")
Back to Journals » Patient Preference and Adherence » Volume 8
How patients experience the surroundings in relation to patient participation: a qualitative study of inpatients with intestinal failure
Authors Thyssen GD, Beck A
Received 21 December 2013
Accepted for publication 29 January 2014
Published 28 April 2014 Volume 2014:8 Pages 585—592
DOI https://doi.org/10.2147/PPA.S59554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Gunvor Dichmann Thyssen, Anne Beck
Department of Hepatology and Gastroenterology, Aarhus University Hospital, Aarhus, Denmark
Introduction: Patient participation is known to improve patients' motivation, compliance, treatment results, and satisfaction with the received care. It is well known that the physical environment is of great importance in supporting patient involvement. A systematic literature search has shown a lack of articles on the subject of “surroundings” in relation to patient participation, for all patient groups.
Aim: We aimed to investigate how patients with intestinal failure experience their hospital surroundings in relation to patient participation.
Methods: The study included eight patients admitted for at least 2 weeks at the Intestinal Failure Unit, H8, Salford Royal NHS Foundation Trust, Manchester, United Kingdom. Included patients had a good level of consciousness with no confusion. The included patients participated in a semistructured interview. The interviews were analyzed using Malterud's principles of systematic text condensation.
Results: The patients described that the surroundings enabled them to participate in their treatment and care. The surroundings made it possible for them and encouraged them to participate through: the possibility to seek and get information and the possibility to participate in daily activities. This led to a feeling of independence, reassurance, normality, control, responsibility, and confidence.
Conclusion: The findings in this study indicate that the hospital surroundings are essential for the patients with respect to their ability to participate in their own care and treatment. The surroundings, in relation to patient participation, should be considered when planning and organizing nursing care. Further research is needed to increase the understanding of the surroundings in relation to patient participation - this research could, for eg, include the nurse's perspective.
Keyword: patient perspective, patient involvement, patient environment, emotional consequences
Introduction
The focus on patient participation has increased during the last decades,1–4 and patient participation is described as a well-established and highly valued concept in medical practice.2
Over the past 40 years, the patient position has shifted from that of a passive recipient to one of an active participant who is involved in decisions on treatment and care.1,4–6 Additionally, the increased amount of available information, technological developments in health care, and an increase in number of patients with chronic diseases has led to a more active involvement of patients.4,5,7
Intestinal failure (IF) has recently been defined as occurring “when there is reduced intestinal absorption so that macronutrient and/or water and electrolyte supplements are needed to maintain health and/or growth”.8,9 IF can develop into a chronic condition,8 and in this situation, patient participation is of great importance to increase the level of self-care.2 Literature on patient participation in patients with IF is lacking.
Patient participation has been defined by Sahlsten et al as an established relationship between nurse and patient wherein there is surrender of some power or control by the nurse, shared information and knowledge, and an active engagement together in intellectual and/or physical activities.10 However, in other studies, there has been no consensus on the definition of patient participation in nursing care.11
Several studies on chronic patients indicate that patient participation improves patients’ motivation, compliance, treatment results, and satisfaction with the received care.12–18 However, studies have shown that both patients and nurses face barriers related to patient participation.11,19 In a qualitative study by Sahlsten et al, nurses described “the environment” as one of several barriers to patient participation. Examples of this could be inadequate facilities, limited space, or lack of right equipment.20
A systematic literature search has shown a lack of articles on the subject of “surroundings” in relation to patient participation, for all patient groups. A study by Ryden from 1985 indicated that the physical environment was relevant for patient autonomy. The environment is especially important when it comes to a lack of space that limits the patients’ autonomic function.21 An article by Giloth in 1990 described that the physical environment is of great importance in supporting patient participation, ie, access to kitchen, lounge, library, and rooms providing privacy.22
The aim of this study was to investigate how patients with IF experience the surroundings in relation to patient participation.
Methods
A phenomenological hermeneutical approach was used. This method was chosen for its ability to clarify the meaning of lived experience and to gain insight about the patient’s world.23
Exchange visit
The investigators had 6 weeks of observation as part of an exchange visit at the Intestinal Failure Unit, H8, Salford Royal NHS Foundation Trust, Manchester, United Kingdom, in the autumn of 2013.
Through observations, the investigators conceived the notion that the surroundings were of great importance in relation to patient participation. At the Intestinal Failure Unit, patients had access to a kitchen, a launderette, a day room, a sluice room, a medicine cabinet, and they each had a notebook and two blackboards.
Participants
The patient group consisted of eight patients with IF who were admitted to the Intestinal Failure Unit. The selection of patients was purposeful, and the patients were included in collaboration with the nurses from the unit. The inclusion criteria were: 1) a high level of consciousness, with no confusion; and 2) admission to the unit for at least 2 weeks (to ensure that the patients had knowledge about the surroundings).
The participants included five women and three men. The age range was 18–59 years. Patients were included in interviews until saturation, when no additional or new data involving the experience of the surroundings in relation to patient participation were identified, in accordance with the study design.24
Interviews
Data were collected through semistructured interviews. The intention was to explore the participants’ experiences in depth. Each interview lasted approximately 20 minutes. Interviews were audio-recorded and transcribed verbatim.
If the patient was mobile, the interview was conducted in a private room at the unit. Otherwise, the interview was performed at the patient’s bedside, behind drawn curtains. The same investigator performed all the interviews, while the other investigator observed, took notes, managed a voice recorder, and asked any additional questions.
An interview guide containing four questions was used to structure the interview (Table 1). The guide was pilot-tested in one interview, to ensure quality and usefulness.
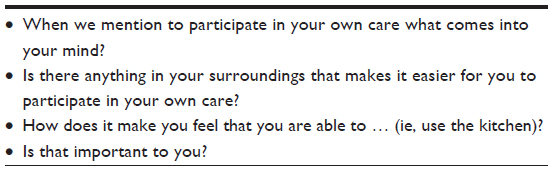 | Table 1 Interview guide |
Ethical considerations
All patients provided written informed consent in accordance with Ethical Guidelines for Nursing Research in the Nordic Countries.25 All patients were informed about voluntariness, anonymity, confidentiality, publication, and their right to withdraw from the study at any time without consequence. The patients were informed that they could choose any time of the day for the interview. This assured the investigator of the patients’ ability to be committed to the interview.
The study was approved by the Danish Data Protection Agency.
Analysis
Malterud’s principles of systematic text condensation were used.26,27 The principles of systematic text condensation involve four steps.27
First, the investigators read the interviews as a whole to get an overall impression. Temporary themes were created.
Second, the interviews were decontextualized. The investigators identified meaning units (quotations or words) matching the temporary themes. These meaning units were parts of the text that were found to express important themes for understanding how patients with IF experienced the surroundings, in relation to patient participation.
The third step was estimation of the temporary themes and the matching meaning units, and artificial quotes were made for each theme. After reading the artificial quotes, the final themes were identified.
In the fourth and final step, the final themes were converted into an analytical text, constituting the findings in this study. The interviews were recontextualized to ensure that the investigators were faithful to the source data. The analysis process is described in Table 2. The analytical text consisted of interview statements, descriptions, and opinions about the surroundings in relation to patient participation. These statements, descriptions, and opinions were selected to describe the surroundings as a phenomenon and the extent to which it was important to the patients in relation to patient participation. Furthermore, the investigators paid special attention to the aspects of surroundings in relation to patient participation that were repeated throughout the different interviews.
 | Table 2 Analysis process |
The investigators collaborated throughout the whole analysis process and completed all steps together.
Findings
Two major themes emerged from the interviews: “enabled through the surroundings” and “emotional experiences.” Each theme had underlying subthemes. Figure 1 illustrates the connection between the major themes and subthemes.
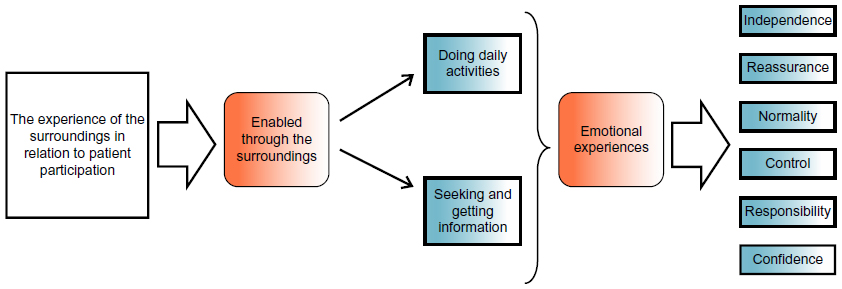 | Figure 1 Patients’ experience of the surroundings in relation to patient participation. |
Enabled through the surroundings
This theme illustrates that the surroundings enabled the patients to participate in their treatment and care. The surroundings made it possible for them and encouraged them to participate, through the possibility of seeking and getting information and the possibility of participating in daily activities. This major theme had two subthemes: doing daily activities and getting and seeking information.
Doing daily activities
The patients expressed that the surroundings enabled them to manage daily activities by themselves. Particularly, the ability to make themselves a cup of tea or something to eat, do their own laundry, to measure intake and output (fluids, urine, vomit, and feces), and to self-medicate was of great importance to them. One patient expressed:
The patients want to be able to look after their own stoma bags, they want to be able to, you know, go in the kitchen and make a brew and use the laundry. And it is a big help.
Furthermore, patients had the impression that the staff expected and encouraged them to participate in daily activities:
That was the first thing I found when I came here, that the matron showed me around and she said, “We have got the activity room, the day room, and we encourage you to go and take part in things and get involved.”
When talking about the surroundings, space was mentioned as being important in relation to participation. By having ample space to move around and thereby, being able to carry out daily activities, increased participation:
But just having the space to move around and make your bed and sit and … that makes a huge difference.
Furthermore, space was described as reducing the feeling of claustrophobia and increasing the feeling of relaxation and privacy. Having “your own space” was mentioned as a basic human need and could improve patient participation.
Getting and seeking information
The patients described that the surroundings enabled them to get information. The notebook was a central way of getting access to information. The staff at the Intestinal Failure Unit had a tradition of writing down notes about care and treatment in the notebook. Furthermore, the patients added anything they felt was relevant to them, for eg, questions and answers. The patients used the notebook as a way of keeping records and reminding themselves and their relatives of their current status. Patients found the notebook very useful in communicating with the staff.
Similar to the notebook, the two blackboards around the bed were used as a way of keeping hold of information. This was especially important in relation to keeping track of upcoming tests and appointments. To have the plan on the blackboard right next to the bed was important for the patients.
Staff were also described as a source of information in the surroundings. The patients had the understanding that the staff always kept them informed and took the time to explain given information. The patients felt that the staff were available for questions any time:
… and when sisters come through, that is another thing I like, when they do the doctors’ round, sisters would write down what is being said. So you do not … . “What did he say, what did he mean?” and then they will come in and say, “Do you got any questions?” we can arrange of the doctors and make them come back and they will answer the questions … .
The notebook, the blackboards, and the staff were all sources of information in the surroundings, and these gave the patients a sense of participation.
Emotional experiences
This major theme describes the feelings emerging from the possibility of participating in their own care and treatment through the surroundings. Subthemes were: independence, reassurance, normality, control, responsibility, and confidence.
Independence
Patients described a feeling of independence due to the possibility of doing daily activities by themselves; this gave them a sense of freedom.
Patients expressed that independence was of great importance and one of the basics in life.
The fact that the patients did not need to rely on friends, staff, or family to do their laundry, make them a cup of tea, bring them food, bring them their medicine etc made them feel independent. The possibility of using the surroundings and thus managing to do things by themselves were of great importance and very desirable to the patients.
As an example, patients described that as a result of their independence, they did not have to wait for the nurses to bring them their medicine. Waiting time and ways of minimizing waiting time were big issues, and patients expressed that it meant a lot to them to be able to make a cup of tea when they wanted one:
It makes you feel independent (that you can make your own coffee). That you are not relying on somebody... as you are all relying on a certain time you know, you have got to wait another hour, it is bad enough waiting for painkillers, but waiting for tea or coffee … and then if they are too busy it might not happen, so you do not get a drink and your only option is to go downstairs for a cup of tea or something. So yeah it makes you quite independent.
Furthermore, independence meant that the patients did not have to ask and disturb the staff.
Reassurance
Patients expressed that using the surroundings, they were able to minimize their anxiousness and promote a feeling of reassurance.
The patients described their risk of becoming anxious, which was related to, for eg, not being able to manage their own medication, not being able to wash their clothes, not knowing about their disease status, and not being able to do daily activities when they returned home.
The fact that the patients had a medicine cabinet next to their bed and that they had the opportunity to manage medication themselves reduced anxiousness. Self-medication made it possible for the patients to keep their own time schedule for the medication because they did not have to wait for a nurse. One patient described it in this way:
You just know that it is there [the medicine]. So, you do not get that anxious feeling when you are waiting to get your tablets from the nurses.
Anxiousness in relation to not being able to do their laundry was connected to the fact that many of the patients at the Intestinal Failure Unit had a stoma. The patients pointed out that they often experienced leaking stoma bags. The access to a launderette made the leaks less embarrassing because they could wash their clothes right away:
It makes me feel happy that I can get it done [the laundry]. Not anxious that it is going to be lying around smelling, you know … . Makes me feel a lot more relaxed.
Anxiousness concerning not knowing about status of one’s own treatment and care was reduced through information and the access to information from the surroundings. Also, information, especially the notebook, gave the patients’ relatives a sense of reassurance and participation. The anxiousness related to not being able to manage daily activities at home was met through the surroundings, where patients had the opportunity to participate in and practice daily activities.
The ability to manage their own medication, wash clothes, to get to know about status of their treatment and care, and to do daily activities gave the patients a sense of reassurance.
Normality
Patients described several things in the surroundings that made it possible for them to participate in their daily activities. These daily activities could, for eg, include going shopping, and making themselves or their family tea or coffee. One patient explained:
Even if you have got visitors coming, especially in Marks and Spencer [store] downstairs, you can get food to eat it in the day room with them, you know, it is just more of normality.
These activities were described as being a part of the patients’ daily routine at home, and the ability to do the same at the unit gave the patients a sense of normality. Furthermore, the patients described that the ability to, for eg, do their laundry gave them something else to focus on during the day.
Control
It gave a sense of control to the patients to, for eg, do their own laundry and keep a record of treatment and care through the notebook and the blackboard. The patients described control to be of great importance:
You could see exactly what you have got to come [tests and appointments], you could plan your days because they try to balance it … . That I knew exactly what I was having when and where, and times and that … and that really … it is just knowing … . It is back to being in control … . You are not really in control, but you have that illusion of being in control, because you know what is happening … .
The fact that the patients were able to use the sluice room and keep track of their input and output could lead to improved control and understanding of the connection between input and output. This is illustrated in the following quotation:
… makes you aware of how much is coming out and going in. It makes you more aware of what you are drinking and what you are eating … . I mean most patients on this ward the more they put in the more they put out … .
Responsibility
The patients described that the surroundings made it possible for them to take responsibility, through the ability to participate.
I’ve come here to get well, so I just do not want to sit around all day … . So participation is taking part in whatever they offer … self-medicating … . Taking responsibility, really, for life, and my treatments and what they are going to do.
Furthermore, the ability to participate in the daily activities were described by the patients as an ability to help the nurses and thereby take responsibility:
I look at it as helping, because … I know that they are short-staffed, in some cases they are, and I just think, “Well, if I am capable, why can I not do it?”
The patients did not have the perception that daily activities, such as fetching a cup of tea, were an important task for the nurses. If they were able to, patients felt it important to do these themselves, so the nurses could focus on more important issues.
Confidence
The patients described an opportunity to feel confident in their own ability to do daily activities. The surroundings made this achievable because of the possibility of participating in daily activities, and in this way, the patients could gain confidence in their own ability:
… and I thought, “Well, I am quite capable of doing this” and it was a test for me, how did I cope making my own bed, and I know now if I go home, I am quite confident I can do that … .”
Patients described “having confidence” as especially important when discharged and afterwards, when having to be able to take care of themselves.
Discussion
This study explored the importance of the surroundings in relation to patient participation, based on patients’ experiences.
The emotional experiences were described separately even though they seem to affect each other – thus, patients described a connection between feeling confident and thereby getting reassurance. However, the investigators chose to describe the emotional experiences separately to clarify the findings.
The findings in this study indicate that the patients’ surroundings are essential to the patients’ ability to participate in their own care and treatment. Hence, it could be possible to improve patient participation by changing the surroundings.
Nurses have noted that shortcomings in the physical environment can be a barrier for patient participation.19 The findings of this study confirmed the importance of the surroundings, from the patients’ point of view, in relation to participation.
Larson et al11 described patients’ perception of barriers to participation in nursing care. One of the categories, named “facing own inability”, illustrates barriers related to patients lack of control of their situation, for eg, when “not knowing enough” and when having “low self-esteem”.11 The lack of knowledge as a barrier to participation has been pointed out in other studies as well.2,28 This study showed that the surroundings can make it easier to seek and get information, which can in turn, reduce the barrier of not knowing enough. The barrier of low self-esteem can be overcome by the possibility of gaining confidence through the surroundings.
The patients in this study emphasized the importance of nurses being encouraging and available for conversation, in relation to participation. This finding is consistent with other findings that point out that nurses’ attitude can have an effect on patient participation.11,19,28
An important question is whether patients with IF experience the surroundings in relation to patient participation differently from other patient groups - this remains unknown. However, the interview guide used in this study was not made specifically for patients with IF and did not include disease-specific questions. Thus, transfer of the results of the present study to other patient groups may be possible. Further investigation, using the interview guide in other patient groups, could be possible because of the specific focus on the surroundings only.
The launderette was of great significance for patients. Since more than half of the interviewed patients had a stoma, this finding may be of particular importance in this patient group and might not be as valued in other patient groups.
Patients with IF experience prolonged hospitalization. Thus, the surroundings may be especially important for these patients. Furthermore, Faulkner and Aveyard described that patients are more willing to participate when the initial stages of illness have passed,29 which indicates that the surroundings may be of greater importance in patients with prolonged hospital admission. The study also describes that when patients are admitted to a hospital, they have the perception that they are not expected to look after themselves.29 The findings of the study implied that the surroundings can present an expectation that patients participate in their own care and treatment.
The findings in this study are limited to the data collected and are based on the participants’ ability to express their experience of the surroundings in relation to patient participation. All the interviews took place at the hospital, although the environment might not have been convenient from the patients’ perspective; this may have affected the answers. Two of the interviews were performed at the patients’ bedside because of immobility; this could also have an impact on the interview.
Data were collected from eight interviews, which might be considered as a small sample size. However, patients were included in interviews until saturation, when no additional or new data were identified. Furthermore, Sandelowski described that if the data material is too large, it may not permit an in-depth analysis.30
Conclusion
Our study contributes to the knowledge and understanding of patients’ experiences of the surroundings in relation to patient participation. The findings showed that patients can be enabled through their surroundings, by the possibility of participating in daily activities, and by seeking and getting information. Having the possibility of participating in daily activities, and of seeking and getting information led to emotional experiences related to: independence, reassurance, normality, control, responsibility, and confidence. The surroundings, in relation to patient participation, should be considered of greater importance when planning and organizing nursing care. Further research is needed to increase the understanding of the importance of patient surroundings in relation to patient participation. This research could include the nurses’ perspective on the topic.
Acknowledgments
We are grateful to the participants who were willing to be interviewed and who openly shared their thoughts and experiences. Furthermore, we would like to thank the Intestinal Failure Unit, H8, Salford Royal NHS Foundation Trust, Manchester, United Kingdom, for letting us stay at their unit.
Disclosure
The authors report no conflicts of interest in this work.
References
Larsson IE, Sahlsten MJ, Sjöström B, Lindencrona CS, Plos KA. Patient participation in nursing care from a patient perspective: a Grounded Theory study. Scand J Caring Sci. 2007;21(3):313–320. | |
Höglund AT, Winblad U, Arnetz B, Arnetz JE. Patient participation during hospitalization for myocardial infarction: perceptions among patients and personnel. Scand J Caring Sci. 2010;24(3):482–489. | |
Cahill J. Patient participation – a review of the literature. J Clin Nurs. 1998;7(2):119-128. | |
Tariman JD, Berry DL, Cochrane B, Doorenbos A, Schepp K. Preferred and actual participation roles during health care decision making in persons with cancer: a systematic review. Ann Oncol. 2010;21(6):1145–1151. | |
Burton D, Blundell N, Jones M, Fraser A, Elwyn G. Shared decision-making in cardiology: do patients want it and do doctors provide it? Patient Educ Couns. 2010;80(2):173–179. | |
Sahlsten MJ, Larsson IE, Sjöström B, Lindencrona CS, Plos KA. Patient participation in nursing care: towards a concept clarification from a nurse perspective. J Clin Nurs. 2007;16(4):630–637. | |
Hesse BW, Nelson DE, Kreps GL, et al. Trust and sources of health information: the impact of the Internet and its implications for health care providers: findings from the first Health Information National Trends Survey. Arch Intern Med. 2005;165(22):2618–2624. | |
Lal S, Teubner A, Shaffer JL. Review article: intestinal failure. Aliment Pharmacol Ther. 2006;24(1):19-31. | |
O’Keefe SJ, Buchman AL, Fishbein TM, Jeejeebhoy KN, Jeppesen PB, Shaffer J. Short bowel syndrome and intestinal failure: consensus definitions and overview. Clin Gastroenterol Hepatol. 2006;4(1):6–10. | |
Sahlsten MJ, Larsson IE, Sjöström B, Plos KA. An analysis of the concept of patient participation. Nurs Forum. 2008;43(1):2-11. | |
Larsson IE, Sahlsten MJ, Segesten K, Plos KA. Patients’ perceptions of barriers for participation in nursing care. Scand J Caring Sci. 2011;25(3):575–582. | |
Williams GC, Freedman ZR, Deci EL. Supporting autonomy to motivate patients with diabetes for glucose control. Diabetes Care. 1998;21(10):1644–1651. | |
Sainio C, Lauri S, Eriksson E. Cancer patients’ views and experiences of participation in care and decision making. Nurs Ethics. 2001;8(2):97-113. | |
Greenfield S, Kaplan SH, Ware JE Jr, Yano EM, Frank HJ. Patients’ participation in medical care: effects on blood sugar control and quality of life in diabetes. J Gen Intern Med. 1988;3(5):448–457. | |
Rachmani R, Levi Z, Slavachevski I, Avin M, Ravid M. Teaching patients to monitor their risk factors retards the progression of vascular complications in high-risk patients with Type 2 diabetes mellitus – a randomized prospective study. Diabet Med. 2002;19(5):385–392. | |
Rost KM, Flavin KS, Cole K, McGill JB. Change in metabolic control and functional status after hospitalization. Impact of patient activation intervention in diabetic patients. Diabetes Care. 1991;14(10):881–889. | |
Arnetz JE, Almin I, Bergström K, Franzén Y, Nilsson H. Active patient involvement in the establishment of physical therapy goals: Effects on treatment outcome and quality of care. European Journal of Physiotherapy. 2004;6(2):50-69. | |
Loh A, Leonhart R, Wills CE, Simon D, Härter M. The impact of patient participation on adherence and clinical outcome in primary care of depression. Patient Educ Couns. 2007;65(1):69–78. | |
Sahlsten MJ, Larsson IE, Plos KA, Lindencrona CS. Hindrance for patient participation in nursing care. Scand J Caring Sci. 2005;19(3):223–229. | |
Sahlsten MJ, Larsson IE, Lindencrona CS, Plos KA. Patient participation in nursing care: an interpretation by Swedish registered nurses. J Clin Nurs. 2005;14(1):35–42. | |
Ryden MB. Environmental support for autonomy in the institutionalized elderly. Res Nurs Health. 1985;8(4):363–371. | |
Giloth BE. Promoting patient involvement: educational, organizational, and environmental strategies. Patient Educ Couns. 1990;15(1):29–38. | |
Lindseth A, Norberg A. A phenomenological hermeneutical method for researching lived experience. Scand J Caring Sci. 2004;18(2):145–153. | |
Kvale S, Brinkmann S. InterViews: Learning the Craft of Qualitative Research Interviewing. 2nd ed. Thousand Oaks, CA: Sage Publications, Inc.; 2009. | |
Sykepleiernes Samarbeid i Norden. [Ethical Guidelines for Nursing Research in the Nordic Countries.] Etiske Retningslinier for Sygeplejeforskning i Norden. Revideret udgave ed. Oslo: Sykepleiernes Samarbeid i Norden; 2003. | |
Crabtree BF, Miller WL. Doing Qualitative Research. 2nd ed. Thousand Oaks, CA: Sage Publications, Inc.; 1999. | |
Malterud K. Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. 2012;40(8):795–805. | |
Eldh AC, Ekman I, Ehnfors M. Conditions for patient participation and non-participation in health care. Nurs Ethics. 2006;13(5):503–514. | |
Faulkner M, Aveyard B. Is the hospital sick role a barrier to patient participation? Nurs Times. 2002;98(24):35–36. | |
Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18(2):179-183. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.