")
Back to Journals » International Journal of Women's Health » Volume 7
Hormone withdrawal-associated symptoms with ethinylestradiol 20 µg/drospirenone 3 mg (24/4 regimen) versus ethinylestradiol 20 µg/desogestrel 150 µg (21/7 regimen)
Authors Bitzer J, Banal-Silao MJ, Ahrendt H, Restrepo J, Hardtke M, Wissinger-Graefenhahn U, Trummer D
Received 22 November 2014
Accepted for publication 9 February 2015
Published 18 May 2015 Volume 2015:7 Pages 501—509
DOI https://doi.org/10.2147/IJWH.S77942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Johannes Bitzer,1 Maria Jesusa Banal-Silao,2 Hans-Joachim Ahrendt,3 Jaime Restrepo,4 Marion Hardtke,5 Ulrike Wissinger-Graefenhahn,6 Dietmar Trummer7
1Department of Obstetrics and Gynecology, University Hospital of Basel, Basel, Switzerland; 2University of the Philippines College of Medicine, Manila, Philippines; 3Praxis für Frauenheilkunde, Klinische Forschung und Weiterbildung (Clinical Research and Further Education), Magdeburg, Germany; 4Centro de Investigación Clínica, Clinica Medellin Poblado, Medellin, Colombia; 5Global Clinical Development Operations, Bayer Pharma AG, Berlin, Germany; 6Global Medical Affairs Women’s Healthcare, Bayer Pharma AG, Berlin, Germany; 7Clinical Statistics Europe, Bayer Pharma AG, Berlin, Germany
Objective: To assess whether the combined oral contraceptive (COC) ethinylestradiol (EE) 20 µg/drospirenone 3 mg taken in a 24/4-day regimen (ie, 4-day hormone-free interval) is more effective than an EE 20 µg/desogestrel (DSG) 150 µg COC taken in a 21/7-day regimen (ie, 7-day hormone-free interval) in reducing hormone withdrawal-associated symptoms (HWAS).
Methods: This double-blind, randomized study (NLM identifier: NCT01076582) was conducted at 34 centers in 12 countries. Otherwise healthy women who experienced ≥2 HWAS of headache, pelvic pain, and/or bloating when using their current COCs in a 21/7-day regimen were recruited. Subjects rated the severity of their HWAS daily on a seven-point Likert scale during a baseline cycle and during four 28-day cycles with EE/drospirenone 24/4 (n=290) or EE/DSG 21/7 (n=304). The primary variable was the mean change from baseline to cycle 4 in the composite HWAS score (sum of scores for all three symptoms) during cycle days 22–28.
Results: In the EE/drospirenone 24/4 group, the mean (standard deviation) composite HWAS score during cycle days 22–28 was reduced from 42.2 (24.8) at baseline to 12.8 (13.4) at cycle 4 (change from baseline: -30.3 [22.9]). In the EE/DSG 21/7 group, the corresponding value was reduced from 41.9 (25.8) to 14.3 (13.2) (change from baseline: -27.7 [24.8]), not significantly different versus EE/drospirenone 24/4. Bleeding pattern, treatment response, rescue medication use, compliance, quality of life, and tolerability were similar between treatments.
Conclusion: Both EE/drospirenone 24/4 and EE/DSG 21/7 reduced the composite HWAS score from baseline to cycle 4 in otherwise healthy women. The differences between treatments were too small to be statistically significant.
Keywords: combined oral contraceptives, ethinylestradiol, drospirenone, desogestrel, hormone withdrawal
Introduction
Many women with ovulatory menstrual cycles experience significant symptomatology during their cycle, which in general have been attributed to fluctuations in endogenous hormone levels.1,2 Akin to this symptomatology, some women using combined oral contraceptives (COCs) with the standard 21/7-day regimen report side effects such as nausea/vomiting, headaches, bloating/swelling, breast tenderness, and/or pelvic pain more commonly during the hormone-free interval (HFI) than during active tablet intake.3 These side effects are generally referred to as “hormone withdrawal-associated symptoms” (HWAS). COCs with a shortened HFI (eg, from 7 days to 5 days, 4 days, or even 2 days) provide markedly greater suppression of ovarian activity and limit the extent of exogenous hormonal fluctuations throughout the cycle, and have been shown to reduce or eliminate these symptoms.3–7 Consequently, shortening or eliminating the HFI is now recognized as a well-tolerated and effective method of reducing the frequency or severity of HWAS.8
The aim of this study was to assess whether the ethinylestradiol (EE) 20 μg/drospirenone 3 mg COC taken in a 24/4-day regimen (ie, 4-day HFI) is more effective than an EE 20 μg/desogestrel (DSG) 150 μg COC taken in a 21/7-day regimen (ie, 7-day HFI) in reducing the frequency and severity of HWAS in otherwise healthy women prone to these symptoms.
Methods
Study design
This two-arm, parallel-group, double-blind, randomized, active-controlled study (NLM identifier: NCT01076582) was conducted at 34 centers in 12 countries (Argentina, Chile, Colombia, Czech Republic, Germany, Italy, Korea, Philippines, Portugal, Switzerland, Thailand, and the United Kingdom). The study was conducted in line with the Declaration of Helsinki and was approved by each site’s Independent Ethics Committee/Institutional Review Board. All participants provided written informed consent.
Study population
Otherwise healthy women aged 18–35 years (smokers aged ≤30 years) with regular menstrual cycles and who were currently using a low-dose EE-containing COC in a 21/7-day regimen (for at least 3 months), but suffering from at least two of the HWAS of headache, pelvic pain and bloating were recruited.
During a baseline cycle with their usual low-dose EE-containing COC taken in a 21/7 regimen, subjects rated their HWAS daily on a seven-point Likert scale, where 0= no pain to 6= worst pain imaginable. The women were asked to rate three symptoms (headache, pelvic pain, or bloating) in their diaries daily, indicating the worst pain level on that day. In order to be eligible for randomization, the 7-day composite score of HWAS (sum of headache + pelvic pain + bloating) during cycle days 22–28 had to be at least 50% higher than the composite score during cycle days 1–21 (ie, the 21-day score divided by 3 [for normalization]). This was deemed sufficient evidence that the symptoms were related to hormone withdrawal.
Exclusion criteria were in accordance with the usual contraindications for COCs.9
Study treatment
Subjects were randomized (1:1) to receive EE 20 μg/drospirenone 3 mg in a 24/4-day regimen, or EE 20 μg/DSG 150 μg in a 21/7-day regimen for four consecutive 28-day cycles in a block randomization scheme (block size 4). An interactive voice response system/interactive Web response system was used to keep track of the randomization blocks. Both COCs were encapsulated to maintain blinding.
Study variables
The primary efficacy variable was the mean change from baseline to cycle 4 in the composite HWAS score for headache, pelvic pain, and bloating during cycle days 22–28; a composite HWAS score was calculated by summing up all three HWAS ratings. Subjects recorded the severity of their HWAS daily in diary cards using a seven-point Likert scale, as described for the baseline cycle.
Secondary efficacy variables assessed during cycle days 22–28 were as follows: mean change from baseline to cycle 2 in the composite HWAS score, as described for the primary variable; mean change from baseline to cycles 2 and 4 in individual HWAS (headache, bloating, pelvic pain, and the composite score for bloating plus pelvic pain); proportion of subjects experiencing individual HWAS (score of ≥1); and mean change from baseline to cycles 2 and 4 in the maximum intensity of individual HWAS.
Regional analyses for Asia/Pacific, Europe, and Latin America were performed for the primary variables, as well as for the baseline characteristics and demography post hoc.
Quality of life was assessed using a short version of the Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q)10 and the Clinical Global Impression (CGI) scale.11 The short Q-LES-Q is a 15-item questionnaire in which the subject rates their satisfaction during the last week. Scores were rated on a 5-point scale, where 1= very poor and 5= very good. Women completed the Q-LES-Q on day 1 after the baseline cycle and day 1 after cycle 4. The CGI was completed by both women and the investigators at the end of the study. The subject’s overall clinical experience was rated on an eight-point scale, where 0= not assessed, 1= very much improved, and 7= very much worse.
The following variables were also assessed: bleeding/spotting days and episodes; cycle control indices; treatment response; rescue medication use; and compliance. Subjects assessed and recorded their bleeding daily in the same diary cards used to document HWAS severity. Any bleeding that occurred on a given day was rated by the subjects as: none; spotting; light; normal; or heavy, as previously described.12 Bleeding/spotting episodes were described using the 90-day reference period as recommended by World Health Organization.13 Withdrawal bleeding and intracyclic bleeding were assessed as cycle control indices. Withdrawal bleeding was defined as the first bleeding episode that starts on days 1 to 7 after progestogen withdrawal, provided that the progestogen-free interval lasts at least 3 days. All other bleeding episodes were considered intracyclic. Treatment response was defined as an improvement from baseline to cycle 4 in the most severe symptom during cycle days 22–28 of at least half the standard deviation (SD) with no increase in rescue medication use. In terms of rescue medication, subjects were permitted to take medication to relieve, but not prevent, HWAS. Rescue medication use was recorded by the subject in the daily diary card. Subjects were asked not to change their rescue medication during the study. To assess compliance to the study drug’s use, all subjects recorded their study drug intake on a daily basis in diary cards along with the return of all used, partially used, or unused pouches/blister cards for drug reconciliation at the final visit. Compliance to study treatment was assessed by the extent of exposure (absolute and relative to planned exposure) and cycle length. Safety variables included adverse event (AE) monitoring, physical and gynecological examinations, and monitoring of vital signs.
Statistical analysis
For simplicity, we reasonably assumed that the sum of the composite scores during cycle days 22–28 was normally distributed. The change in composite score during cycle days 22–28 from baseline to cycle 4 was calculated and compared between the two groups using the unpaired, two-sided t-test. Missing data were not imputed, except in the case of: 1) single missing Likert scale data, where missing entries were replaced by the highest intensity of the bordering days (eg, in the case of “3/missing/4”, “missing” would be replaced by “4”; and 2) single missing bleeding intensity data, which were managed in a similar way to missing Likert scale data.
The sample size was determined as 680 subjects in order to provide 90% power to detect a treatment difference of 6.5 (assuming an SD of 23.5) in the composite scores between treatment groups with a two-sided significance level of 5% (type 1 error), assuming a dropout rate of approximately 20%. The treatment difference was estimated on the basis that the reduction in HWAS was 42% greater with a continuous COC than with a 21/7 COC.14 Taking into account differences in the Likert scale used in the Sulak et al14 publication (0–10 versus 0–6 in our study), the sum of scores was estimated to be approximately 5 for each symptom, yielding a score of 15 for three symptoms. It was assumed that the 24/4 COC would reduce the sum of scores by 3/7 compared with the 21/7 COC; therefore, the anticipated reduction was 15×3/7≈6.5.
Results
Subjects
Overall, 714 women were screened and 594 were randomized into the EE/drospirenone group 24/4 (number [n]=290) and the EE/DSG 21/7 group (n=304) (Figure 1). Demographic characteristics at baseline, including gynecological and menstrual bleeding history, were similar between both groups (Table 1). The number of patients in each regional subgroup is also shown in Table 1.
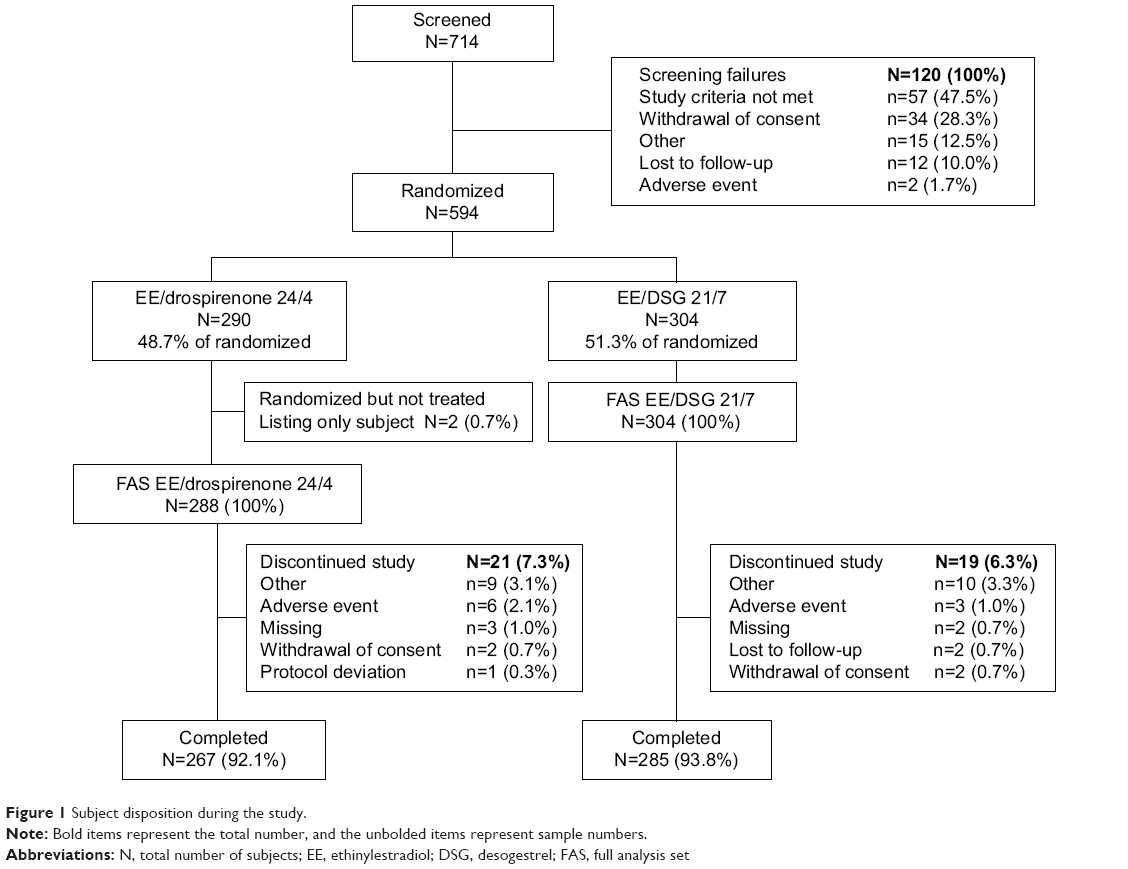 | Figure 1 Subject disposition during the study. |
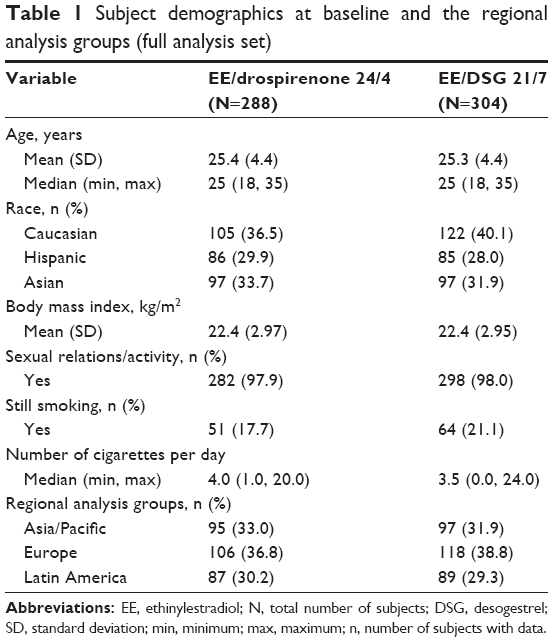 | Table 1 Subject demographics at baseline and the regional analysis groups (full analysis set) |
Primary efficacy variable
The changes in composite symptom scores (comprising pelvic pain, headache, and bloating) during cycle days 22–28 from baseline to cycle 2 or 4 are summarized in Figure 2. For the primary endpoint, the mean (SD) composite HWAS score was reduced from 42.2 (24.8) at baseline to 12.8 (13.4) at cycle 4 in the EE/drospirenone 24/4 group. This corresponded to a mean (SD) change from baseline of −30.3 (22.9; Figure 2). In the EE/DSG 21/7 group, the corresponding composite HWAS scores were reduced from 41.9 (25.8) to 14.3 (13.2), corresponding to a change from baseline of −27.7 (24.8; Figure 2). There was a small difference in the reduction in composite HWAS score in favor of EE/drospirenone 24/4, but this was not significantly greater than that achieved with EE/DSG 21/7 (P=0.2045).
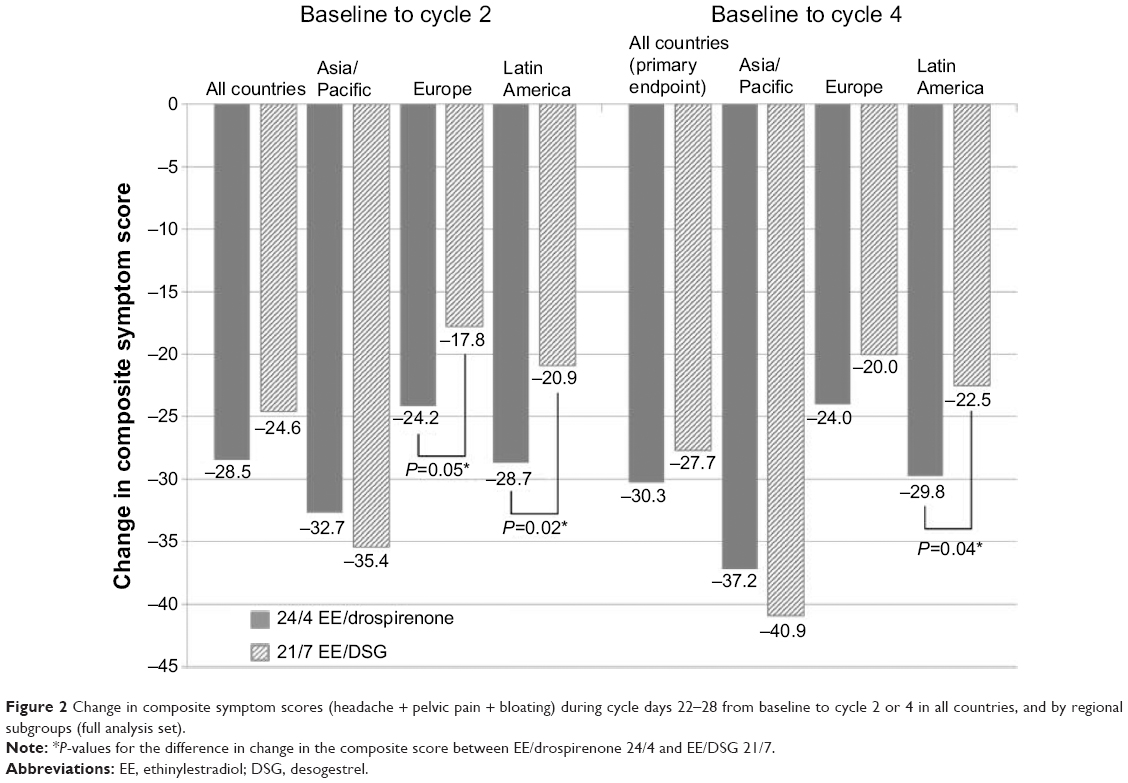 | Figure 2 Change in composite symptom scores (headache + pelvic pain + bloating) during cycle days 22–28 from baseline to cycle 2 or 4 in all countries, and by regional subgroups (full analysis set). |
When the primary endpoint was examined by region, similar results were seen in Europe and Latin America, but not in the Asia/Pacific region where the reduction was greater with EE/DSG 21/7 than with EE/drospirenone 24/4 (Figure 2). In the Latin American subgroup, the reduction in composite HWAS from baseline to cycle 4 was significantly greater with EE/drospirenone 24/4 than with EE/DSG 21/7 (P=0.04; Figure 2).
Secondary efficacy variables
Individual symptom scores
The reduction in individual symptom scores for headache, bloating, pelvic pain, and the composite of bloating plus pelvic pain from baseline to cycles 2 and 4 in the two groups is summarized in Figure 3. Statistical comparisons between treatments were not undertaken. The proportion of women with individual HWAS (headache, bloating, pelvic pain) on days 22–28 (ie, Likert score of ≥1) was reduced from baseline to cycle 4 in both treatment arms (data not shown). Consistent with the individual symptom improvements, there was also a reduction in the maximum intensity of individual symptoms from baseline to cycle 2 and cycle 4 in both treatment groups (Figure 4).
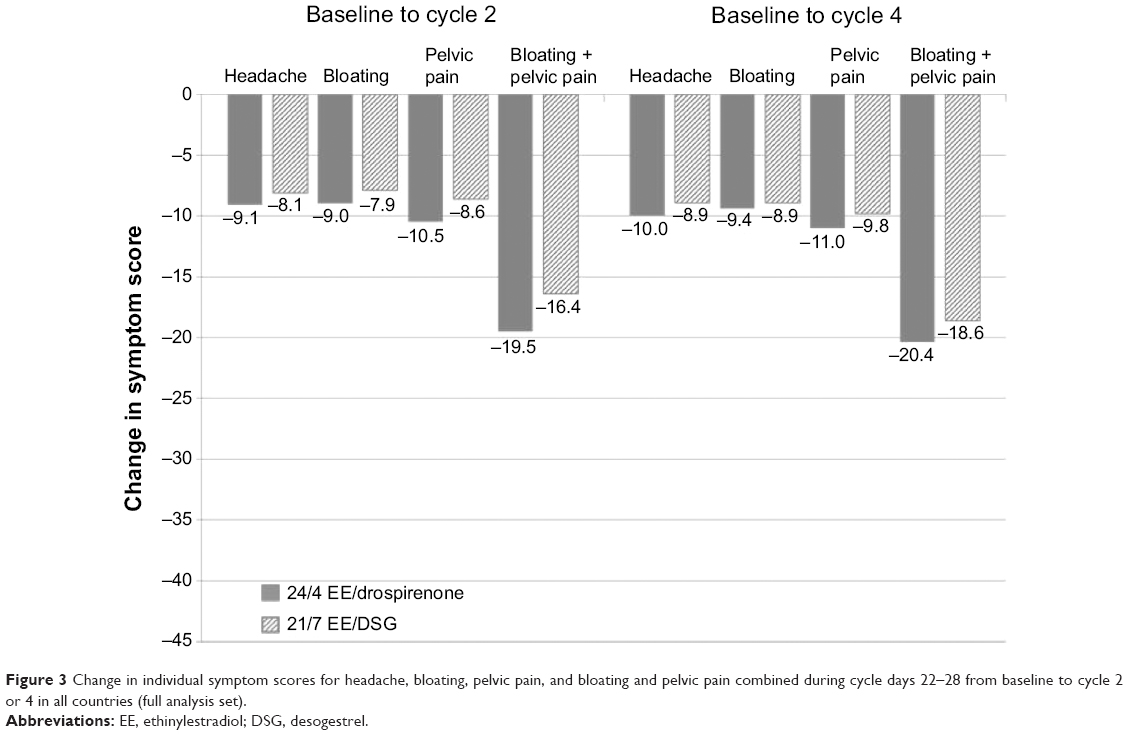 | Figure 3 Change in individual symptom scores for headache, bloating, pelvic pain, and bloating and pelvic pain combined during cycle days 22–28 from baseline to cycle 2 or 4 in all countries (full analysis set). |
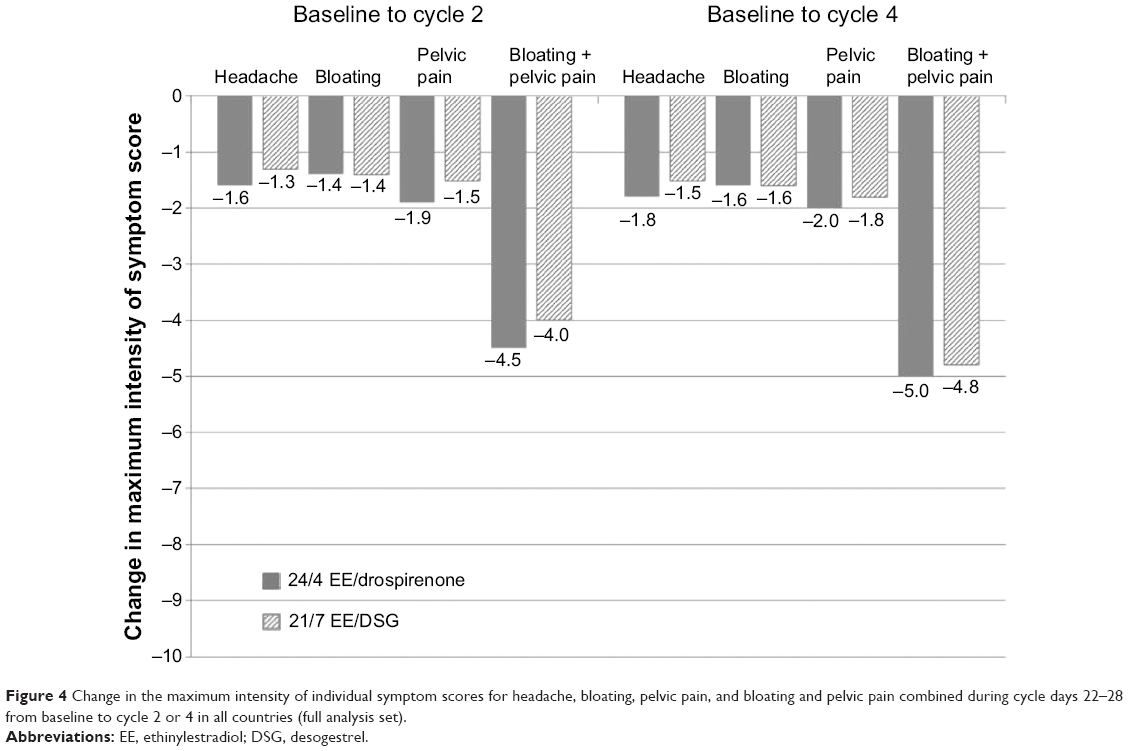 | Figure 4 Change in the maximum intensity of individual symptom scores for headache, bloating, pelvic pain, and bloating and pelvic pain combined during cycle days 22–28 from baseline to cycle 2 or 4 in all countries (full analysis set). |
Bleeding pattern indices
The number of bleeding/spotting days and episodes, as well as the duration of these episodes, was similar between the two groups (Table 2). Bleeding data for cycle 4 were incomplete for many women, as the study ended during their final bleeding episode. For this reason, withdrawal and intracyclic bleeding data were assessed for cycles 1–3 only. The majority of women in both treatment groups experienced withdrawal bleeding (84.4%–92.5% in the EE/drospirenone 24/4 group; 90.6%–96.6% with EE/DSG 21/7). The length of their withdrawal bleeding episodes was 4.7–4.8 days and 5.0–5.4 days, respectively. Bleeding intensity was rated as light or normal in both treatment arms.
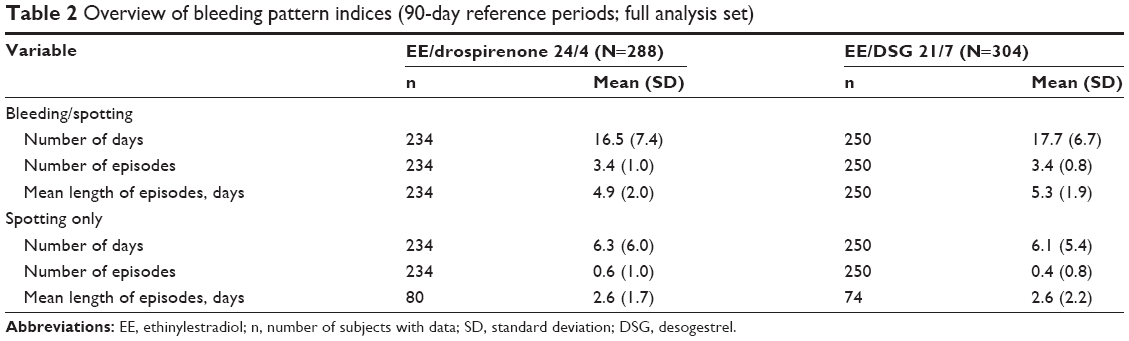 | Table 2 Overview of bleeding pattern indices (90-day reference periods; full analysis set) |
The incidence of intracyclic bleeding was low in both groups (4.3%–10.9% with EE/drospirenone 24/4; 4.0%–8.2% with EE/DSG 21/7). The mean number of intracyclic bleeding days was 0.4–0.5 days and 0.2–0.3 days in the EE/drospirenone 24/4 and EE/DSG 21/7 groups, respectively. The intensity of intracyclic bleeding was rated as “spotting” or “light” in the majority of women.
Treatment response
A total of 76.2% participants in the EE/drospirenone 24/4 group and a comparable proportion of 75.0% in the EE/DSG 21/7 group responded to treatment during cycle days 22–28.
Rescue medication
The pattern of rescue medication consumption was similar between treatment groups throughout the study. At baseline, the proportion of women using rescue medication at any time during the cycle was 37.2% for EE/drospirenone 24/4 and 41.8% for EE/DSG 21/7. There was an immediate reduction in the use of rescue medication in both treatment groups (the proportion of women using rescue medication in cycle 1: EE/drospirenone 24/4, 20.6% [16.6% reduction]; EE/DSG 21/7, 25.9% [15.9% reduction]). This proportion remained low (<32%) throughout the study. Of those women who took rescue medication, most took it for only 1 day during all cycles.
Quality of life
Similar improvements in the mean (SD) score with the Q-LES-Q questionnaire were observed in both treatment groups; EE/drospirenone 24/4 increased from 62.21 (144.94) to 69.76 (13.87) (mean increase [SD]: 7.68 [16.19]); EE/DSG 21/7 increased from 63.55 (14.45) to 72.42 (12.76) (mean increase [SD]: 8.99 [14.72]), and an analogous pattern was observed for all subscores (with the exception of the “Medication” subscore, where no improvement was observed). According to the subjects’ assessments using the CGI questionnaire, a similar proportion of women in each treatment group had “much improved” or “very much improved” symptoms (EE/drospirenone 24/4: 55.6%; EE/DSG 21/7: 53.2%). Similar trends were observed for the investigator assessments.
Compliance
Treatment compliance was high in both treatment arms, with 96.4% compliance in the EE/drospirenone 24/4 group and 98.1% in the EE/DSG 21/7 group.
Tolerability
Treatment-emergent AEs (TEAEs) were reported in 31.3% of women in the EE/drospirenone 24/4 group and 29.9% of women in the EE/DSG 21/7 group. The majority of these women had mild or moderate TEAEs (96.7% on EE/drospirenone 24/4 and 94.5% on EE/DSG 21/7). An overview of AEs and TEAEs is shown in Table 3. Three serious AEs were reported, two of which occurred in the EE/DSG 21/7 treatment group but were considered unrelated to the study drug (pyelonephritis, leading to discontinuation, and tonsillitis). The third serious AE was a spontaneous abortion occurring in one subject receiving EE/drospirenone 24/4, which was considered to be related to the study drug. This was the only pregnancy reported in the study. There were no deaths during the study.
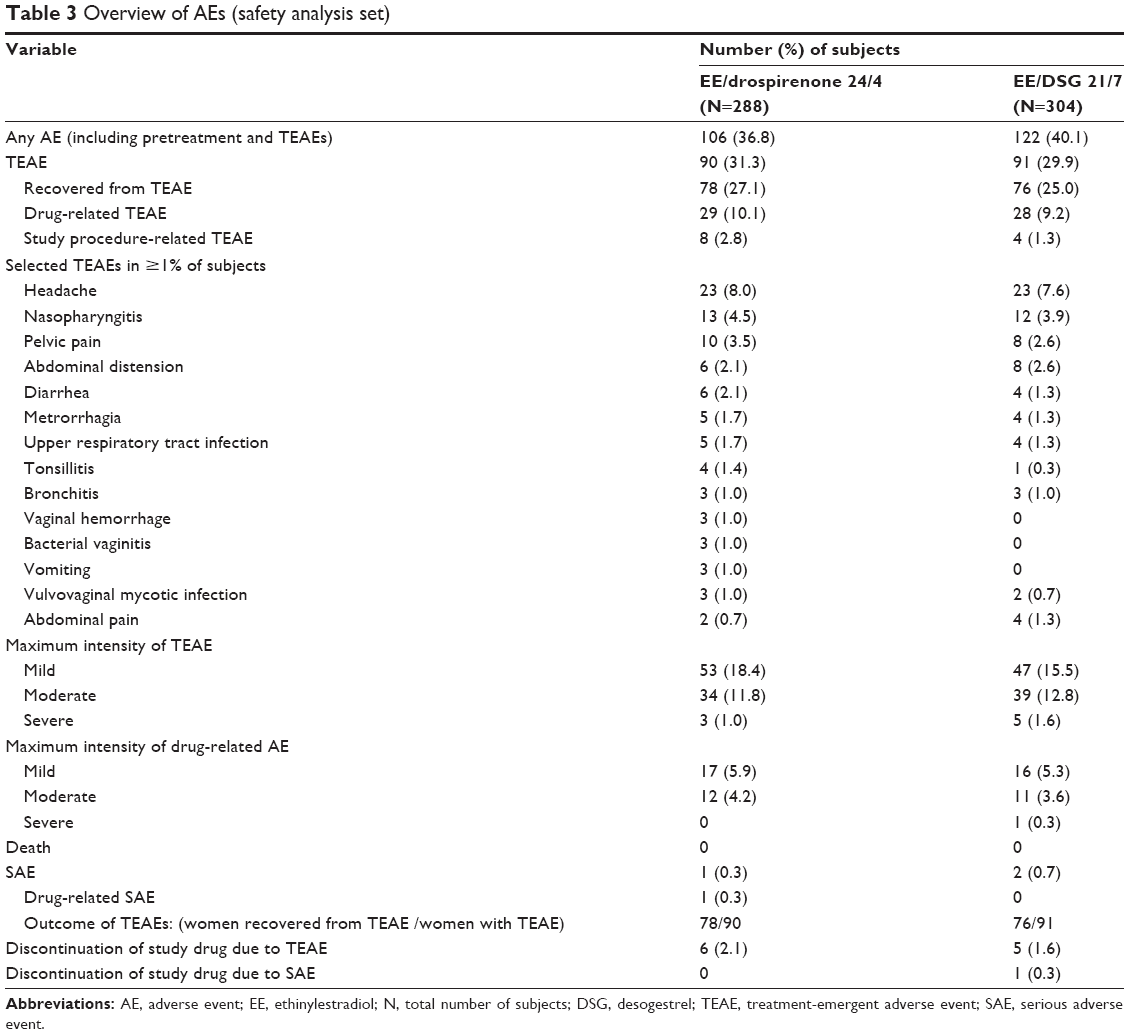 | Table 3 Overview of AEs (safety analysis set) |
Discussion
In this randomized, double-blind, multicenter study, both EE/drospirenone 24/4 and EE/DSG 21/7 reduced the composite HWAS score in otherwise healthy women who experienced these symptoms with their previous COCs. The reductions seen with both treatments were deemed to be clinically relevant; in other (chronic) pain indications, a change of approximately one point on the Likert scale translates into a clinically relevant difference in the subject’s pain perception (which is typically about half a SD).15 This corresponds to a treatment difference of 14 for two symptoms, although it should be noted that the threshold may be smaller in cyclic HWAS.15
In contrast to what we expected, the difference in the composite HWAS score change from baseline to cycle 4 was smaller and hence not statistically significant between the EE/drospirenone 24/4 and EE/DSG 21/7 groups. Previous studies have shown that shortening the HFI reduces HWAS; in a study by Klipping et al5 of women receiving EE 20 μg/drospirenone 3 mg, shortening the HFI from 7 days to 4 days was associated with greater ovarian suppression and a trend toward a reduction in headache and breast tenderness, which were reported as AEs. Furthermore, in two studies of similar design, estradiol valerate/dienogest in a 26/2 regimen was shown to reduce the frequency and intensity of headache and pelvic pain to a significantly greater extent than the comparator 21/7-day COCs (EE/levonorgestrel6 and EE/norgestimate4).
The reason for the absence of a statistical difference between the EE/drospirenone 24/4 and EE/DSG 21/7 groups in our study is partly unclear. One possibility is that the seven-point Likert scale used in our study was not sufficiently sensitive to detect differences in the reduction of HWAS severity between the treatment groups. Our study included a diverse population of women across three continents, and it is likely that the prevailing symptom profile may differ between regions as to the most troublesome HWAS. For the post hoc analysis of the primary endpoint, the results favored EE/drospirenone 24/4 in both Europe and Latin America. In the Asia/Pacific region, however, the opposite effect was seen.
One of the limitations of our analysis was an issue with data collection procedures at one study site in the Asia/Pacific region. During the analysis of the study data, potential inconsistencies were identified, leading to an audit inspection and site visit by the study sponsor. This audit showed an implausible bleeding pattern that was not in line with other sites and regions in the study. This site recruited the most women (>10% of the overall study population) and, therefore, these discrepancies could have had a major impact on the study results. However, the exclusion of data from the problematic site from the Asia/Pacific region data did not alter the statistical conclusion (data not shown). It is possible that European/Latin American women may differ from those in Asia in terms of the types of HWAS experienced and/or the perception of severity. From this experience, the conclusion can be drawn that differences in patient reported outcomes including pain perception, general well-being, etc, are conditioned by a large variety of individual factors that are difficult to control for. Future research should therefore be focusing on a homogeneous sample of women observed by closely collaborating investigators or by a single center.
Conclusion
Both EE/drospirenone in a 24/4-day regimen and EE/DSG in a 21/7-day regimen reduced composite HWAS scores (headache, bloating, and pelvic pain) from baseline to cycle 4 in otherwise healthy women. Contrary to expectations, statistically significant differences between treatments were not observed.
Acknowledgments
This study was funded by Bayer HealthCare AG. Medical writing support was provided by Claire Byrne and Faysal Riaz of inScience Communications, Springer Healthcare, and funded by Bayer Pharma AG. Statistical analysis was supported by Matthias Boerner and Felix Mueller.
Disclosure
Marion Hardtke, Ulrike Wissinger-Graefenhahn, and Dietmar Trummer are employees of Bayer Pharma AG. Johannes Bitzer serves on the advisory boards of Bayer Pharma AG, MSD/Merck, Gedeon Richter, Vifor, and Lilly. Maria Jesusa Banal-Silao, Hans-Joachim Ahrendt, and Jaime Restrepo report no conflicts of interest in this work.
References
Sulak PJ. Continuous oral contraception: changing times. Best Pract Res Clin Obstet Gynaecol. 2008;22(2):355–374. | ||
Clayton AH. Symptoms related to the menstrual cycle: diagnosis, prevalence, and treatment. J Psychiatr Pract. 2008;14(1):13–21. | ||
Sulak PJ, Scow RD, Preece C, Riggs MW, Kuehl TJ. Hormone withdrawal symptoms in oral contraceptive users. Obstet Gynecol. 2000;95(2):261–266. | ||
Jensen JT, Parke S, Mellinger U, Serrani M, Mabey RG Jr. Hormone withdrawal-associated symptoms: comparison of oestradiol valerate/dienogest versus ethinylestradiol/norgestimate. Eur J Contracept Reprod Health Care. 2013;18(4):274–283. | ||
Klipping C, Duijkers I, Trummer D, Marr J. Suppression of ovarian activity with a drospirenone-containing oral contraceptive in a 24/4 regimen. Contraception. 2008;78(1):16–25. | ||
Macìas G, Merki-Feld GS, Parke S, Mellinger U, Serrani M. Effects of a combined oral contraceptive containing oestradiol valerate/dienogest on hormone withdrawal-associated symptoms: results from the multicentre, randomised, double-blind, active-controlled HARMONY II study. J Obstet Gynaecol. 2013;33(6):591–596. | ||
Spona J, Elstein M, Feichtinger W, et al. Shorter pill-free interval in combined oral contraceptives decreases follicular development. Contraception. 1996;54(2):71–77. | ||
Bitzer J. Hormone withdrawal-associated symptoms: overlooked and under-explored. Gynecol Endocrinol. 2013;29(6):530–535. | ||
World Health Organization. Medical eligibility criteria for contraceptive use – 4th ed. 2010. Available from: http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf?ua=1. Accessed 23 February 2015. | ||
Endicott J, Nee J, Harrison W, Blumenthal R. Quality of Life Enjoyment and Satisfaction Questionnaire: a new measure. Psychopharmacol Bull. 1993;29(2):321–326. | ||
Guy W. Clinical Global Impressions. In: National Institute for Mental Health, editors. ECDEU Assessment Manual for Psychopharmacology. Rockville, MD: DHEW Pub; 1976:218–222. | ||
Bachmann G, Sulak PJ, Sampson-Landers C, Benda N, Marr J. Efficacy and safety of a low-dose 24-day combined oral contraceptive containing 20 micrograms ethinylestradiol and 3 mg drospirenone. Contraception. 2004;70(3):191–198. | ||
Belsey EM, Machin D, d’ Arcangues C. The analysis of vaginal bleeding patterns induced by fertility regulating methods. World Health Organization Special Programme of Research, Development and Research Training in Human Reproduction. Contraception. 1986;34:253–260. | ||
Sulak P, Willis S, Kuehl T, Coffee A, Clark J. Headaches and oral contraceptives: impact of eliminating the standard 7-day placebo interval. Headache. 2007;47(1):27–37. | ||
Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care. 2003;41(5):582–592. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.