")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 6
Impact of therapeutic drug monitoring of antiretroviral drugs in routine clinical management of patients infected with human immunodeficiency virus and related health care costs: a real-life study in a large cohort of patients
Authors Perrone V, Cattaneo D, Radice S, Sangiorgi D , Federici A, Gismondo MR, Medaglia M, Micheli V, Vimercati S, Pallone E, Degli Esposti L , Clementi E
Received 22 November 2013
Accepted for publication 27 February 2014
Published 14 July 2014 Volume 2014:6 Pages 341—348
DOI https://doi.org/10.2147/CEOR.S58036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Valentina Perrone,1 Dario Cattaneo,1 Sonia Radice,1 Diego Sangiorgi,2 Augusto B Federici,3 Maria Rita Gismondo,4 Massimo Medaglia,5 Valeria Micheli,4 Stefania Vimercati,5 Enza Pallone,6 Luca Degli Esposti,2 Emilio Clementi1,7
1Unit of Clinical Pharmacology, Department of Biomedical and Clinical Sciences, L Sacco University Hospital, University of Milan, Milan, 2CliCon Srl, Health, Economics and Outcomes Research, Ravenna, 3Hematology and Transfusion Medicine, Department of Clinical Sciences and Community Health, 4Clinical Microbiology Virology and Diagnosis of Bioemergency, 5Pharmaceutical Department, 6Quality Clinical Risk and Accreditation Unit, L Sacco University Hospital, Milan, 7Scientific Institute, IRCCS Eugenio Medea, Bosisio Parini, Lecco, Italy
Background: Highly active antiretroviral therapy (HAART) has reduced morbidity and mortality in patients infected with human immunodeficiency virus (HIV). Studies have documented high interindividual variability in the pharmacokinetics of antiretroviral drugs, which may impair the success of HAART if not managed properly. Therapeutic drug monitoring (TDM) is a useful diagnostic tool that helps clinicians to optimize drug doses so that drug concentrations associated with the highest therapeutic efficacy are obtained with a reduced risk of concentration-dependent adverse effects. The aim of this study was to assess whether use of TDM improves clinical outcomes and cost of illness.
Methods: A retrospective cohort study was conducted at L Sacco University Hospital in Milan, Italy, in HIV-infected patients aged ≥18 years with at least one prescription of antiretroviral drugs for which TDM was applied. The inclusion period was from January 2010 to December 2011, with a follow-up period of up to 12 months. Laboratory and administrative databases were analyzed and matched with each other.
Results: The cohort consisted of 5,347 patients (3,861 males and 1,486 females) of mean age 43.9±12.5 years. We found that TDM had been used in 143 of these patients, among whom adherence with therapy was significantly higher than among those in whom TDM had not been used (94% versus 78%). In TDM-controlled patients, the mean length of HIV-related hospitalization stay and mean cost of hospitalization were significantly reduced with respect to those observed in the group in which TDM had not been used (7.21 days versus 29.47 days and €293 versus €688, respectively).
Conclusion: Inclusion of TDM as part of routine clinical optimization of drug dosing in HIV-infected patients is associated with higher adherence to therapy, reduced length of hospitalization stay, and reduced cost of illness.
Keywords: human immunodeficiency virus, therapeutic drug monitoring, health care costs
Introduction
Human immunodeficiency virus (HIV) infection is a major public health challenge in Europe. Nearly 29,381 new diagnoses of HIV are reported yearly for European countries and the European Economic Area member states, with a rate of 5.8 diagnoses per 100,000 inhabitants.1 In Italy, an incidence of 6.5 new diagnoses of HIV per 100,000 inhabitants has been reported.2 The highest prevalence of acquired immunodeficiency syndrome (AIDS) cases and one of the highest incidence rates of new diagnosis in Italy has been observed in the Lombardy region (10.5 cases per 100,000 inhabitants), with a strong burden on the regional health care budget. In particular, the cost of antiretroviral therapy in this region has gradually increased from about €92 million in 2004 to more than €193 million in 2010.3
Use of highly active antiretroviral therapy (HAART) has reduced morbidity and mortality in HIV-infected patients.4 For those patients who have access to these drugs, life expectancy now approaches that of individuals without HIV infection, particularly if treatment is started early in the course of the disease,5,6 although a significant percentage of patients experience only a partial response to HAART. Adherence to therapy is one of the key factors that increase the efficacy of the antiretroviral response.7–9 Several studies have demonstrated that adherence is second only to CD4+ T-cell count in accurately predicting progression to AIDS and death.10,11 Other determinants of HAART failure or success include genetic differences in drug metabolism, a high baseline viral load, inherited or acquired drug resistance, concurrent opportunistic infections, and non HIV-related comorbidities.6 Studies have documented that high interindividual variability in the pharmacokinetics of antiretroviral agents plays an important role in predicting the outcome for HIV-infected patients.12–15 Inadequate exposure to antiretroviral drugs can increase the risk of a poor virologic response, whereas higher drug concentrations have been associated with an increased incidence of adverse events. Therapeutic drug monitoring (TDM) is a tool for clinicians to individualize and optimize drug dosage in order to obtain drug concentrations associated with the highest therapeutic efficacy with a reduced risk of concentration-dependent adverse effects. This approach consists of measurement of drug concentration in a biologic matrix and adjustment of the dose according to the actual drug concentration in the patient.
TDM has already been incorporated into US and Europe treatment guidelines recommending application of TDM in certain situations and special populations.15 TDM for antiretroviral agents, however, is not recommended for routine use in the management of HIV-infected adults (C-III).16 Antiretroviral monitoring remains in its infancy and there is currently no consensus about whether TDM should be used in routine clinical practice in the management of HIV infection. The current economic recession in European countries has forced governments to devise emergency measures to reduce spending on drugs, including antiretroviral therapies.17 In a context of limited health care resources, pharmacoeconomic considerations are thus crucial to help policy-makers make the most appropriate decision on resource allocation. Evidence is available from observational studies in several clinical conditions showing that TDM helps to optimize drug use and, as a consequence, also to contain disease-related costs. This has been shown for a variety of drug classes including antibiotic, antiepileptic, psychiatric, and immunosuppressant drugs.18 A recent study has shown that TDM-guided dosing of citalopram has a positive impact and decreases the duration of hospitalization.19 In particular, the introduction of TDM led to significant changes in clinical dosing strategies, ultimately resulting in a mean difference in length of hospital stay of 23 days between patients who undergo TDM and those who do not. Considering daily hospitalization costs of €250, the potential savings amounted to €5,750 per patient.
In the present study we aimed to evaluate whether TDM is a useful tool to optimize HAART and reduce the costs associated with handling HIV infection. To address this issue, we compared HIV-infected patients treated with antiretroviral drugs in which TDM was or was not used, assessing several clinical outcomes, including length of hospitalization (related to reduced therapeutic response and/or occurrence of serious adverse drug reactions) and cost of illness.
Materials and methods
Data source
Data for the study subjects were extracted from the administrative and clinical databases of L Sacco University Hospital, Milan, Italy. The following databases were used: the Health-Assisted Subjects’ Database, containing patient demographic data; the Medications Prescription Database, providing information for each medication prescription, the Anatomic Therapeutic Chemical (ATC) classification system code for the drug purchased, the number of packs, the number of units per pack, the dosages, the unit cost per pack, and the prescription date; the Hospital Discharge Database, containing information on discharge for each hospitalization, in particular the date of admission and discharge, main and accessory diagnosis coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 CM); the Ambulatory Care Specialist, which records outpatient specialist services (visits, laboratory tests, diagnostic tests) provided to the patient, including the type and date of visit; and laboratory test databases, containing information on the application of TDM in routine clinical practice for optimization of drug dosing in HIV-infected patients.
Using appropriate data linkage procedures, a population databank containing individual, analytical, and chronologic profiles of all patients enrolled was created. This administrative database is complete, includes validated data, and has been used in previous epidemiologic studies.20 The Italian Ministry of Health defined these archives as 100% complete and 95% accurate.21
In compliance with privacy laws, the patients’ identification code was encrypted and the individuals/bodies involved in processing of the data for the purposes of the analysis were blinded to the identification of patients. The patient code in each database permitted electronic linkage between all databases. In order to guarantee patient privacy, each subject was assigned an anonymous univocal numeric code. No identifiers related to patients were provided to the researchers. The local institutional ethics committee was informed of the study according to the legal requirements concerning observational analysis and waived the need for consent.
Cohort definition
This was a retrospective cohort study and included all HIV-infected patients aged ≥18 years with at least one prescription of antiretroviral drugs and routinely followed by outpatient visits at L Sacco University Hospital. The inclusion period was from January 2010 to December 2011 and the follow-up observational period was from January to December 2012 (ie, 12 months). Enrolled patients were stratified in two cohorts according to the presence/absence of at least one TDM evaluation during the inclusion period.
Antiretroviral therapy prescribed during the study period included all components of HAART, namely nucleoside analog reverse transcriptase inhibitors (NRTIs), non-nucleoside analog reverse transcriptase inhibitors (NNRTIs), protease inhibitors, or other drugs in ATC group J05A. For control patients (ie, those who did not undergo TDM evaluations) the inclusion date was the date of the first prescription of antiretroviral drugs occurring after the start date of the study including patients who were already on HAART, whereas for patients who underwent TDM, the inclusion date was that of the first assessment of TDM. The therapeutic regimen was analyzed in relation to the backbone (a combination of two NRTIs) and the third drug (usually a protease inhibitor or an NNRTI, raltegravir, or maraviroc). The chronologic analysis of prescriptions identified all therapeutic combinations and/or changes that occurred. The cohort of patients that switched to a new treatment regimen, whether or not controlled via TDM, was excluded from our study because it could have created potential bias in the evaluation, given that switching may modify clinical parameters and increase hospitalizations and therapeutic failures. Causes of hospitalization were identified by ICD-9 CM codes, and included in the analysis were those with a principal or secondary diagnosis of HIV (ICD-9 codes 042.X). Data and costs were collected for medications, hospitalizations, diagnostic tests, and specialist visits for the 12 months after the first prescription of antiretroviral therapy (follow-up). History of AIDS-defining events was evaluated in the 12 months preceding the inclusion date according to the Centers for Disease Control and Prevention classification.22 Coinfection with hepatitis B virus or hepatitis C virus was evaluated for the 12-month period preceding the inclusion date based on the presence of a hospitalization with a primary or secondary diagnosis of hepatitis B virus (ICD-9 codes 0702, 0703) and/or hepatitis C virus (ICD-9 codes 0704, 0705, 0707). Patient health status was defined by viral load and CD4+ T-cell count, evaluated at baseline and at the end of follow-up. CD4+ T-cell levels were defined to be within range when between 0.6 cells/μL and 1.5×103 cells/μL. Undetectable viral load was defined as fewer than 50 copies/mL. This analysis was done on a randomly selected sample of patients. Only patients with continuous eligibility for at least 24 months (12 months before and 12 months after the enrollment date) were included.
Adherence to therapy
Treatment adherence was calculated according to methods described in the literature.23 Adherence was determined by calculating the proportion of days on which a patient had a supplied medication in the time interval of 12 months after the enrolment date. Overall adherence for each patient was calculated as the duration-weighted average adherence of up to three regimens. Specific programming was developed to account for overlapping prescriptions, regimen modifications, and overlapping regimens to ensure that these factors did not contribute to the differences in adherence detected.
Evaluation of TDM
Plasma concentrations of antiretroviral drugs were assessed by validated chromatographic methods coupled with ultraviolet light detectors (atazanavir, darunavir, etravirine, lopinavir, tipranavir) or with triple quadrupole mass spectrometry (efavirenz, maraviroc, nevirapine, raltegravir, amprenavir, tenofovir, ritonavir, indinavir, saquinavir, nelfinavir). Plasma samples were collected for TDM after each drug reached the steady state concentration. The trough levels were measured. Reference ranges for antiretrovirals were retrieved from the recently updated US Department of Health and Human Services guidelines.16
Statistical analysis
Descriptive statistics were mainly used due to the descriptive nature of the study. Quantitative variables (eg, age) were expressed as the mean ± standard deviation or as the median (interquartile range), as deemed appropriate. Qualitative variables were expressed as absolute and relative frequencies. Incidence rates per 100 patients per year for risk of hospitalization were also reported. Patients with missing data were not included in the analyses. All analyses were performed using STATA SE version 12.0 (StataCorp LP, College Station, TX, USA) using 95% confidence intervals.
Cost analysis
Costs are reported in Euros. All health care resources for antiretroviral drug treatments (ATC code J05A), hospitalizations for HIV (ICD-9 codes 042.X; Diagnosis Related Groups 488, 489, 490), and laboratory tests/visits used during the observation period were considered in the cost of illness calculation. The price for drug treatments was the one at the time of drug purchasing, costs for visits were retrieved from regional tariffs, while the costs for the hospitalizations were derived from Diagnosis Related Group codes.
Results
Patient characteristics
Overall, 5,347 patients (3,861 males and 1,486 females) were eligible for analysis and were enrolled from January 2010 to December 2011. TDM of antiretroviral drugs was performed in 143 patients. Demographic and baseline clinical characteristics of the study population are shown in Table 1. The mean patient age was 43.9±12.5 years (P=0.706). No relevant difference in demographic characteristics or HAART therapy regimes that could have introduced potential sources of biases was observed. No differences in coinfections with hepatitis B and C virus were observed either. Presence of at least one AIDS-defining conditions was found in 7% versus 5% (P=0.417) of patients who did or did not undergo TDM (TDM+ and TDM−, respectively). Ninety-four percent of the TDM+ group versus 72% of the TDM− group (P<0.001) had been treated with antiretroviral drugs before the observational study period. During the study period, 40 of the 143 TDM+ patients (28%) were switched to a new treatment regimen versus 1,056 of the 5,204 TDM− patients (20.3%). Adherence was significantly higher in TDM+ patients versus TDM− patients (94% versus 78%, P<0.001, Figure 1).
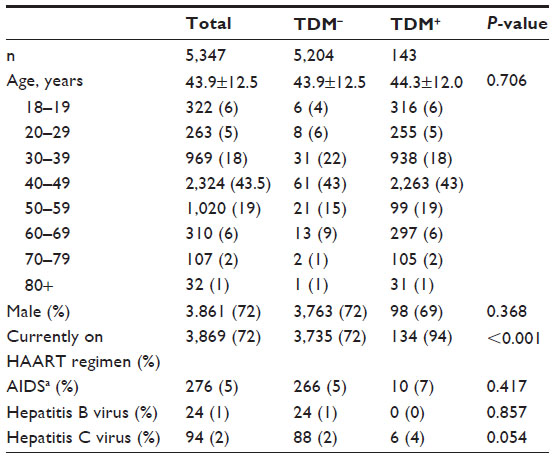 | Table 1 Demographic characteristics |
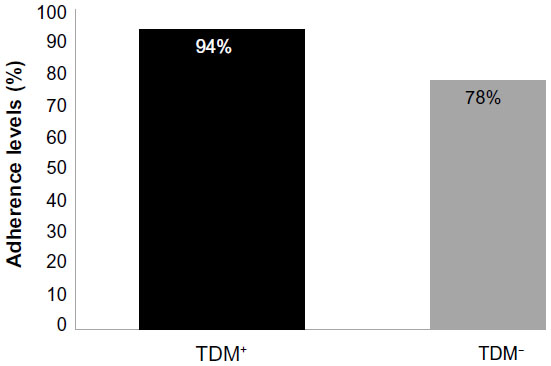 | Figure 1 Adherence to HAART regimens. |
TDM and immunovirologic outcome
At the end of the follow-up period, the percentage of patients with a viral load <50 copies/mL was 85.3% in TDM+ patients and 81.4% in TDM− patients (P=0.474). No difference was observed between the TDM+ and TDM− patients with regard to whole CD4+ T-cell count or the percentage of patients with a CD4+ T-cell count within the therapeutic range (P=0.917, Figure 2).
 | Figure 2 Viral load and CD4+ T-cell counts. |
TDM and costs related to patient management
No significant differences were detected between the TDM+ group and the TDM− group in terms of number of patients hospitalized during the observation period (P=0.623). However, the mean length of HIV-related hospitalization stay was 7.21 days in the TDM+ group versus the 29.47 days observed in the TDM− groups. The costs of illness reflecting the difference in adherence and hospitalization parameters between the TDM+ and TDM− groups are shown in Figure 3. The mean health care cost per patient in the TDM+ group was €12,042. Patients in the TDM− group showed a significantly lower mean cost of €10,227 (P=0.004). The difference in overall costs between the two groups is a consequence of the higher adherence level for TDM+ patients, who also showed incremental consumption of the following resources: specialist examinations (€2,493 versus €1,278), current antiretroviral regimen (€9,021 versus €8,066), and concomitant medications (€235 versus €195), which were the factors leading to increased health care costs in these patients. In contrast, during the same observation period, the average cost of hospitalization was significantly higher in the group without TDM (€688 versus €293). The difference in hospitalization costs between the two group was thus €395 per patient.
 | Figure 3 Cost of illness. |
Discussion
Because of the massive and growing public health impact of HIV infection, knowledge of its economic implications is urgently required for practical purposes. In an era when health care budgets are under increasing pressure, individual HIV care providers, administrators, and national and international scientific steering committees for HIV-infected cohorts will play a crucial role in promoting the collection of high-quality and detailed data on all components of resource use and costs of care.24 Decision-makers and health planners require this information for several purposes: to quantify current expenditures and to project future direct medical costs associated with HIV management; to evaluate the impact of policy decisions; and to assess the economic consequences of different treatment options in health care management.25 Poor virologic response or toxicity are the most frequent reasons for discontinuation or switch of first-line antiretroviral therapy.26 Consequently, it is now mandatory to investigate the variables affecting the clinical outcome in HIV-infected patients, since such understanding is crucial to being able to tailor antiretroviral regimens according to patient characteristics in order to increase the probability of tolerability of combination antiretroviral therapy, enjoying longer survival, and having better quality of life. Within this context, TDM-guided intervention could help to extend the effectiveness of individual treatments and to reduce the use of costly drugs. Previous studies have documented that TDM for some antiretroviral drugs, namely protease inhibitors and NNRTIs, is associated with important improvements in the response of HIV-infected patients to HAART, in terms of increased efficacy13–15,27 and/or improved drug safety.14,28 In this study, we extended those findings by investigating the impact of TDM on health costs in a real life scenario, considering at the same time demographic, clinical, and laboratory variables known to influence the response to antiretroviral therapy. A first important observation is the low proportion of patients who underwent TDM of antiretroviral drugs for optimization of their dosing, which most likely reflects the fact that such assessments were not done systematically but rather requested within a context of individual clinical problems. As a consequence, it can be reasonably assumed that TDM is not used yet as a diagnostic tool for the day-by-day management of antiretroviral therapy in the context of HIV. Our results suggest also that in clinical practice the choice of the clinician to use TDM is based on its suitability to contribute towards solving specific clinical scenarios such as uncertain compliance, poor response to therapeutic doses,29 or to determine dose reductions without risking loss of efficacy. Of importance, there were no significant differences between the TDM− and TDM+ groups with regard to demographic and laboratory covariates nor in coinfections at baseline that may have justified the need or otherwise for TDM. In this respect, our results are in line with those of a previous study, although in a selected group of patients, suggesting that TDM is a promising strategy for increasing the success of antiretroviral therapy.30 However, larger well designed trials are required in order to assess conclusively the potential utility of TDM-based intervention before it can be definitely recommended for routine clinical practice.
It is well known that good adherence to antiretroviral therapy is necessary for success of treatment.31,32 A recent study33 also showed that nearly 42% of patients (672 of 1,605 eligible participants) were hospitalized for one or more days after initiating HAART. Median adherence levels were 92 (interquartile range 58–100) and 100 (interquartile range 83–100) among those hospitalized and those never hospitalized, respectively. After controlling for confounders, those with <95% adherence had a 1.88-fold (95% confidence interval 1.6–2.21) higher risk for hospitalization. Identifying and addressing factors contributing to poor adherence in the early treatment period could improve patient care and lower hospitalization costs. Although poor adherence is one of the most important factors in the development of virologic failure, applying TDM in this setting represents a challenge.34 Numerous approaches have been used to evaluate adherence, including patient self-reports, physician assessment, electronic monitoring, pill count, and prescription refill compliance.35 Using these approaches, TDM was found to enhance adherence, the most likely reason being that it enhances patient awareness of the therapy and the sense of being properly taken care of.36,37 Only the association of therapeutic failure with the detection of subtherapeutic or more specifically null drug levels is a strong indicator of noncompliance with treatment. Our data show that the cohorts of patients we studied did not differ in demographic/confounding factors, leaving TDM as the main critical difference and thus the variable affecting adherence to treatment. Suboptimal adherence among HIV-infected patients taking HAART may also predict hospitalization. Overall, cost models have shown that high levels of adherence are associated with overall lower total health care costs in the USA38 and South Africa.39 Timely and practical combination of antiretroviral therapy adherence monitoring and interventions are thus advisable for HIV/AIDS programs in both developed and developing countries. Our results support this evidence, by demonstrating that use of TDM was associated with a reduction in the length of hospital stay from 29.47 days to 7.21 days per patient. Thus, it can be reasonably hypothesized that use of TDM in routine clinical management of HIV-infected patients has a positive impact on the duration and cost of hospitalization. Indeed, in our cohort, the cost of hospitalization per patient was €395 less in the TDM+ group than in the TDM− group. This does not cover the increased cost due to the mean health care per patient, that was €1,815 more in the TDM+ group, a value including also the costs incurred to analyze the plasma drug concentrations. It does not cover the costs for a specialized clinical laboratory to perform quantitation of antiretroviral concentrations, that includes high-performance liquid chromatography and tandem mass spectrometry; these may cost in the range of €200,000. This implies that, to be cost-effective, TDM has to be performed in centralized structures servicing more than one hospital. This is related to a considerably higher adherence level that in the long run will benefit the patient and reduce costs further. The reduced costs of hospitalization may also impact positively long term on health care resources because of the reduced number of hospital beds and associated health care operators required, although the possible longer life expectancy of TDM+ patients might lead to higher lifetime costs per patient. Despite the demonstrated relevance of TDM, there are still some problems that limit its use in routine clinical practice. These include timing of sample collection for TDM and the presence of confounding factors, such as virologic and immunologic parameters, protein binding, intracellular kinetics, and the nature of combination therapy, which may also complicate the interpretation of TDM results. Nevertheless, TDM has already been incorporated in the treatment guidelines from the USA and Europe. Our results provide the first evidence that introducing TDM for HIV-infected patients is not only a useful tool to improve the response of patients to HAART, but is also potentially cost-effective.
A limitation of this study was that the differences between the TDM and non-TDM groups were not fully explored and we do not have enough information to run a univariate or multivariate analysis adjusting for potential confounders and allowing determination of whether hospitalization or admission costs truly differ by use of TDM. The limited number of patients in some of the comparisons was a challenge. Some numeric differences did not reach statistical significance, and this might be due to lack of power. Missingness is a common problem in register-based observational studies. In our study, missingness did not differ among drugs. However, due to the limitations described above, the results of this study have to be interpreted with caution. Finally, we excluded evaluation of patients that incurred in drug switches. This was due to a limitation of the database, that it does not provide the reason behind the drugs switches.
Conclusion
We found that inclusion of TDM as part of the clinical routine for optimization of drug dosing in HIV-infected patients is associated with higher adherence to therapy, fewer hospitalizations, and a significant reduction in the cost to health care systems. Ongoing research on TDM may provide a useful tool for future improvement of HAART. In a context of limited health care resources, pharmacoeconomic considerations are crucial to help policy-makers in making the most appropriate decisions regarding resource allocation. In the case of antiretroviral drugs, such decisions may not be in contrast with optimal treatment for patients.
Acknowledgments
We are indebted to the technicians in the Unit of Clinical Pharmacology, Department of Biomedical and Clinical Sciences, L Sacco University Hospital, who performed drug level determination in the TDM samples.
Author contributions
EC, LDE, SR, and DC conceived the study, analyzed and interpreted the data, contributed to the drafting of the article, revised it, and approved the final version. VP conceived the study, acquired and analyzed the data, drafted the article, and approved the final version. DS, SV, VM, and EP contributed to the design of the study, acquired and analyzed the data, revised the article, and approved the final version. ABF, MRG, and MM contributed to the conception of the study, acquisition and interpretation of the data, and critical revision of the article, and approved the final version. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
The authors declare that they have no competing interests in this work.
References
Centers for Disease Control and Prevention. Surveillance Report – HIV/AIDS surveillance in Europe 2012. Atlanta, GA, USA: Centers for Disease Control and Prevention; 2013. | |
Centro Operativo AIDS dell’Istituto Superiore di Sanità (ISS). Not Ist Super Sanità 2013;26(9 Suppl 1):3–47 I. | |
Lombardy Region. [Therapeutic and Diagnostic Path for the patient with HIV disease]. Milan, Italy: Lombardy Region; 2011. Decree no 7485. Available from: http://www.sanita.regione.lombardia.it/cs/Satellite?c=Page&childpagename=DG_Sanita/Page/NormativaDetail&pagename=DG_SANWrapper&cid=1213275902673&keyid=3520. Accessed April 5, 2014. Italian. | |
Mocroft A, Ledergerber B, Katlama C, et al. Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet. 2003;362(9377):22–29. | |
Nakagawa F, Lodwick R, Costagliola D, et al. Calendar time trends in the incidence and prevalence of triple-class virologic failure in antiretroviral drug-experienced people with HIV in Europe. J Acquir Immune Defic Syndr. 2012;59(3):294–299. | |
Gazzard BG, Anderson J, Babiker A, et al. British HIV Association Guidelines for the treatment of HIV-1-infected adults with antiretroviral therapy 2008. HIV Med. 2008;9(8):563–608. | |
Lima VD, Harrigan R, Bangsberg DR, et al. The combined effect of modern highly active antiretroviral therapy regimens and adherence on mortality over time. J Acquir Immune Defic Syndr. 2009;50(5):529–536. | |
Garcia de Olalla P, Knobel H, Carmona A, Guelar A, Lopez-Colomes JL, Cayla JA. Impact of adherence and highly active antiretroviral therapy on survival in HIV-infected patients. J Acquir Immune Defic Syndr. 2002;30(1):105–110. | |
Cooke CE, Lee HY, Xing S. Adherence to antiretroviral therapy in managed care members in the United States: a retrospective claims analysis. J Manag Care Pharm. 2014;20(1):86–92. | |
Weiss L, French T, Finkelstein R, Waters M, Mukherjee R, Agins B. HIV-related knowledge and adherence to HAART. Aids Care. 2003;15(5):673–679. | |
Knobel H, Carmona A, Grau S, Pedro-Botet J, Diez A. Adherence and effectiveness of highly active antiretroviral therapy. Arch Intern Med. 1998;158(17):1953. | |
Back D, Gatti G, Fletcher C, et al. Therapeutic drug monitoring in HIV infection: current status and future directions. AIDS. 2002;16 Suppl 1:S5–S37. | |
Pretorius E, Klinker H, Rosenkranz B. The role of therapeutic drug monitoring in the management of patients with human immunodeficiency virus infection. Ther Drug Monit. 2011;33(3):265–274. | |
Khoo SH, Gibbons SE, Back DJ. Therapeutic drug monitoring as a tool in treating HIV infection. AIDS. 2001;15 Suppl 5:S171–S181. | |
Liu X, Ma Q, Zhang F. Therapeutic drug monitoring in highly active antiretroviral therapy. Expert Opin Drug Saf. 2010;9(5):743–758. | |
AIDS Info. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Available from: http://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-treatment-guidelines/0. Accessed April 4, 2014. | |
Llibre JM, Cardona G, Santos JR, et al. Antiretroviral treatment switch strategies for lowering the costs of antiretroviral therapy in subjects with suppressed HIV-1 viremia in Spain. Clinicoecon Outcomes Res. 2013;5:215–221. | |
Touw DJ, Neef C, Thomson AH, Vinks AA. Cost-effectiveness of therapeutic drug monitoring: a systematic review. Ther Drug Monit. 2005;27(1):10–17. | |
Ostad Haji E, Mann K, Dragicevic A, et al. Potential cost-effectiveness of therapeutic drug monitoring for depressed patients treated with citalopram. Ther Drug Monit. 2013;35(3):396–401. | |
Di Bari M, Balzi D, Roberts AT, et al. Prognostic stratification of older persons based on simple administrative data: development and validation of the “Silver Code,” to be used in emergency department triage. J Gerontol A Biol Sci Med Sci. 2010;65(2):159–164. | |
Ministry of Labour, Health and Social Policies. Annual report on the hospitalization activity. 2005. Available from: http://www.ministerosalute.it/programmazione/sdo/sezDocumenti.jsp?id=148&label=osp. | |
Schneider E, Whitmore S, Glynn KM, Dominguez K, Mitsch A, McKenna MT. Revised surveillance case definitions for HIV infection among adults, adolescents, and children aged <18 months and for HIV infection and AIDS among children aged 18 months to <13 years – United States, 2008. MMWR Recomm Rep. 2008;57(RR–10):1–12. | |
Gardner EM, Burman WJ, Maravi ME, Davidson AJ. Selective drug taking during combination antiretroviral therapy in an unselected clinic population. J Acquir Immune Defic Syndr. 2005;40(3):294–300. | |
Levy A, Johnston K, Annemans L, Tramarin A, Montaner J. The impact of disease stage on direct medical costs of HIV management: a review of the international literature. Pharmacoeconomics. 2010;28 Suppl 1:35–47. | |
Gebo KA, Chaisson RE, Folkemer JG, Bartlett JG, Moore RD. Costs of HIV medical care in the era of highly active antiretroviral therapy. AIDS. 1999;13(8):963–969. | |
Mocroft A, Youle M, Moore A, et al. Reasons for modification and discontinuation of antiretrovirals: results from a single treatment centre. AIDS. 2001;15(2):185–194. | |
Schoenenberger JA, Aragones AM, Cano SM, et al. The advantages of therapeutic drug monitoring in patients receiving antiretroviral treatment and experiencing medication-related problems. Ther Drug Monit. 2013;35(1):71–77. | |
Back DJ, Khoo SH, Gibbons SE, Merry C. The role of therapeutic drug monitoring in treatment of HIV infection. Br J Clin Pharmacol. 2001;51(4):301–308. | |
Hiemke C, Baumann P, Bergemann N, et al. AGNP consensus guidelines for therapeutic drug monitoring in psychiatry: update 2011. Pharmacopsychiatry. 2011;44(6):195–235. | |
Fabbiani M, Di Giambenedetto S, Bracciale L, et al. Pharmacokinetic variability of antiretroviral drugs and correlation with virological outcome: 2 years of experience in routine clinical practice. J Antimicrob Chemother. 2009;64(1):109–117. | |
Tsasis P. Adherence assessment to highly active antiretroviral therapy. AIDS Patient Care STDS. 2001;15(3):109–115. | |
Bangsberg DR, Perry S, Charlebois ED, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15(9):1181–1183. | |
Fielden SJ, Rusch ML, Yip B, et al. Nonadherence increases the risk of hospitalization among HIV-infected antiretroviral naive patients started on HAART. J Int Assoc Physicians AIDS Care (Chic). 2008;7(5):238–244. | |
Gunda DW, Kasang C, Kidenya BR, et al. Plasma concentrations of efavirenz and nevirapine among HIV-infected patients with immunological failure attending a tertiary hospital in North-Western Tanzania. PLoS One. 2013;8(9):e75118. | |
Arnsten JH, Demas PA, Farzadegan H, et al. Antiretroviral therapy adherence and viral suppression in HIV-infected drug users: comparison of self-report and electronic monitoring. Clin Infect Dis. 2001;33(8):1417–1423. | |
Reeve E, Wiese MD. Benefits of deprescribing on patients’ adherence to medications. Int J Clin Pharm. 2014;36(1):26–29. | |
Goicoechea M, Best B, Seefried E, Wagner G, Capparelli E, Haubrich R. Failure of modified directly observed therapy combined with therapeutic drug monitoring to enhance antiretroviral adherence in a patient with major depression. AIDS Patient Care STDS. 2006;20(4):233–237. | |
Freedberg KA, Hirschhorn LR, Schackman BR, et al. Cost-effectiveness of an intervention to improve adherence to antiretroviral therapy in HIV-infected patients. J Acquir Immune Defic Syndr. 2006;43 Suppl 1:S113–S118. | |
Nachega JB, Leisegang R, Bishai D, et al. Association of antiretroviral therapy adherence and health care costs. Ann Intern Med. 2010;152(1):18–25. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.