). The health service coverage of the region is estimated to be about 100%. An ART program was launched on March 26, 2006 in the region. Hiwot Fana Specialized University Hospital, which is one of the hospitals in the region providing ART services to HIV/AIDs patients, began providing these services in March 2006. Until March 2014, a total of 3,290 HIV/AIDS patients have utilized ART services at this hospital.
A hospital-based, retrospective study was conducted in Hiwot Fana Specialized University Hospital ART clinic from April to June 2014. A total of 358 study participants were selected by systematic random sampling using the ART registration book as a sampling frame, and these patients’ clinical records were reviewed.
Data collection methods
Data were collected by using a checklist, which was adopted from the hospital’s clinical record format for monitoring HIV/AIDS patients on ART. Information on patients’ details, such as socio-demographic characteristics, functional status, type of OIs, prophylaxis usage, and baseline WHO clinical staging, CD4 count cell count, hemoglobin level, and weight were retrieved from clinical records of the HIV/AIDS patients by trained nurses. Those patients’ clinical records that were not complete or were missing data were omitted and were replaced with the next patient’s record on the list. The data collection format was checked for its completeness and consistency with the patient’s clinical records by a supervisor and the investigators on a daily basis.
Data entry and analysis
Data were double entered into a data entry file using SPSS software Version 16 and were analyzed according to the different variables. Results were presented by using mean, standard deviation (SD), and simple frequency tables with percentages. The prevalence of OIs was determined as the proportion of HIV/AIDS patients on ART who developed one or more OIs. Univariate and multivariate analysis logistic regression models were used to describe the significance of association between prevalence of OIs between selected variables. Crude and adjusted odds ratios (CORs and AORs, respectively) with 95% confidence intervals (CIs) were used to describe the strength of association between the selected study variables. The criterion for significance was set at P<0.05 based on a two-sided test.
Ethical considerations
The study protocol was approved by Institutional Health Research and Ethical Review Committee of the College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia. The patients’ clinical records were reviewed anonymously, and all information obtained from clinical records was kept confidential.
Results
Socio-demographic and clinical characteristics of the study participants
A total of 358 HIV/AIDS patients’ ART records were reviewed in the current study. The mean age of study participants was 34 (SD ±9.8) years and ranging from 18–71 years. Most of the patients were in the age group of 30–39 years (41.4%), were female (68.4%), urban (83%), and had an elementary school education (44.7%). Many study participants (150, or 41.9%) were at WHO clinical stage III. Concerning functional status, most (65.9%) of patients were working personnel. The majority (75.7%) of the participants were receiving cotrimoxazole, while 14.5% were receiving isonicotinylhydrazine (INH) prophylaxis. About 69% of participants had a CD4 count <200 cells/mm3. In addition, about 19.8% and 67% of participants had <10 mg/dL hemoglobin level and weighed <60 kg, respectively (Table 1).
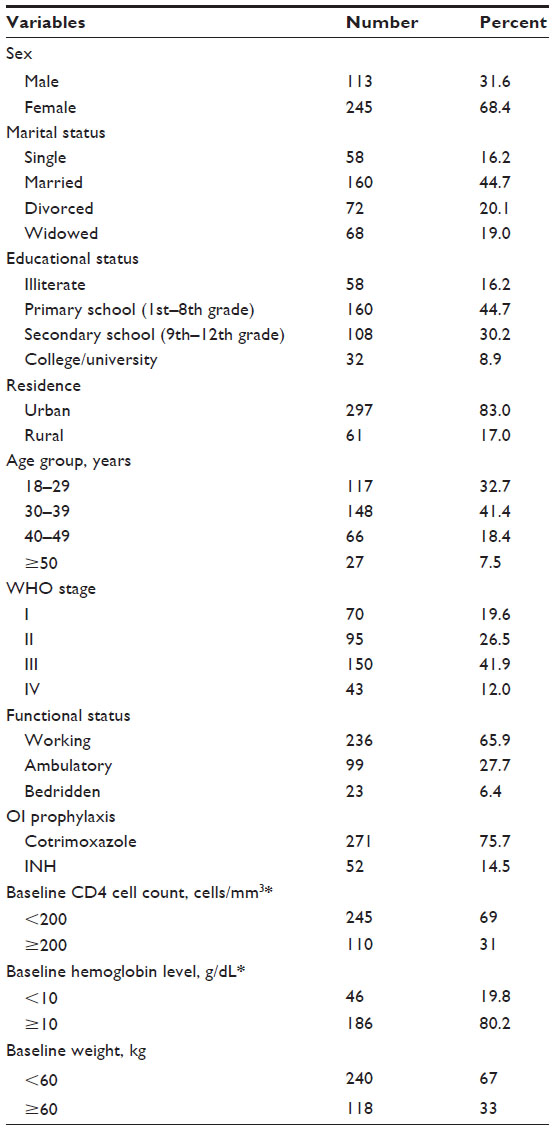 | Table 1 Socio-demographic and clinical characteristics of the study participants (n=358) at Hiwot Fana Specialized University Hospital ART Clinic, Harar, Eastern Ethiopia, 2014 |
Prevalence of OIs
Out of 358 patients, 172 had diagnosed OIs, yielding an overall prevalence of 48% (172/358). There were a total of 185 OIs diagnosed in the 172 patients. About 44.7% (160/358), 3.1% (11/358), and 0.3% (1/358) of the study participants had single, dual, and triple OIs, respectively. The most frequent OIs were TB at 21.23% (76/358), Herpes zoster at 11.2% (40/358), and oral candidiasis at 9.5% (34/358) (Table 2).
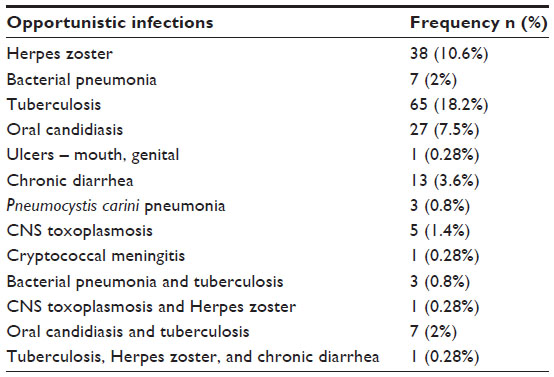 | Table 2 Prevalence of opportunistic infections among HIV/AIDS patients on ART at Hiwot Fana Specialized University Hospital ART Clinic, Harar, Eastern Ethiopia, 2014 |
Risk factors of OIs
The prevalence of OIs among males (48.7%) and females (47.8%) was comparable. The highest prevalence of OIs was found in those individuals in the age group of 30–39 years old (52.0%), with secondary school educational level (57.4%), rural dwellers (52.5%), and with body weight ≤60 kg (50.0%). However, the prevalence of OIs was not statistically different among the above variables (P>0.05).
In univariate analysis, study participants in WHO clinical stages III and IV were more likely develop OIs compared to those participants at WHO clinical stages I (COR =2.926; 95% CI =1.913, 5.768 and COR =3.654; 95% CI =2.476, 7.592, respectively). Those participants with CD4 cell counts of <200 cells/mm3 were more likely develop OIs than their counterparts with higher CD4 cell counts (COR =1.878; 95% CI =2.070, 3.298). Participants who were bedridden (COR =7.901; 95% CI =5.457, 10.217) and ambulatory (COR =4.441; 95% CI =3.687, 7.012) were more likely to develop OIs compared to patients at work during initiation of ART. In addition, participants who were not on cotrimoxazole and INH prophylaxis were more likely develop OIs (COR =1.712; 95% CI =1.348, 2.758) compared to their counterparts who were on cotrimoxazole prophylaxis (Table 3).
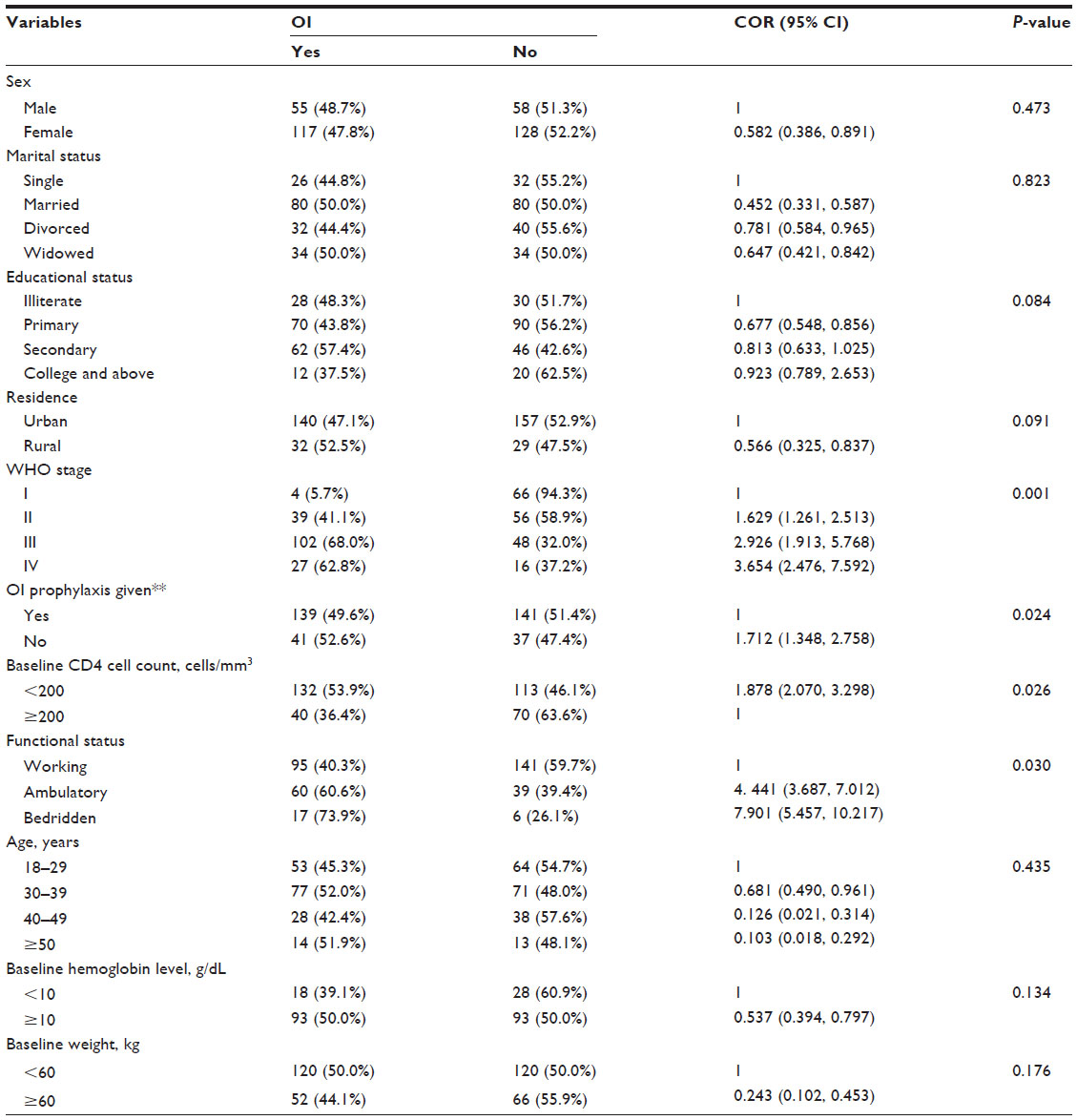 | Table 3 Univariate analysis factors associated with opportunistic infections (OIs) among HIV patients taking antiretroviral therapy (ART) at Hiwot Fana Specialized University Hospital ART Clinic, Harar, Eastern Ethiopia, 2014 |
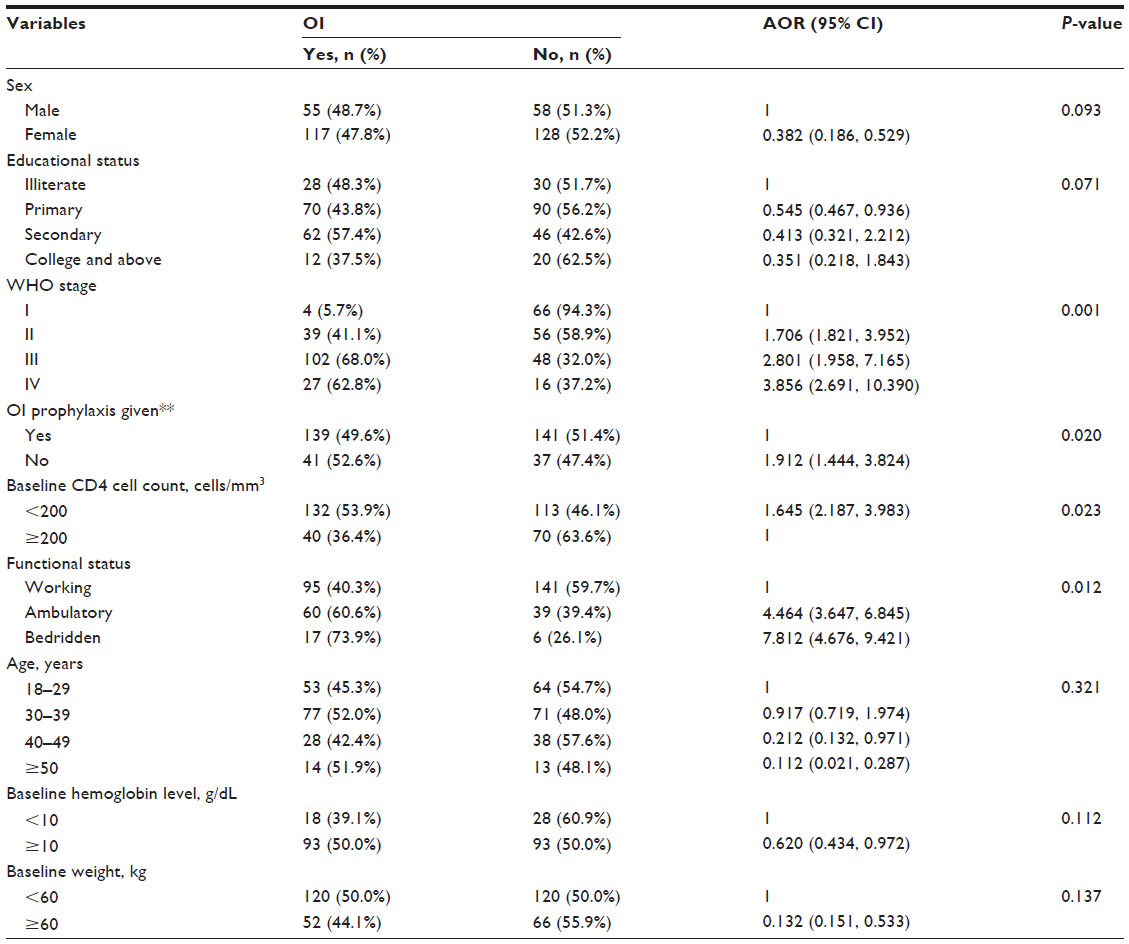 | Table 4 Multivariate analysis for selected variables with occurrence of opportunistic infections (OIs) among HIV patients taking antiretroviral therapy (ART) at Hiwot Fana Specialized University Hospital ART Clinic, Harar, Eastern Ethiopia, 2014 |
In order to determine the independent predictors of OIs, WHO clinical stages, CD4 cell count, functional status of patients at the beginning of ART, participants receiving cotrimoxazole and INH prophylaxis, educational status, hemoglobin levels, and body weight were included in multivariate analysis, as they all had P<0.25 on univariate analysis. In addition, age and sex were also included in multivariate analysis due to the consideration of associated risk of OI in prior studies.10,11
Those participants in WHO clinical stage IV were about four times (AOR =3.856; 95% CI =2.691, 10.390) and participants in WHO stage III were about three times (AOR =2.801, 95% CI =1.958, 7.165) more likely develop OIs compared to those in WHO clinical stage I. Participants with CD4 cell counts of <200 cells/mm3 were about two times (AOR =1.645; 95% CI =2.187, 3.983) more likely develop OIs compared to those with CD4 cell counts ≥200 cells/mm3. Those participants who were not on prophylaxis were about two times (AOR =1.912; 95% CI =1.444, 3.824) more likely develop OIs than those who were on prophylaxis. Those HIV/AIDS patients who were bedridden were eight times (AOR =7.812; 95% CI=4.676, 9.421) and those who were ambulatory four times (AOR =4.464; 95% CI =3.647, 6.845) more likely develop OIs when compared with patients at work.
Discussion
The current study assessed the prevalence and associated factors of OIs among HIV-positive patients taking ART. The current study found that about 48% of HIV/AIDS patients on ART had one or more OIs. This finding was comparable to the 47.6% reported in a study conducted in Taiwan.12 However, it is higher than two recent, similar studies carried out in Ethiopia in Gondor and Debre Markos, which documented 19.7% and 33.3% prevalence, respectively.11,13 This difference might be due to variation of the degree of host immunity and methodological differences in selecting study subjects. These studies were conducted among HIV patients taking ART for 5 and more years. The risk of developing an OI for a person receiving ART is highest during the initial month of therapy.14 Cohort studies carried out in Senegal15 and Taiwan12 also reported a decline of 79% in OIs among their cohorts during the 4th year of ART and 39% after 12 months of initiation of ART, respectively.
There were 12 co-infections of different OIs observed in the current study. Of these, 58.3% (n=7/12) were TB and oral candidiasis co-infections. This finding is in agreement with a report from Gondar, Ethiopia, which reported 50% TB and oral candidiasis co-infections.13 A higher proportion of TB and oral candidiasis co-infection in the current study might be explained by a higher prevalence of these two OIs among the study participants. Dual and triple OIs were also reported from studies conducted in Debre Markos, Ethiopia and Nigeria.11,16
Mycobacterium tuberculosis is the leading cause of morbidity and mortality among people living with HIV worldwide. In Ethiopia, the co-infection rate is 20%–50%, creating a dual epidemic of symptomatic HIV infection and TB. TB enhances progression of HIV infection by inducing immune activation. In addition, HIV increases the risk of infection as well as reactivation of latent TB. Hence, it is conceivable that TB can occur across the clinical spectrum of HIV infection.1
The present study also revealed that TB infection is the predominant OI identified, with a prevalence of 21.23% (76/358). This was comparable with a study conducted in Taiwan in which the prevalence of TB-related OIs was found to be 18.2%.12 However, it was higher than the prevalence reported from two areas in Ethiopia (9.7%) and Nigeria (7.7%), which also revealed TB as a major OI.11,13,16 The rate was also lower compared to a TB prevalence of 34.5% previously reported in ART-naïve, HIV-infected patients in Bahir Dar, Ethiopia.17 This might possibly be explained by methodological differences in selecting study subjects and the prevalence of TB in the general population.
Following TB, Herpes zoster and oral candidiasis were the second and the third most prevalent OIs in the present study, at 11.2% (40/358) and 9.5% (34/358), respectively. The prevalence of candidiasis was in agreement with a report from Debre Markos, Ethiopia and a report from Nigeria in which prevalence rates of 11.8% and 8.6% were noted, respectively.11,16 The prevalence of Herpes zoster is in agreement with study carried out in India, which reported prevalence of 14.7%.18 This rate was higher than the 0.6% reported from Nigeria.16 However, higher (30.7%) prevalence of Herpes zoster were reported in ART-naïve, HIV-infected patients in Bahir Dar, Ethiopia.17 This difference might be due to methodological differences in selecting study subjects and the prevalence of Herpes zoster in the general population.
The hospital where this study was conducted initiates ART when the CD4 level of a patient falls below 200 cells/mm3 of blood, which is far lower than the recommendation by WHO, which increase susceptibility of HIV-infected individuals to OIs. In the current study, HIV-infected patient with CD4 counts of <200 cells/mm3 were more likely to develop OIs compared to those with CD4 counts of ≥200 cells/mm3. This finding is concordant with other studies from Gondar, Ethiopia which reported that HIV-infected patients with CD4 counts of <200 cells/mm3 were more likely to develop OIs compared to the reference group of patients with CD4 counts >350 cells/mm.13 Other studies from India also reported high risk of developing OIs such as TB, Pneumocystis jirovecii pneumonia, and Cryptococcal meningitis among patients with CD4 counts <200 cells/mm3.18 This finding appears accurate, since CD4 cells play a central role in the activation of both humoral and cellular immune response to fight against infection. Hence, low CD4 count increases susceptibility to OIs.1,13,19
Participants with advanced WHO stages III and IV were four and three times more likely to develop OIs than those with a WHO stage of I, respectively. This finding is in agreement with two studies from Gondar and Debre Markos, Ethiopia.11,13 The study conducted in Gondor reported that WHO clinical stages III and IV HIV-infected patients were 9.4 and 22.6 times more likely to develop OIs compared to those in clinical stage I, respectively. The study conducted in Debre Markos reported that patients with advanced WHO stages III and IV were more likely to develop OIs than those with a WHO stage of I. Similar finding were also observed in studies conducted in India, South Africa, and Nigeria, which reported that advanced clinical stage of the disease were significantly associated with development of OIs among patients on ART.16,20,21
In the current study, the prevalence of OIs in those participants who were not on prophylaxis was significantly higher as compared to those who were on prophylaxis. This finding is in complete agreement with the study from Gondor, Ethiopia,13 which reported that cotrimoxazole prophylactic use is significantly associated with development of OIs among patients on ART.
Limitations
Due to the fact that data were collected from patients’ clinical records, important records of risk factors of OIs such as adherence rate to ART and prophylactic treatments was not found. The hospital where this study was conducted did not perform cultures for the diagnosis of OIs. Hence, the majority of the OIs were diagnosed clinically, which may have affected the diagnostic accuracy. Since the pre-ART burden of OIs among the patients in this study was not assessed, the rate of decline in the burden of HIV-related OIs due to ART could not be determined.
Conclusion
In this study, a high rate (48%) of OIs was observed. This suggests that OIs remain a challenge in patients receiving ART in Ethiopia. TB followed by Herpes zoster and candidiasis were the major OIs encountered by HIV-infected patients taking ART. Baseline CD4 cell count was <200 cells/mm3, baseline WHO clinical stages III and IV, and prophylaxis usage were found to be strongly associated with prevalence of OIs. Therefore, interventions need to be designed to promote early HIV testing and early enrollment of HIV-infected individuals into ART services. Individuals who continue to have low CD4 cell counts while on ART should be aggressively evaluated for OIs, and practical efforts to optimize their immunological recovery should be made. Prophylaxis should be widely implemented in the routine management of people living with HIV, irrespective of ART use.
Acknowledgments
We acknowledge Haramaya University Research and Publication Office for budget allocation and Institutional Health Research and Ethical Review Committee of the College of Health and Medical Sciences, Haramaya University, for giving ethical clearance. We also thank all individuals who have in one way or other contributed to the completion of this research.
Author contributions
HM designed the study, participated in data collection, analysis, interpretation, and write-up, drafted the manuscript, and critically revised the manuscript. ZT participated in study design, participated in data collection, analysis, interpretation, and write-up, drafted the manuscript, and critically revised the manuscript. FW participated in data collection, analysis, interpretation, and write-up, drafted the manuscript and critically revised the manuscript. All authors read and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Federal HIV/AIDS Prevention and Control Office, Federal Ministry of Health. Guidelines for Management of Opportunistic Infections and Anti-Retroviral Treatment in Adolescents and Adults in Ethiopia. 2008. Available at http://www.who.int/hiv/pub/guidelines/ethiopia_art.pdf. Accessed November 8, 2014. | |
Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America 2013. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf. Accessed November 8, 2014. | |
Chaisson RE, Moore RD. Prevention of opportunistic infections in the era of improved antiretroviral therapy. J Acquir Immune Defic Syndr Hum Retrovirol. 1997;16(Suppl 1):S14–S22. | |
Hogg R, Yip B, Kully C, et al. Improved survival among HIV-infected patients after initiation of triple-drug antiretroviral regimens. CMAJ. 1999;160:659–665. | |
Miller V, Mocroft A, Reiss P, et al. Relations among CD4 lymphocyte count nadir, antiretroviral therapy, and HIV-1 disease progression: results from the Euro SIDA study. Ann Intern Med. 1999;130: 570–577. | |
WHO case definitions of HIV for surveillance and revised clinical staging and immunological classification of HIV-related disease in adults and children [webpage on the Internet]. 2006. Available from: http://www.who.int/hiv/pub/guidelines/hivstaging/en/. Accessed March 24, 2015. | |
Dore GJ, Li Y, McDonald A, Ree H, Kaldor JM; National HIV Surveillance Committee. Impact of highly active antiretroviral therapy on individual AIDS-defining illness incidence and survival in Australia. J Acquir Immune Defic Syndr. 2002;29:388–395. | |
Federal HIV/AIDS Prevention and Control Office, Federal Ministry of Health. Guidelines for Management of Opportunistic Infections and Antiretroviral Treatment in Adolescents and Adults in Ethiopia. 2007. Available at http://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---ilo_aids/documents/legaldocument/wcms_125386.pdf. Accessed March 24, 2015. | |
Benson CA, Kaplan JE, Masur H, Pau A, Holmes KK; CDC; National Institutes of Health; Infectious Diseases Society of America. Treating opportunistic infections among HIV-infected adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association/Infectious Diseases Society of America. MMWR Recomm Rep. 2004;53(RR-15):1–112. | |
Corey DM, Kim HW, Salazar R, et al. Brief report: effectiveness of combination antiretroviral therapy on survival and opportunistic infections in a developing world setting: an observational cohort study. J Acquir Immune Defic Syndr. 2007;44:451–455. | |
Moges NA, Kassa GM. Prevalence of opportunistic infections and associated factors among HIV positive patients taking anti-retroviral therapy in Debre Markos Referral Hospital, Northwest Ethiopia. J AIDS Clin Res. 2014;5:5. | |
Sun HY, Chen MY, Hsieh SM, et al. Changes in the clinical spectrum of opportunistic illnesses in persons with HIV infection in Taiwan in the era of highly active antiretroviral therapy. Jpn J Infect Dis. 2006;59: 311–316. | |
Damtie D, Yismaw G, Woldeyohannes D, Anagaw B. Common opportunistic infections and their CD4 cell correlates among HIV-infected patients attending at antiretroviral therapy clinic of Gondar University Hospital, Northwest Ethiopia. BMC Res Notes. 2013;6:534. | |
Ledergerber B, Egger M, Erard V, et al. AIDS-related opportunistic illnesses occurring after initiation of potent antiretroviral therapy: the Swiss HIV Cohort Study. JAMA. 1999;282:2220–2226. | |
De Beaudrap P, Etard J, Diouf A, et al; ANRS 1215 Study Group. Incidence and determinants of new AIDS-defining illnesses after HAART initiation in a Senegalese cohort. BMC Infect Dis. 2010;10:179. | |
Iroezindu MO, Ofondu EO, Hausler H, Van Wyk B. Prevalence and risk factors for opportunistic infections in HIV patients receiving antiretroviral therapy in a resource-limited setting in Nigeria. J AIDS Clinic Res. 2013;3:2. | |
Abera B, Walle F, Tewabe T, Alem A, Yessin M. ART-naive HIV patients at Feleg-Hiwot Referral Hospital Northwest, Ethiopia. Ethiopian J Health Devel. 2010;24(1):3–8. | |
Wood R, Maartens G, Lombard CJ. Risk factors for developing tuberculosis in HIV-1-infected adults from communities with a low or very high incidence of tuberculosis. J Acquir Immune Defic Syndr. 2000;23: 75–80. | |
World Health Organization. Guidelines for HIV Diagnosis and Monitoring of Antiretroviral Therapy. Geneva: WHO Press; 2000. | |
Wadhwa A, Kaur R, Agarwal SK, Jain S, Bhalla P. AIDS-related opportunistic mycoses seen in a tertiary care hospital in North India. J Med Microbiol. 2007;56:1101–1106. | |
Badri M, Wilson D, Wood R. Effect of highly active antiretroviral therapy on incidence of tuberculosis in South Africa: a cohort study. Lancet. 2002;359:2059–2064. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.