")
Back to Journals » Risk Management and Healthcare Policy » Volume 7
Inpatient hospital costs and length of stay for the treatment of affective and somatoform disorders – evidence from Germany
Authors Romeyke T, Scheuer H, Stummer H
Received 4 September 2014
Accepted for publication 17 October 2014
Published 2 December 2014 Volume 2014:7 Pages 245—252
DOI https://doi.org/10.2147/RMHP.S73724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Frank Papatheofanis
Tobias Romeyke,1,2 Hans Christoph Scheuer,2 Harald Stummer1
1Department of Public Health and Health Technology Assessment: Division for Organizational Behaviour Research and Workplace Health Promotion, University for Health Sciences, Medical Informatics and Technology, Vienna, Austria; 2Department of Acute Internal and Integrative Medicine and Pain Management, Waldhausklinik Deuringen, Germany
Introduction: Diagnosis related costs analyses are the subject of science and research and are of great relevance and importance for decision makers in the hospital and for funding bodies, but also for international health policy. Up to now, standardized costs analyses with valid costs data have not been available for inpatient care of patients with affective and somatoform disorders.
Background: This clinical picture presents a major challenge for the provision of outpatient and inpatient care. An interdisciplinary approach in an inpatient setting can be beneficial for already "chronified" patients with severe forms of progression. Because of its structural and procedural demands, this type of care is associated with a greater expenditure of resources.
Methods: Costs data from the years 2008 to 2012 were analyzed for a total of 17,424 hospitalized patients in more than 200 different hospitals in Germany. The study compared the costs of treating patients with the main diagnosis affective and somatoform disorders using standardized interdisciplinary therapy, with the costs of conventional therapy.
Results: Interdisciplinary patient care is characterized by a high proportion of the costs derived from the structural and procedural implementation and the medical and nursing care. For interdisciplinary therapy with a mean period of hospitalization of 15.2 days, over 60% of the total costs were incurred by the personnel and material costs of the medical and non-medical infrastructure. The outlay is considerably greater than would be incurred by a conventional therapeutic approach without interdisciplinary therapy.
Discussion and conclusion: For the first time, detailed diagnosis-related costs data are published which were generated by consistent, standardized cost unit accounting. An interdisciplinary, holistic approach to the clinical picture results in a significant increase in costs for the hospitals.
Keywords: inpatient costs analyses, diagnosis-related costs, somatoform disorders, affective disorders, interdisciplinary approach, multimodal pain therapy
Introduction
Indication related costs analyses were previously performed for numerous diseases, for example depression with the comorbidities pain and cardiovascular diseases,1 pain in fractures caused by osteoarthritis2 and osteoporosis,3 acute coronary syndrome,4 rheumatoid arthritis,5 and end-stage cancers.6 Diagnosis related costs analyses remain at the focus of research, especially in the context of increasingly tighter funding in the health system.
Significant progress toward achieving the aim of care providers reducing the costs within the health service will be possible only on the basis of results from standardized costs analyses. This can happen at the core process level of providing care, for example through process optimization using clinical pathways7–9 or case management.10,11
Diagnosis related costs analyses impose significant economic consequences on the nation’s health care system. These analyses provide the basis for decision-making for establishing health policies in the context of demographic change. Valid costs of the performance are also the basis for management decisions.
The care provider’s main problem often lies in the lack of an exact calculation of the costs actually incurred in patient care. As a result of the lack of calculation data, there are still no binding prices in Germany for some diagnosis related groups (DRGs), although the case tariff fee system was established there more than 10 years ago. Non-calculated case tariff fees must be negotiated individually with the funding bodies. Among other things, faulty costs calculations and imprecise costs data can lead to wrong decisions in strategic hospital management and to too low agreements with the health insurance funds – resulting in financial problems for the hospitals; this can exert negative effects on patient care.
Today, distributed over the whole of Germany, specialized hospitals, clinical pain centers, and outpatient pain clinics exist at which specialist doctors, psychologists, and physiotherapists provide interdisciplinary patient care. Some hospitals currently possess in-depth expertise and experience in this area.
If the complexity and intricacy of the clinical picture of an affective or somatoform disorder is taken into account, holistic treatments12 that cover all the components of the situation can currently deliver therapeutic success – because of the numerous complex accompanying diseases often present that can increase the psychological strain the patient must endure. Holistic therapy can lead to better therapy outcomes and to greater patient satisfaction.13 On the basis of proven evidence of the benefits of an interdisciplinary therapeutic approach, the German Ministry of Health commissioned the German Institute for Medical Documentation (DIMDI) to include complex treatments in the list of therapies available as inpatient care.
The demands made of a multimodal treatment concept are high since, depending on the particular indications, this could include not only medical procedures and medication, but also psychological methods of behavioral medicine14,15 and exercise therapy adapted to the individual patient’s physical capabilities.16
The aim of the present study is to analyze cost differences between interdisciplinary and usual care treatment and to achieve complete transparency about the costs incurred by the inpatient treatment of patients with diseases in the area of affective and somatoform disorders. In order to do this, a comprehensive costs analysis in accordance with a defined standard was performed using cost unit accounting. The intention was to ascertain the costs incurred by medical, nursing, and therapeutic personnel, by the use of medication, and by taking advantage of the hospital infrastructure.
Clinical picture
Physical complaints for which no satisfactory somatic correlation can be found even after careful diagnosis are known as “medically unexplained (physical) symptoms”.17
The most frequent manifestations of medically unexplained physical symptoms are pains at different locations and functional disturbances of organs, including the vegetative symptoms, exhaustion/fatigue. It may be assumed that the quality of life of these patients is more strongly impaired than is the case for those with somatic disorders.18
This type of clinical picture is responsible for a very significant number of health service claims.19–23
Mono-causal treatments are not useful and can mask the risk of a somatic fixation.24 The outcome of interdisciplinary therapy that is prescribed too late can also be problematic.25
Interdisciplinary multimodal therapy appears to deliver useful efficacy.26 No studies currently exist which evaluate the costs using a standardized approach and which would also enable a benchmark to be set for the providers of care.
Interdisciplinary provision of services in the operations and procedures code
The (Operationen- und Prozedurenschlüssel [Operations and Procedures Code]) (OPS) is an adaptation of the International Classification of Procedures in Medicine published by the World Health Organization (WHO). The OPS is a version adapted to the requirements of the German health service. The OPS is published by DIMDI on behalf of the Federal Ministry of Health.27 The DIMDI is commissioned to publish the OPS by the Federal Ministry of Health.
The interdisciplinary therapy used in the present study was multimodal pain therapy OPS 8-918.
Structural requirements and provision of services
The code for multimodal pain therapy stipulates a minimum of 7 days interdisciplinary treatment (by legislation) of patients with chronic pain conditions (including tumor pain) with involvement of at least two specialist fields (of which one must be a psychiatric, psychosomatic or psychological discipline). Patients must have at least three of the following features:
- manifest or threatened impairment of quality of life and/or capability;
- failure of previous uni-modal pain therapy, a pain-related surgical intervention, or withdrawal treatment;
- existing medication addiction or medication abuse;
- psychological disease accompanying the pain;
- serious somatic accompanying disease.
This code requires an interdisciplinary diagnosis by at least two disciplines (compulsory psychiatric, psychological or psychosomatic-psychotherapeutic discipline).
In addition, at least three of the following active therapeutic methods must be used simultaneously: psychotherapy, physiotherapy, relaxation techniques, ergotherapy, medical training therapy, sensomotoric training, workplace training, artistic therapy (art or music therapy) or other kinds of occupational therapy. The therapy sessions last an average of 30 minutes. The code also includes an evaluation of the progression of the treatment by means of a standardized therapeutic assessment, a daily doctor’s visit or team discussion, and a weekly interdisciplinary team meeting. In group therapy, the size of the group is limited to a maximum of eight people. Use of this code requires the responsible doctor to have the additional qualification, “special pain therapy” (OPS 8-918).
The area of application in this study comprised pain therapy with the DRG U42Z. There are four pain DRGs in the German DRG system. Performance of multimodal pain therapy (OPS 8-918) in association with the main diagnosis category involves the pain DRGs I42Z, Z44Z, B47Z, and U42Z.
Methods
Costs accounting
In order to ensure that the case costs were calculated in an exact and comparable way, the procedure chosen was that of the Institute for the Hospital Reimbursement System (InEK) as described in the Costs Accounting Manual, Version 3.0. Comparison of the patients is therefore based on a standard method of costing.
The InEK is responsible for the further development and maintenance of the new reimbursement system on behalf of the autonomous partners in the German health system: the Deutsche Krankenhausgesellschaft (German Hospitals Association), the central associations of the health insurance funds, and the Verband der privaten Krankenversicherung (Association of Private Health Insurance Funds).
When a calculation of case costs is performed according to the Costs Accounting Manual, the high quality of the data is ensured by the InEK plausibility and conformity tests.
The significant steps in the costs accounting – as used in the present study – are summarized in Figure 1.
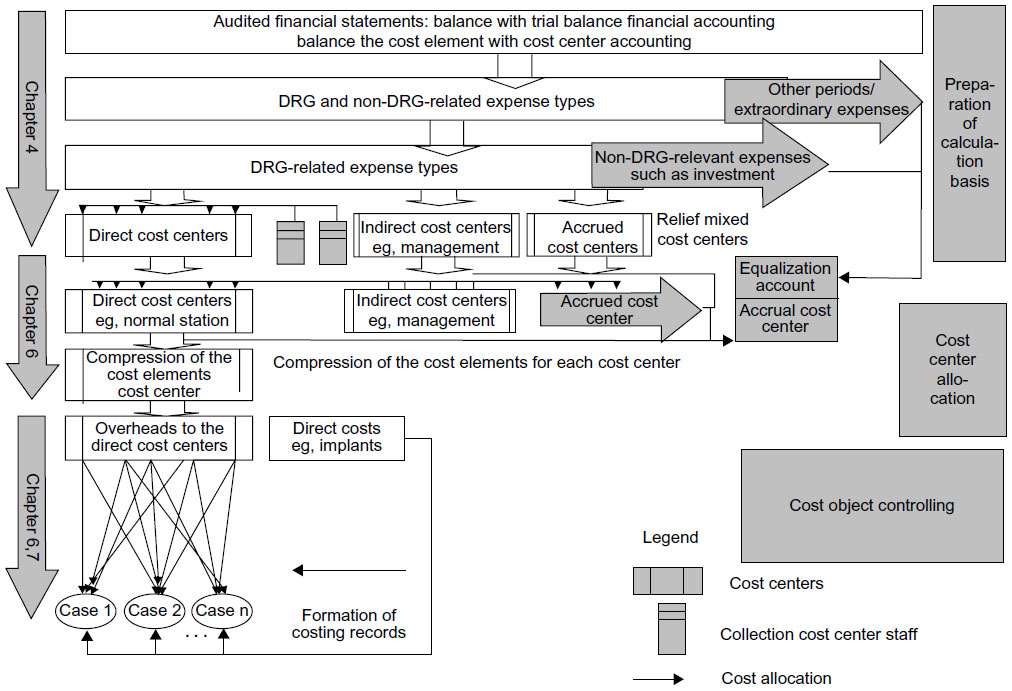 | Figure 1 Overview of the calculation steps for determining the DRG-relevant case costs, of InEK. |
First, the medical case documentation (International Classification of Diseases, [OPS]) and the usage data recorded directly in the cost centers were examined for completeness and plausibility. This is also especially important regarding relevance to the case, completeness, and differentiation, taking into account the requirements for the individual and total cost allocation.
It was also ensured that the costs listed in the latest totals and balances list were in agreement with the costs stated in the profit and loss account of the annual financial statement.
A check was also done of whether the total costs listed in the cost center accounting and the total of the individual costs agreed with the total expenditures in the financial accounting.
The organization of the cost centers and the allocation key used for the indirect cost centers were also examined. The direct cost centers to be included in the personnel costs allocation were determined and labeled.
In the course of the personnel cost allocation, the allocation formula found for the direct personnel costs resulted in a reduction for the cost centers providing services and a corresponding increase for the cost centers benefiting from services.
In the course of cost center allocation it was ensured that the costs of the indirect cost centers of the medical infrastructure were allocated to cost center group 7 (personnel and material costs of the medical infrastructure) of the direct cost centers and the costs of the indirect cost centers of the non-medical infrastructure were allocated to cost center group 8 of the direct cost centers.
Combined cost centers were created before performing the cost center allocation. A list of totals and balances for the cost centers was generated before performing the internal cost allocation. The allocation key was allocated for every indirect cost center of the medical and non-medical infrastructure.
The internal cost allocation was done on the basis of mutual clearing. The costs of the indirect cost centers of the medical and non-medical infrastructure were distributed between the direct cost centers on the basis of the allocation formula found.
In addition, the non-DRG relevant share of the allocated costs of the indirect cost centers was separated and the separated amount booked to the separation cost center. After completion of the internal cost allocation the list of totals and balances was drawn up. The list of totals and balances for the cost centers to be separated was drawn up in each case both before and after their transfer to the separation cost center.
The cost types for each direct cost center were combined into cost type groups. In the course of the cost bearer accounting the direct cost centers were allocated to cost center groups.
Those costs were then determined which are allocated as individual costs. In addition, suitable reference magnitudes were chosen for every direct cost center for the allocation of case-related costs.
After the generation of calculation rates for the direct cost centers, the joint costs of the direct cost centers were distributed using the calculation rates between the cases receiving care. The individual costs were allocated to the corresponding cost modules of the treatment cases in accordance with the consumption documentation, and the costs data were combined into cost modules.28
Table 1 contains a presentation of case-related cost modules consisting of cost type groups and cost center groups.
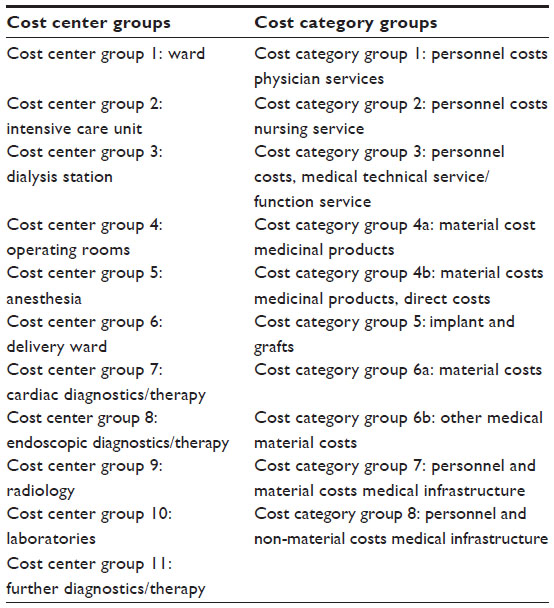 | Table 1 Cost center groups, cost category groups |
Costs data
The costs data were analyzed for a total of 17,424 hospitalized patients with diseases from the group of affective and somatoform disorders (without the application of multimodal pain therapy). The cost data of hospitals are representative. They are the result of a valid cost calculation in Germany. The basis is the standardized cost accounting scheme of the InEK.
The following main diagnosis groups were taken into account: somatization disorder, miscellaneous somatoform disorders, persistent somatoform pain disorder, somatoform disorder not further defined, undifferentiated somatization disorder, somatoform autonomous functional disorder of the upper digestive system, somatoform autonomous functional disorder of the lower digestive system.
Table 2 shows the distribution between different years of the patients and hospitals with and without interdisciplinary complex therapy (CwMT).
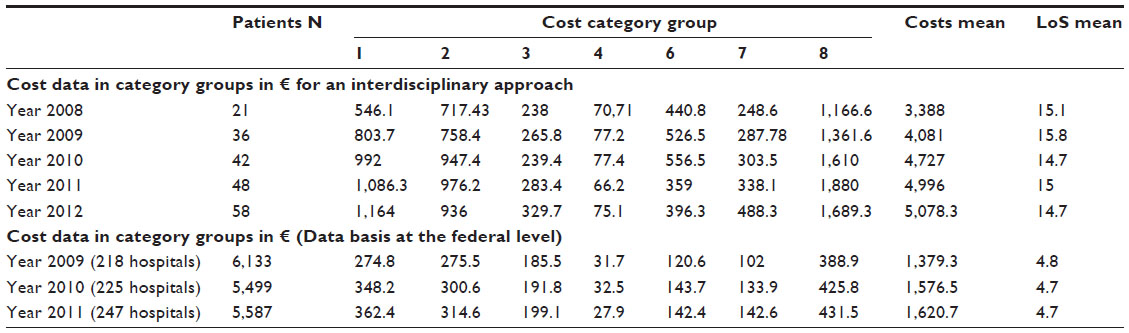 | Table 2 Overview: cost data in category groups in € |
Because costs data at national level have been unavailable up to now, cost accounting was performed for the years 2008 to 2012 for 205 cases receiving multimodal pain therapy. The procedure chosen was analogous to that of the InEK Costs Accounting Manual Version 3.0, as already described in the Methods section.
The patients included in the study also suffered from diseases from the group of somatization disorder with the same main diagnosis groups as listed above.
Both groups have the same or a similar disease picture. The basis is the International Classification of Diseases, the standard diagnostic tool for epidemiology, health management, and clinical purposes.
Insured persons in Germany have a right to full inpatient hospital treatment only if the aim of the treatment cannot be achieved by means of partial inpatient, pre- and post-inpatient or out-patient therapy including nursing care at home.
Multimodal pain therapy can be performed only on patients when specific path entry criteria are met (see Structural Requirements and Provision of Services).
Results
Analysis of costs data with multimodal pain therapy (CMT)
The analysis shows that the personnel and material costs of the non-medical infrastructure is the largest item. This includes the salaries and statutory social insurance contributions of the hospital domestic staff, the trade and supply service, and the administrative services (patient billing, personnel management and recruitment, electronic data processing). Also included are consultation fees, costs for lawyers, insurance, laundry, material costs of training and continuing education, patients’ meals, and all energy costs. Cost unit accounting revealed that an average of 34.6% of all costs are incurred by this cost category group (CCG) 8. The average costs for a single patient undergoing treatment amount to €1,541.49.
CCG 1 includes the personnel costs for the medical service, statutory social insurance contributions, costs incurred by retirement provision, and fees for doctors not employed by the hospital. Over the entire period under observation this amounts on average to 20.4% of all costs and is therefore the second largest item. Medical care of a single patient incurs average costs of €918.50.
On average over the entire period, 19.4% of the costs were due to the nursing staff (CCG 2). This includes salaries, social insurance contributions, and retirement provision. Nursing costs for a single patient amount on average to €866.71.
CCG 6 with an average of 10.6% of all costs is the fourth largest item. This comprises the material costs of medical treatment, in other words, medical and nursing material, and material requirements of physiotherapy and hygiene management. The average costs amount to €449.20.
The personnel and material costs of the medical infrastructure are recorded in CCG 7 and comprise an average of 7.4% of the total costs. They include the costs for transportation of patients, maintenance of medical technical equipment, and writing off repurchased medical consumables. The average costs per patient amount to €332.26.
An average 6.2% of the costs were incurred by CCG 3 (personnel costs of medical technical service/functional service). This includes salaries, social insurance contributions, and retirement provision. The care of a single patient results in an average of €271.26.
The material costs for drugs are recorded in CCG 4 and comprise an average of 1.6% of the costs. This consists of medicines, blood bottles, and blood plasma. The costs per patient amounted on average to €73.30.
During the period studied, the patients remained in hospital for an average of 15.08 days.
Analysis of the costs data at national level without multimodal pain therapy (CwMT)
In the year 2009 the data of 6,133 patients were evaluated (38.06% male, 61.93% female). The mean length of stay was 4.8 days with a standard deviation of 2.9 days. The costs incurred in CCG 1 and CCG 2 are equally high on average while, here too, CCG 8 with 28% accounted for the greatest share (Table 2).
The data of 5,499 patients (34.08% male, 65.92% female) were evaluated for the year 2010. The mean length of stay was 4.7 days with a standard deviation of 2.5 days. The largest share of costs resulted from CCG 8, followed by CCG 1 and CCG 2 (Table 2).
For the year 2011 the data of 5,587 patients were evaluated (34.49% male, 65.51% female); the mean length of stay was 4.5 days with a standard deviation of 2.5 days. The largest share of costs came from CCG 1 and 8, followed by CCG 2 and 3 (Table 2).
Combination of the results obtained by analysis of the years 2009–2011 shows that the largest share of costs with an average of 28% arises from CCG 8, followed by an average of 22% for CCG 1, 19% for CCG 2, 13% for CCG 3, 9% for CCG 6, 8% for CCG 7, and 2% for CCG 4.
Discussion and conclusion
Examination of the two groups surveyed in this study shows that CCG 8 (personnel and material costs of the non-medical infrastructure) was the origin of the largest expenditure for the hospital. There are several reasons why the costs of this cost bearer group are higher for CMT.
The average time of stay in the hospital in the CMT group during the period under observation (January 2008 to December 2012) was 15 days and was therefore an average of 10.3 days longer than in the CwMT. This resulted in higher costs for patients’ food, energy consumption, and for the in-house clinical personnel. The costs for patient management are also higher. High demands are placed on the documentation, the provision of care, and on patient billing. The complexity of the care processes associated with the procedures involved in providing care also made an impact as coordination costs in CCG 8.
In terms of percentage, the average cost of CCG 1 is the second largest cost group in both groups. This can be due to the fact that especially the procedures for admission and discharge of the patient generate the greatest costs. A longer time of stay for the patients in the CMT group increases the demand for resources, in particular because of the need for further medical interventions, observations of progression, and visits.
Moreover, the provision of interdisciplinary services demanded by this procedure is associated with higher costs for specialist medicine. In addition to the therapy management with the additional requirement of special pain therapy, the integration of a psychiatric, psychosomatic or psychological-psychotherapeutic discipline is required. In the present study, a specialist for psychiatry was integrated into the treatment process. The weekly, individual discussion with the doctor, which is a mandatory component of multimodal pain therapy, also contributes to the higher costs.
The costs for the nursing procedures form the third highest cost group (CCG 2) in both groups (in percentage). The average outlay for resources is significantly higher in the CMT group. This can, in particular, be due to the greater organizational demands on the nursing personnel, for example as a result of the deployment of nurses specially trained in pain management. Furthermore, the presence of complex accompanying diseases may be assumed, which can necessitate a holistic approach to nursing.29
Percentage differences are found in both groups in respect of CCG 6. The considerably greater therapy costs in the CMT group derive from the requirements of multimodal pain therapy as an interdisciplinary therapy, which requires the integration of various therapeutic specializations in the treatment process. The individual disciplines are also included at the interdisciplinary team meeting, which takes place every week. In the course of the meeting, therapeutic targets are formulated and evaluated and the treatment progression examined and documented,30 which can be reflected in higher costs.
The differences in the CCG 3, which, in this case, are much higher in percentage terms in the CwMT, can be the result of a more intensive diagnostic amount during an extensive initial examination. In the CMT an existing, confirmed diagnosis is assumed, which can incur further costs only as part of diagnostic monitoring of progression.
CCG 7 and CCG 4 will not be discussed in greater detail because here there are no major percentage deviations.
There are a lot of implications for health care provision, health policies and use. This clinical picture of affective and somatoform disorders presents like other psychiatric diseases31 a major challenge for the provision of outpatient and inpatient care worldwide. It is important to achieve complete transparency about the costs incurred by the inpatient treatment of patients with diseases in the area of affective and somatoform disorders and to analyze cost differences between interdisciplinary and usual care treatment. Diagnosis related costs analyses are the subject of science and research and are of great relevance and importance not only for decision makers in the hospital and for funding bodies, but also for health policy.
Numerous studies demonstrate the superior efficacy of interdisciplinary therapies in complex diseases compared with conventional mono-modal therapeutic approaches.32–36
For the care provider, interdisciplinary therapies are associated with a higher use of resources in comparison with uni-modal therapies.29,30
That is why in Germany, indication-related interdisciplinary care provision in the form of complex treatments has been included in the OPS, in order to properly define a holistic approach to complex clinical pictures. The complex treatments included in the OPS define specific minimum criteria for the quality of organization, procedures, and outcomes.
Further costs analyses are necessary for other clinical pictures requiring interdisciplinary inpatient therapy, especially in the context of procedure and outcome quality.
Disclosure
The authors report no conflict of interest in this work.
References
Pan YJ, Knapp M, Yeh LL, Chen YP, McCrone P. Treatment costs for depression with pain and cardiovascular comorbidities. J Psychiatr Res. 2013;47(3):329–336. | |
Le TK, Montejano LB, Cao Z, Zhao Y, Ang D. Healthcare costs associated with osteoarthritis in US patients. Pain Pract. 2012;12(8):633–640. | |
Li J, Burge RT, Ye WW, et al. Inpatient hospital costs and length of stay for the treatment of osteoporosis fractures in China. Value in Health. 2013;16(3):A220–A221. | |
Zhao Z, Zhu B, Anderson J, Fu H, LeNarz L. Resource utilization and healthcare costs for acute coronary syndrome patients with and without diabetes mellitus. J Med Econ. 2010;13(4):748–759. | |
Baser O, Burkan A, Baser E, Koselerli R, Ertugay E, Altinbas A. Direct medical costs associated with rheumatoid arthritis in Turkey: analysis from National Claims Database. Rheumatol Int. 2013;33(10):2577–2584. | |
Chastek B, Harley C, Kallich J, Newcomer L, Paoli CJ, Teitelbaum AH. Health care costs for patients with cancer at the end of life. J Oncol Pract. 2012;8(6):75s–80s. | |
Romeyke T, Stummer H. High quality at low cost – how can a clinical pathway contribute towards reconciling this apparent contradiction? IOSR Journal of Pharmacy. 2012;2(6):10–20. | |
Sylvester AM, George M. Effect of a clinical pathway on length of stay and cost of pediatric inpatient asthma admissions: an integrative review. Clin Nurs Res. 2013;23(4):384–401. | |
So JB, Lim ZL, Lin HA, Ti TK. Reduction of hospital stay and cost after the implementation of a clinical pathway for radical gastrectomy for gastric cancer. Gastric Cancer. 2008;11(2):81–85. | |
Kolbasovsky A, Zeitlin J, Gillespie W. Impact of point-of-care case management on readmissions and costs. Am J Manag Care. 2012;18(8):e300–e306. | |
Harrison JP, Nolin J, Suero E. The effect of case management on US hospitals. Nurs Econ. 2004;22(2):64–70. | |
Warner CM, Colognori D, Kim RE, et al. Cognitive-behavioral treatment of persistent functional somatic complaints and pediatric anxiety: an initial controlled trial. Depress Anxiety. 2011;28(7):551–559. | |
Romeyke T, Scheuer HC, Stummer H. Introduction of the German case tariff fee system and its effects on patient satisfaction in inpatient naturopathy. European Journal of Integrative Medicine. 2013;5(2):171–177. | |
Hamilton J, Guthrie E, Creed F, et al. A randomized controlled trial of psychotherapy in patients with chronic functional dyspepsia. Gastroenterology. 2000;119(3):661–669. | |
Hoedeman R, Blankenstein AH, van der Feltz-Cornelis CM, Krol B, Stewart R, Groothoff JW. Consultation letters for medically unexplained physical symptoms in primary care. Cochrane Database Syst Rev. 2010;12:CD006524. | |
Henningsen P, Zipfel S, Herzog W. Management of functional somatic syndromes. Lancet. 2007;369(9565):946–955. | |
McFarlane AC, Ellis N, Barton C, Browne D, Van Hooff M. The conundrum of medically unexplained symptoms: questions to consider. Psychosomatics. 2008;49(5):369–377. | |
Aiarzaguena JM, Grandes G, Salazar A, Gaminde I, Sanchez A. The diagnostic challenges presented by patients with medicallyunexplained symptoms in general practice. Scand J Prim Health Care. 2008;26(2):99–105. | |
Smith GR Jr, Monson RA, Ray DC. Patients with multiple unexplained symptoms. Their characteristics, functional health, and health care utilization. Arch Intern Med. 1986;146(1):69–72. | |
Williams ER, Guthrie E, Mackway-Jones K, et al. Psychiatric status, somatisation, and health care utilization of frequent attenders at the emergency department: a comparison with routine attenders. J Psychosom Res. 2001;50(3):161–167. | |
Schneider A, Hörlein E, Wartner E, Schumann I, Henningsen P, Linde K. Unlimited access to health care – impact of psychosomatic co-morbidity on utilisation in German general practices. BMC Fam Pract. 2011;12:51. | |
Barsky AJ, Orav EJ, Bates DW. Somatization increases medical utilization and costs independent of psychiatric and medical comorbidity. Arch Gen Psychiatry. 2005;62(8):903–910. | |
Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three decades of research. A comprehensive review. J Clin Pharm Ther. 2001;26(5):331–342. | |
Rief W, Zenz M, Schweiger U, Ruddel H, Henningsen P, Nilges P. Redefining (somatoform) pain disorder in ICD-10: a compromise of different interest groups in Germany. Curr Opin Psychiatry. 2008;21(2):178–181. | |
Bouton C, Roche G, Roquelaure Y, et al. [Management of low back pain in primary care prior to multidisciplinary functional restoration: a retrospective study of 72 patients.] Ann Readapt Med Phys. 2008;51(8):650–662. French. | |
Arnold B, Häuser W, Arnold M, et al. Multimodale Therapie des Fibromyalgiesyndroms. Systematische übersicht, Metaanalyse und Leitlinie [Multicomponent therapy of fibromyalgia syndrome. Systematic review, meta-analysis and guideline]. Schmerz. 2012;26(3):287–290. German. | |
DIMDI. Deutsche Institut für Medizinische Dokumentation und Information [German Institute for Medical Documentation]. | |
InEK, Institute for the Hospital Remuneration System. | |
Romeyke T, Stummer H. Economic of aspects of nursing in inpatient naturopathy: evidence from Germany. Nurs Econ. 2013;31(3):137–143. | |
Romeyke T, Stummer H. Interdisciplinary complex therapies in inpatient hospital treatment in Germany: Evidence from Germany. Journal of Management and Marketing in Healthcare. 2011;4(4):208–216. | |
Zeidler J, Slawik L, Fleischmann J, Greiner W. Impact and costs of hospitalisation in schizophrenia. Value in Health. 2010;13(7):A449. | |
Pfingsten M, Hildebrandt J, Leibing E, Franz C, Saur P. Effectiveness of a multimodal treatment program for chronic low-back pain. Pain. 1997;73(1):77–85. | |
Abdulrahman GO Jr. The effect of multidisciplinary team care on cancer management. The Pan African Medical Journal. 2011;9:20. | |
Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA. 2004;292(19):2388–2395. | |
Ford AC, Talley NJ, Schoenfeld PS, Quigley EM, Moayyedi P. Efficacy of antidepressants and psychological therapies in irritable bowel syndrome: systematic review and meta-analysis. Gut. 2009;58(3):367–378. | |
Stones W, Cheong YC, Howard FM. Interventions for treating chronic pelvic pain in women. Cochrane Database Syst Rev. 2005;3:CD000387. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.