")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 6
HIV/AIDS health care challenges for cross- country migrants in low- and middle-income countries: a scoping review
Authors Suphanchaimat R , Sommanustweechai A, Khitdee C, Thaichinda C, Kantamaturapoj K, Leelahavarong P, Jumriangrit P, Topothai T, Wisaijohn T, Putthasri W
Received 20 October 2013
Accepted for publication 11 December 2013
Published 26 February 2014 Volume 2014:6 Pages 19—38
DOI https://doi.org/10.2147/HIV.S56277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Rapeepong Suphanchaimat,1,2 Angkana Sommanustweechai,1 Chiraporn Khitdee,1 Chompoonut Thaichinda,1 Kanang Kantamaturapoj,3 Pattara Leelahavarong,4 Pensom Jumriangrit,1 Thitikorn Topothai,1 Thunthita Wisaijohn,1 Weerasak Putthasri1
1International Health Policy Program (IHPP), Ministry of Public Health, Nonthaburi, Thailand; 2Banphai Hospital, Khon Kaen, Thailand; 3Department of Social Sciences, Faculty of Social Sciences and Humanities, Mahidol University, Nakhon Pathom, Thailand; 4Health Intervention and Technology Assessment Program, Ministry of Public Health, Nonthaburi, Thailand
Introduction: HIV/AIDS has been one of the world's most important health challenges in recent history. The global solidarity in responding to HIV/AIDS through the provision of antiretroviral therapy (ART) and encouraging early screening has been proved successful in saving lives of infected populations in past decades. However, there remain several challenges, one of which is how HIV/AIDS policies keep pace with the growing speed and diversity of migration flows. This study therefore aimed to examine the nature and the extent of HIV/AIDS health services, barriers to care, and epidemic burdens among cross-country migrants in low- and middle-income countries.
Methods: A scoping review was undertaken by gathering evidence from electronic databases and gray literature from the websites of relevant international initiatives. The articles were reviewed according to the defined themes: epidemic burdens of HIV/AIDS, barriers to health services and HIV/AIDS risks, and the operational management of the current health systems for HIV/AIDS.
Results: Of the 437 articles selected for an initial screening, 35 were read in full and mapped with the defined research questions. A high HIV/AIDS infection rate was a major concern among cross-country migrants in many regions, in particular sub-Saharan Africa. Despite a large number of studies reported in Africa, fewer studies were found in Asia and Latin America. Barriers of access to HIV/AIDS services comprised inadequate management of guidelines and referral systems, discriminatory attitudes, language differences, unstable legal status, and financial hardship. Though health systems management varied across countries, international partners consistently played a critical role in providing support for HIV/AIDS services to uninsured migrants and refugees.
Conclusion: It was evident that HIV/AIDS health care problems for migrants were a major concern in many developing nations. However, there was little evidence suggesting if the current health systems effectively addressed those problems or if such management would sustainably function if support from global partners was withdrawn. More in-depth studies were recommended to further explore those knowledge gaps.
Keywords: migrant, refugee, low- and middle-income countries, HIV/AIDS, health systems, scoping review
Introduction
HIV/AIDS has been one of the most important global threats for decades. It has jeopardized not only human health but also countries’ economic growth and the well-being of society as a whole.1–3 Consequently, to effectively tackle the disease, a firm collaboration of medical and health systems research at all levels is required.4,5
The United Nations Programme on HIV/AIDS (UNAIDS) reported that approximately 34 million people around the world were living with HIV/AIDS in 2011 and about 1.7 million people died from the disease in that year.6 Its epidemic burdens vary greatly between countries and regions. Sub-Saharan Africa is the most affected region, contributing to 69% of people living with HIV/AIDS worldwide. The prevalence of HIV/AIDS in adults is consistently high in many regions: approximately 4.9% in sub-Saharan Africa, and 1.0% in the countries of the Caribbean, Eastern Europe, and Central Asia. In South, Southeast, and East Asia, there were almost 5 million infected in these three regions combined.6
Though HIV/AIDS has been one of the world’s greatest health challenges, the global solidarity in responding to HIV/AIDS through the provision of antiretroviral therapy (ART) and the promotion of early screening has been proved successful in saving the lives of infected populations in the past few decades.7 Combating HIV/AIDS was also set as one of the eight Millennium Development Goals, with a target of halting and reversing the spread of the disease by 2015.8 However, there remain several challenges, one of which is how to develop HIV/AIDS policies to be able to keep pace with the growing speed, diversity, and disparity of modern migration flows.9 Several pieces of evidence suggest that migrants and mobile populations are vulnerable to HIV/AIDS infection, and traditional approaches are insufficient to address these complex challenges.10–14 Besides, migrant health is a complex topic and closely linked with unequal distribution of socioeconomic resources. Therefore, to respond to this complexity, policy approaches should be multidisciplinary and be collaborative with stakeholders from all relevant sectors.15,16
The growing demand for a reorientation of policies aimed at securing migrants’ health can be illustrated by a number of recent high-profile health-related international activities. For instance, the 2001 UN General Assembly Special Session on HIV/AIDS called for national, regional, and international strategies that facilitated access to HIV/AIDS-prevention programs for migrants and mobile workers by 2005. In 2009, the Program Coordination Board of the UNAIDS governing body held its 24th meeting in Geneva, with a focus on HIV-related needs for people on the move. The board underscored that the improvement of HIV information and services for these people would boost the development, promotion, and implementation of national, regional, and international strategies.17 In addition, the World Health Organization (WHO) has played active roles in addressing migrants’ health in recent years. This is remarkable through relevant World Health Assembly (WHA) resolutions, eg, Workers Health: Global Plan of Action,18 urging member states to work toward full coverage of all workers including migrants, and Health of Migrants, requesting member states for migrant-sensitive health policies and practices whilst asking the WHO to promote migrant health in collaboration with other relevant organizations.19
With respect to the aforementioned reasons, broader efforts are necessary to understand the interplay between the current HIV/AIDS health service policies and the HIV/AIDS problems affecting migrants’ health. Hitherto, there exist a great number of international publications describing policies in respect of the current HIV/AIDS health services for migrants, such as Mladovsky et al,20 Rechel et al,21 and Gray and van Ginneken,22 and the special report on implementing the Dublin Declaration on partnerships to fight HIV/AIDS in Europe and Central Asia launched by the European Center for Disease Prevention and Control in 2010.23 However, most publications focused on the situation in developed nations. Conversely, pieces of evidence describing the situation in developing countries were hardly found. This is in contrast to the demand for research reported by the International Organization for Migration (IOM) in 2009, which pointed out that the number of migrants flowing between developing countries was not far different from the number of migrants flowing to developed countries.24 The evidence was also supported by the report of the secretary-general of the UN General Assembly in 2006, detailing that approximately a third of the 191 million migrants in the world had flowed from one developing country to another, and another third had moved from a developing country to a developed country. That is to say, “south-to-south” migrants were about as numerous as “south-to-north” migrants.25
This study therefore sought to counter the dearth of evidence by examining the actual practices and challenges of HIV/AIDS health care provision among migrants in low- and middle-income countries (LMICs). The study was executed through a scoping review, focusing on evidence from published literature and from websites of relevant international partners, ie, the WHO, World Bank, and IOM. The authors used a scoping review approach as it is more feasible in finding evidence under broad objectives than traditional systematic reviews that better match with a narrower focus or more specific research questions.26 It was hoped that the study would lead to clearer insights on how HIV/AIDS policies were implemented and operated in response to HIV/AIDS epidemics and health care barriers for migrant populations in developing countries. The byproducts of the review would help to identify the remaining challenges and to suggest ways toward positive policy coherence, as well as future study areas where current evidence is still sparse.20,27
Materials and methods
A roundtable discussion involving all researchers was convened to develop the conceptual framework and identify the review’s subjects. The conceptual framework was adapted and simplified from the “six-building-block” approach of health systems and the Conceptual Framework for Action on the Social Determinants of Health proposed by the WHO.28,29 Nonetheless, only service delivery, human resources, and health financing were key concerns for this review, as they better reflected the broad operational management of the system, whereas other building blocks like medical products and information systems were more technically oriented and should be explored separately. The social determinants of health (SDHs) framework was used to characterize factors regarding hindrances to HIV/AIDS care through a gradient approach, ranging from individual level to community, national, and international level in that order.
Key research questions were identified: 1) What are the epidemic burdens of HIV/AIDS in cross-country migrants living in LMICs?; 2) What are the obstacles hampering the access to health services and what are the related HIV/AIDS risks in the migrant population?; and 3) What is the operational management of existing health systems for addressing HIV/AIDS problems in the migrant population? To address the third research question thoroughly, the following domains were set: service provision and benefit packages, types and roles of the implementing agencies/institutes, human resources for health in managing such services, and health-financing management (Figure 1).
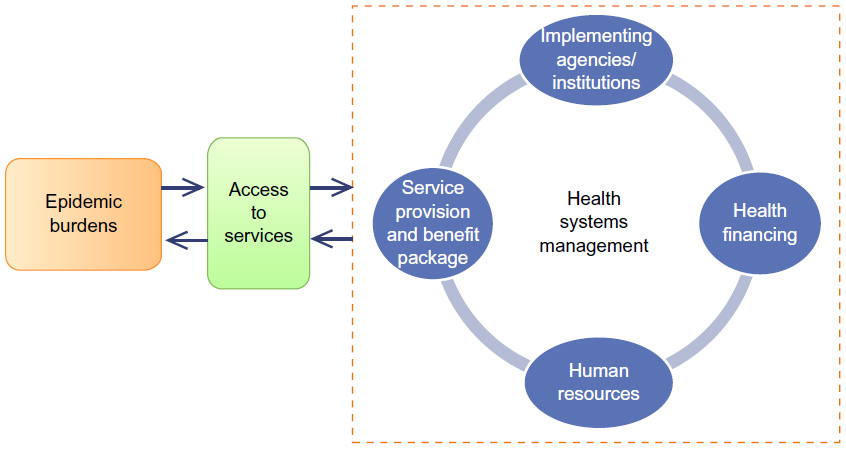 | Figure 1 Conceptual framework of the review on HIV/AIDS-related problems and services in low- and middle-income countries. |
Search strategy
The study explored the literature using two main approaches: systematic search and purposive search. In the systematic search, two key online databases (ie, Medline and ScienceDirect) were identified. The search terms used in the Medline database were constructed as follows: ((“HIV Infections”[Mesh] AND (hasabstract[text])) AND ((“Transients and Migrants”[Mesh] AND (hasabstract[text]) AND Humans[Mesh])) OR (“Refugees”[Mesh] AND (hasabstract[text] AND Humans[Mesh]))). The publication date was limited to between January 1, 2002 and December 31, 2012, and confined to only human studies. For the ScienceDirect database, search terms and date specifications were employed in the same fashion. However, the specific topic areas, ie, social science and medicine, public health, evaluation and program planning, were imposed to narrow the diversity of retrieved articles. In the purposive search, relevant reports and policy briefs were retrieved from the websites of three global development agencies, ie, the WHO, the International Finance Corporation: the World Bank Group, and the IOM. Due to limited capacity in language translation, studies published in languages other than English were excluded.
Inclusion and exclusion criteria
Inclusion and exclusion criteria were defined to ensure the relevance of retrieved articles. Eligible studies were included when they met the following criteria: 1) providing piece(s) of evidence within or about LMICs when they served as destination sites of migration (the identification of LMICs was checked against the World Bank list of country economies in July 2012)30; 2) presenting evidence relevant to the situations and magnitudes of HIV/AIDS-related problems as well as evidence about barriers to health services and/or HIV/AIDS risks in the target population. In this case, the target population was defined as cross-country or cross-national transients and migrants, refugees, and returnees to their countries of origin; and 3) demonstrating the actual practices of existing HIV/AIDS health service systems for the target population.
Concerning the exclusion criteria, studies were kept out of the review if they focused on either 1) a high-income country, 2) domestic migration, or 3) diagnostic tests, clinical trials, and basic science research, all of which were considered irrelevant to the review’s objectives.
Study selection, data extraction, and synthesis
Two authors (RS and PL) independently reviewed titles and abstracts of all the articles retrieved from the databases based on the inclusion and exclusion criteria. Disagreements between the two reviewers were resolved by discussion and consensus with a third party (WP). Potential articles were selected for full-text review and were screened for duplication. EndNote software version X4 (Thomson Reuters, Carlsbad, CA, USA) was used to store and track the search results in a computerized and retrievable format. Selected articles were read and assessed in full in the roundtable discussions among authors. Key information of the selected articles was extracted and entered into the data-extraction form, which was designed in correspondence with the research questions.
Results
Literature search and included studies
A total of 419 citations were selected from Medline and ScienceDirect, and 18 reports (six from the WHO, three from the World Bank, and nine from the IOM). Of these 437 articles, two were excluded on the basis of duplication, leaving a total of 435 articles for further screening. After the initial screen by two independent reviewers (RS and PL), 56 articles were considered relevant. Cohen’s kappa coefficient of interrater reliability was 0.51, suggesting moderate agreement. At this stage, 35 articles were read in full and assessed by all researchers. Their findings were mapped with the research questions and entered into the data-extraction form. The overall article-screening process is presented in Figure 2, and Table 1 displays the overall key information extracted from the selected articles.
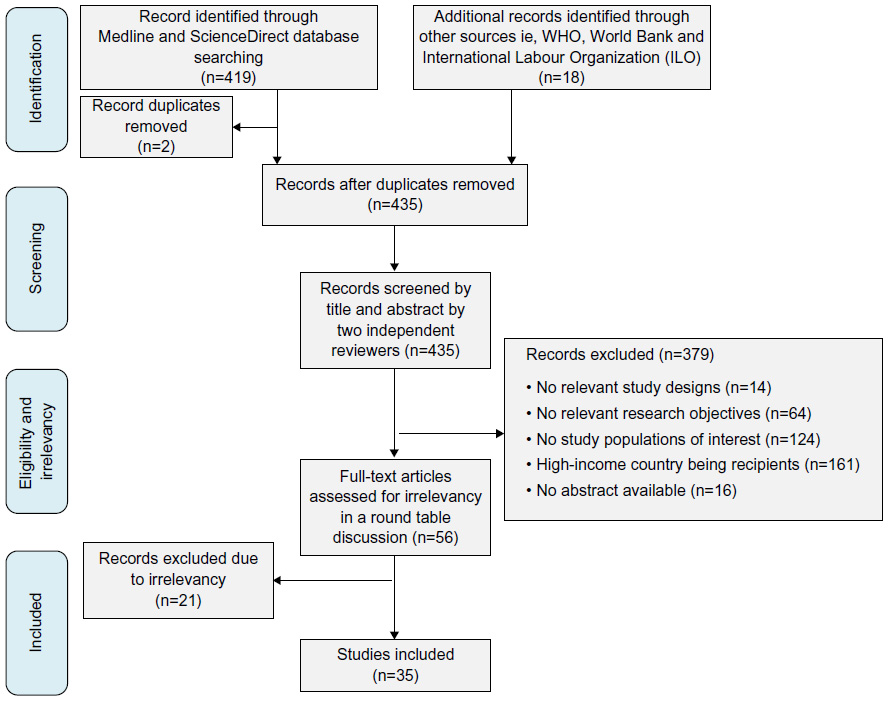 | Figure 2 Article-selection process of the review on HIV/AIDS-related problems and services in low- and middle-income countries. |
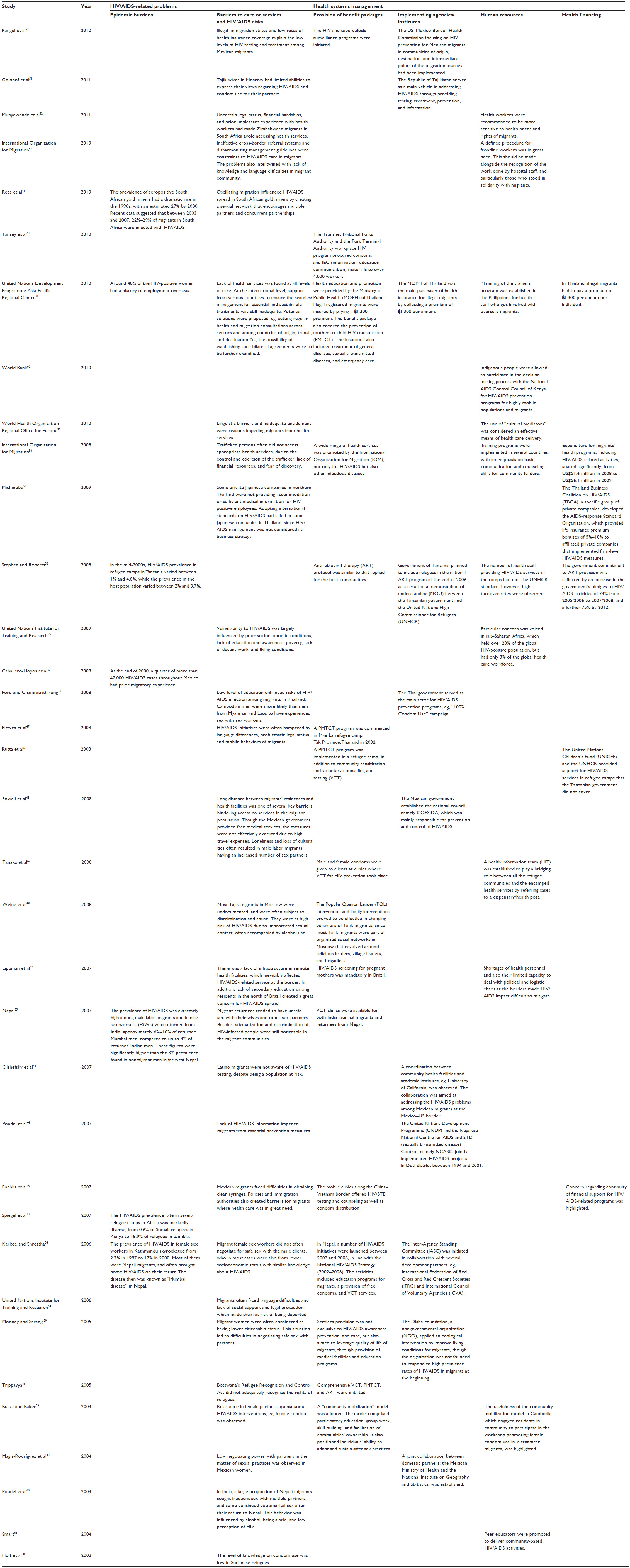 | Table 1 Data-extraction table |
Epidemic burdens
Of the 35 articles reviewed, about a third provided evidence about HIV/AIDS prevalence in the general population without specific data for the migrant and transient population. However, only seven articles from the review presented information on HIV/AIDS epidemics centering on migrants.
Rees et al reported a broad range of HIV/AIDS prevalence of migrants in South Africa, where 22%–29% of migrants were infected with HIV/AIDS between 2003 and 2007.31 In other African countries, ie, Kenya, Uganda, Rwanda, Sudan, Tanzania, and Zambia, a variety of HIV/AIDS rates were observed, ranging from 0.6% to 5% in refugees residing in different camp sites during 2001–2005.32,33
Karkee and Shrestha34 and Nepal35 reported a high prevalence of HIV/AIDS in labor migrants in Nepal, far above the prevalence in the nonmigrant population. In the early 2000s, the prevalence of HIV/AIDS was more pronounced in female sex workers returning from India, accounting for 44%–73% of the returnees, significantly higher than the 4%–10% prevalence in male labor migrants.35 This observation was also consistent with the findings in Sri Lanka by the United Nations Development Programme, where 40% of HIV/AIDS-positive women had a history of overseas employment.36 Only one article from Latin America, reported by Caballero-Hoyos et al in 2008, suggested that at the end of 2000, a quarter of more than 47,000 HIV/AIDS cases throughout Mexico had prior migratory experience.37
Barriers to HIV/AIDS services and risks of HIV/AIDS infection
There were 27 articles mentioning factors impeding HIV/AIDS health services and risks of HIV/AIDS infection in cross-national migrants.31,34–36,38–60 Some articles specifically reported the situation of migrants in certain regions, ie, Asia,34,35,44–47,51,59,60 America (particularly among Mexican migrants),40,42,43,45,48,53 and Africa.31,38,41,49,52 From the review, the barriers to HIV/AIDS services could be classified into two main features: the inadequacy of health service availability, and inaccessibility to care, with special features associating with occupation types and legal status.
The lack of health services was found at all levels of care. At an international level, supports from and within various countries to ensure smooth management for essential and sustainable treatments were still inadequate. This issue was flagged in the regional dialogue on the health challenges for Asian labor migrants in 2010.36 Potential solutions were proposed, eg, establishing regular health and migration consultations across sectors and among countries of origin, transit, and destination. Yet, the possibility of implementing such bilateral agreements were to be further examined.36 At a national level, resources were inequitably distributed and provision for migrants was comparatively scarce compared to those for the general population.42,56 Trippayya also reported that national law was one of the key factors causing discriminatory attitudes toward migrants.41 At a community level, long distances between migrants’ households and health facilities hampered access to health care. This situation was worsened by feeble infrastructure, inadequate management guidelines, and poor referral mechanisms.42,57 In Nepal, a change in lifestyle and community norms influenced Nepali migrants in India to be more engaged in premarital and extramarital conjugations and alcohol consumption, raising their risk of HIV/AIDS infection.60 At an individual organization level, Michinobu revealed that some companies did not provide sufficient medical information for migrant employees, nor did they follow the International Labour Organization code of practice aimed at guaranteeing a decent workplace and proper health care for workers regardless of their HIV/AIDS status.50 Some Japanese companies in Thailand also failed to adopt international standards on HIV/AIDS, as HIV/AIDS management was not considered a business strategy. Furthermore, imposing the notion of human rights on the promotion of HIV prevention among workers was problematic in Thai society, since workers justified themselves as being identified as a powerless and vulnerable group.50
From the perspective of health care inaccessibility and risks of HIV/AIDS infection, the risks included a lack of knowledge and information,34,38,46,48,51,53 discriminatory attitudes toward HIV/AIDS,39,40,43,46,48,55,58 language differences,43,47,54,57–59 and financial hardship.48,49,52 In practice, these factors led to difficulty in accessing such medical products as condoms and clean syringes, as well as other supporting services.44,45,53,58
It is noteworthy that migrants’ types of work significantly interplayed with HIV/AIDS risks. Oscillating migrants working in gold mines in South Africa usually had “informal” family near their place of work alongside their previous family in the country of origin. Oscillating migration influenced HIV/AIDS spread in South African gold miners by creating a sexual network that encouraged multiple partners and concurrent partnerships. This network inevitably resulted in a burgeoning HIV/AIDS epidemic across the entire region.31 The Cambodian seafarers in Thailand reported sex-worker visits more frequently than other men. The reasons behind this included loneliness and time out at sea, a lump payment for work on fishing boats when they arrived at the harbor, and strong pressure from other colleagues working on the boats.46 Loneliness, fewer women, and loss of cultural ties often resulted in male labor migrants having an increased number of sex partners, having sex with male partners, and participating in increased drug use.35,48,61 Even for high-level workers like Japanese and Thai managers working in structured Japanese organizations in Thailand, the HIV/AIDS issue was not adequately considered. As a consequence, measures in the companies were limited only to provision of HIV/AIDS information.
The barriers to care also interweaved with the legal status of migrants, especially those entering the countries illegally.51 For example, male Tajik workers in Russia were legally marginalized at the bottom of the socioeconomic hierarchy. This finding was consistent to what happened in other regions, such as the Mexico–US or India–Nepal borders.42,44,53 Moreover, unsecured legal status made female migrants working in restaurants have no option to complain against sexual exploitation experiences.34 Legal status even affected attitudes of health care providers and hampered the provision of HIV/AIDS programs for migrants living along the Thailand–Myanmar border.47 Likewise, Munyewende et al raised the case of health care staff in South Africa who often denied migrant health services due to mistaken beliefs that the law disallowed services for migrants.52
Health-system management
Service provision and benefit packages
The provision of benefit packages and HIV/AIDS-related services for cross-country migrants was reported in 16 articles.32,34–36,39,41,42,45,47,49,53,56,59,62–64 Of these 16 articles, 14 provided information about general services, including both treatment programs and HIV/AIDS prevention and promotion of interventions. These comprised subactivities as follows: prevention of mother-to-child transmission (PMTCT),36,47,63 ART,41 health education and public campaigns,32,34,39,42,53,59,62,64 condom distribution,45,64 supplementary breastfeeding,63 mobile clinics for HIV/AIDS screening,45 voluntary counseling and testing,35,41,63 and mandatory HIV testing for pregnant women.42 Busza and Baker39 and Mooney and Sarangi59 also urged for the strengthening of communities’ capacity to cope with HIV/AIDS problems. Other articles, eg, Weine et al,49 raised awareness of gender empowerment and challenges in addressing disparities in economic status, language, and cultural positioning in order to maximize the effectiveness of HIV/AIDS intervention programs.56
It is worth mentioning that regional dialogue among policy makers on the health challenges for Asian labor migrants in 2010 suggested the development of guidelines and minimum standards to assist countries of origin and destination for migrant workers, including mandatory health insurance. This initiative was aimed at benefiting migrants as well as their families, regardless if they were joining migrant workers or staying behind.36 Multicountry partnerships should be established to ensure uninterrupted management of conditions requiring long-term treatment, such as HIV/AIDS and tuberculosis. However, the article did not address explicitly how those activities could be executed effectively in actual practice.36
Implementing agencies/institutions
Eleven articles published information about the implementing agencies of HIV/AIDS health care services,32,34,36,40,43,44,46,48,51,53,59 These articles could be further divided into two categories: a single main agency, and jointly collaborative agencies.
Ford and Chamratrithirong highlighted the role of the Thai government in explicitly acting as the most powerful vehicle in setting comprehensive HIV/AIDS programs in the country. One of the key programs was the campaign for 100% condom use by commercial sex workers.46 The Ministry of Public Health (MOPH) of Thailand also instigated health insurance covering PMTCT and a wide range of benefit packages for illegal migrants.36 Sowell et al flagged the leadership of the State Council for Prevention and Control of HIV/AIDS in HIV/AIDS care throughout Mexico.48 Public health leaders in the Republic of Tajikistan integrated gender issues into HIV/AIDS programs by encouraging wives of migrants to play active roles in HIV-prevention initiatives.51 Mooney and Sarangi59 described the case of the Disha Foundation, which applied an ecological intervention to improve living conditions for migrants. However, the organization was not initially tasked with responding to HIV/AIDS problems.
The joint implementing agencies were divided into three subcategories based on the characteristics of collaborations. Magis-Rodríguez et al40 and Olshefsky et al43 reported the first type – domestic agency collaboration – by noting the works done by a number of domestic authorities charged by Mexican government policy with dealing with HIV/AIDS. The second type were multinational collaborations between countries whose borders are connected, eg, Mexico and the US.53 The third type was international development partners who worked with host governments.32,44 It is notable that the stepping in of international development partners could create a profound working network. For instance, the Inter-Agency Standing Committee was initiated in collaboration with several development partners, including the International Federation of Red Cross and Red Crescent Societies and International Council of Voluntary Agencies, which worked together to respond to the dramatic rise in HIV-transmission rates in Kathmandu, Nepal.34
Human resources for health
The issue of labor forces for HIV/AIDS services in migrant populations were discussed in twelve articles32,36,39,42,52,55–58,62,65,66 and grouped according to two main points: shortages in health personnel, and personnel-training systems, as well as capacity-building activities.
Concerns about the shortages of health personnel were found in the three reviewed articles.32,42,55 Lippman et al also detailed the problem of high staff turnover rates, which was aggravated by the drug trade and the weak governmental and community response at the borders of Brazil.42
With regard to personnel training, there were a couple of articles that noted the challenges in training health workforces in general.36,56 Some articles gave specific detail about special training modules, eg, the International Finance Corporation developed training plans for identifying staff who were assigned to be peer educators in mining communities in Southern Africa.65 Several articles also mentioned the strengthening of staff in a wide range of skills, eg, data gathering, research skills, and service delivery, by using cultural mediators and adapting protocols for everyday practices.52,56–58,66 Tanaka et al underscored the use of a health information team consisting of staff with professional backgrounds for delivering HIV/AIDS campaigns to the population of the Nyarugusu refugee camp in Tanzania.62 Busza and Baker underscored the usefulness of a community-mobilization model in Cambodia, which engaged residents in the community to participate in a workshop promoting female condom use in Vietnamese migrants.39
Health financing
Six articles reported the management of financial resources to cope with HIV/AIDS problems in the migrant population.32,36,45,50,56,63 Rutta et al emphasized the important roles of international development partners, ie, the United Nations Children’s Fund and the United Nations High Commissioner for Refugees, in providing support for HIV/AIDS services in refugee camps since the support by Tanzanian government did not cover this population subgroup.63 Rachlis et al raised the importance of continuity of finances for HIV/AIDS-related programs.45 The summary report of the IOM in 2009 pointed out the increase of global expenditure on migrants’ health, from US$51.6 million in 2008 to US$56.1 million in 2009, four times higher than the total 5 years before.56 However, it should be noted that this expenditure comprised all operational expenses of programs targeting migrant health and was not confined only to HIV/AIDS care.
In Thailand, the MOPH provided health security for illegal migrants by collecting an annual  ,300 premium per individual and allocating this revenue to public hospitals affiliated to the Office of Permanent Secretary under the MOPH. Part of the revenue was pooled at the central authority to cover other high-cost treatments, including PMTCT.36
,300 premium per individual and allocating this revenue to public hospitals affiliated to the Office of Permanent Secretary under the MOPH. Part of the revenue was pooled at the central authority to cover other high-cost treatments, including PMTCT.36
The Tanzanian government pledged to leverage ART coverage to 75% by 2012. Funding was secured via commitments through bilateral contributions and global health initiatives to refugees. These commitments were agreed to as funders foresaw a marginal increase in the cost of ART for refugees due to a small number of refugees.32 The private sector also played critical roles in mobilizing funds for HIV/AIDS responses. This was evident in Thailand, where the Thailand Business Coalition on HIV/AIDS, a group of private companies, developed the AIDS Response Standard Organization, providing life insurance premium bonuses of 5%–10% to affiliated private companies that implemented firm-level HIV/AIDS policies and measures, such as corporate social responsibility for HIV/AIDS.50 The initiative was established with an objective to address the societal concerns of the HIV/AIDS epidemic alongside concerns regarding the sexual behavior of young migrant women working in both the commercial and industrial sectors.
Discussion
This review demonstrated interesting findings and comprehensive views about the operational management of current HIV/AIDS health services. However, it is worth mentioning that the results from the review were affected by certain limitations, which will be separately discussed.
Despite the fact that rich information about HIV/AIDS prevalence emerged from the review, few publications explored the actual operational management of existing health systems, with unclear views on the quality, effectiveness, efficiency, and responsiveness of their performance. Some initiatives were proposed, such as developing guidelines and minimum standards for protecting health and financial status of migrants in either origin or destination countries, establishing information-sharing mechanisms across governments for securing health of migrants. These however were still in the process of exploring implementation possibilities.36 Moreover, the roles of receiving and sending countries were not adequately identified, and thus there is a great need for studies examining this matter.
The availability of HIV/AIDS prevalence data in cross-country migrants gave the general impression that such data are quite plentiful in Africa, while not so much information was found about the situation in Latin America and South Asia. This is not surprising, as sub-Saharan Africa contains the greatest HIV/AIDS burden across the globe, and served as a primary region for data gathering. As indicated by the World Bank report in 2006, about two-thirds of the world’s HIV infections were concentrated in sub-Saharan Africa, whose population accounted for 10% of the world’s residents.67 However, the limited number of studies in Latin America and Asia indicated demands for further research on HIV/AIDS services for migrant populations, since the numbers of international migrants and refugees were on the rise in these areas.68,69
Factors hampering HIV/AIDS services were presented in almost half the literature retrieved. The findings were consistent with observations in other publications that explained barriers to HIV/AIDS services for non-migrant populations.70–72 Most of the evidence found common barriers of access to HIV/AIDS services and that these problems were complex, but even more so if they involved migrant populations, since issues of legal status, funding, and stigmatization often played out more significantly.52,65,73 It seems to be a commonly held view that the general health care systems of nations around the world are not adequately dealing with migrants’ SDHs. More primary qualitative works are suggested to obtain better understanding of how diverse religious beliefs and cultural norms are involved in HIV/AIDS risks. For instance, Golobof et al51 underlined the impact of “male-dominated” society on Tajik migrants’ wives, as women had limited ability to voice their concerns on sexual activity with their partners, despite having some awareness of HIV/AIDS.
Most of the publications/reports emphasized the benefits of “hardware” provision, especially condom distribution and the supply of ART, whereas few articles deeply explored or clearly recommended how health care staff and managers might address stigmatization, community attitudes, and legal problems in routine health care service.74 This raises a concern whether such initiatives were adequately and effectively implemented for tackling HIV/AIDS problems in migrants. 28,75 Additionally, only a limited number of publications flagged the issues of language impediments and cultural positioning, both of which may seriously stand in the way of the effectiveness of HIV/AIDS programs.39,49,56,59
As in the case of health care provision for the general population, the success of migrant health care provision is contingent upon the development and training of health care personnel. Without competent health care staff, good services cannot be delivered.76,77 The reviewed publications did not suggest clearly how to manage and train personnel for HIV/AIDS programs in actual situations. Outside HIV/AIDS programs, successful human resources training programs often include “task-shifting”78–80 and “interdisciplinary collaboration.”81,82 Some clues of working with local personnel as cultural mediators and promoting public participation were noticed in a few publications.39,40,58 The lack of data on personnel development/training might derive from a limitation in the search strategy, or it possibly shows up the lack of this issue being addressed by researchers and practitioners dealing with migrant health care at present.
This study also revealed several types of collaborations between different agencies, both domestic and international, in managing HIV/AIDS services for migrants.63 It is clear that there was a growing role for international agencies in filling health care gaps where the government was not willing or able to cover these, as in the case of Tanzania reported by Stephen and Roberts, where bilateral collaborations and global health initiatives supported ART for refugees.32 However, none of the reviewed articles deeply scrutinized the pros and cons of each type of collaboration between the agencies, nor did they deeply outline their challenges and barriers. Furthermore, the monitoring and evaluation systems on such collaborations were not clearly addressed. It is possible that positive signs of HIV/AIDS support from the international partnerships did not derive from the effectiveness of their program management but were due to the small number of refugees they cared for.32 The sustainability of such programs therefore was equivocal.
Another concrete example is what happened in Thailand. Though the government committed to support PMTCT for migrants,36 the population coverage encompassed only registered migrants, while those who were unregistered were left behind. A recent study by Martin in 2007 suggested over 1.3 million migrants in Thailand were unregistered, about triple the number of registered migrants in that year.83 As a result, the responsibility of taking care of this hard-to-reach population who were often engaged with other populations at risk, eg, men who have sex with men and people who inject drugs, were mostly shouldered by nongovernmental organizations (NGOs) in the country.84 Those NGOs thereby mobilized resources from Global Fund (GF) to support their activities for non-Thai key affected populations and migrants. As per the 23rd GF Board meeting in May 2011, a new eligibility, counterpart financing, and prioritization policy was adopted for all funding channels, by taking into account the country’s income level, disease burden, and recent funding history. Although the HIV/AIDS burden in Thailand was high, with its history of recent funding, Thailand is not eligible to ask for support from the GF funding pool. Hitherto, there was no explicit roadmap of how the country will prepare itself given the GF policy has changed.85
This article supported and provided further insights of the findings from the previous systematic review conducted by Weine and Kashuba,61 which identified the determinants of health associated with HIV risks among labor migrants. They mentioned various important HIV/AIDS risks, eg, little social support, family separation, sexual misbehaviors, and low levels of HIV/AIDS knowledge.61 This study further suggested that those factors were not serving as risks alone, but also encumbering the access to HIV/AIDS services, which inevitably created a vicious cycle of the HIV/AIDS situation in migrants. Interestingly, mental health was not explicitly mentioned in this article as a factor impeding access to HIV/AIDS health care services, in contrast to what other studies, such as Weine et al,86 Huang et al,87 and Wong et al,88 have suggested. Though few of the literature describe the issue of mental health in relating to HIV/AIDS, mental health problems among migrant population might be embedded in discriminatory attitudes and stigmatizations, which were reported in many articles under the review.39,40,43,46,48,55,58
Unless a comprehensive policy taking into account all these determinants is to be implemented, HIV/AIDS burdens will continuously be growing in many regions. This review found a variety of efforts aimed at tackling SDHs problems of migrants through many levels, eg, offering HIV/AIDS education to migrant individuals and communities and setting national policies focusing on HIV/AIDS control (a 100% condom campaign, for instance).46 This review however did not illustrate practical approaches on how these policies could be linked together. According to the conceptual framework for tackling SDH inequalities,29 intersectoral action, social participation, and empowerment in the design and implementation of policies were essential to success in addressing SDHs. This point also coincided with that previously discussed, ie, how HIV/AIDS programs for migrants would survive constructively by their own resources and capacity if support from international development agencies was to be curtailed.
Limitations of the study
This study contains certain limitations. First, it is the nature of a scoping review to aim to identify, gather, and summarize articles in order to obtain a comprehensive understanding in a particular research area of interest, not to scrutinize a specific set of questions like a traditional systematic review.89 Another key difference is that a systematic review requires explicit methodologies to assess the quality of included articles, and it requires a full range of search engines where necessary. On the contrary, a scoping review does not necessarily delve into quality assessment of the selected literature. The merit of the scoping review lies in producing a profile of the existing evidence in a specific topic and creating a rich database that will be a foundation for more detailed reviews in an area where existing research is scarce.90 Another reason for not having assessed the scientific quality of the selected publications was the vast heterogeneity of the characteristics of the reviewed articles, unlike a clinical study, which in general practice has a clear set of common quality-assessment tools.
The second limitation is the language restriction. Non-English-language articles were not included due to limited capacity to identify and understand them and lack of access to translation services. This point is fully acknowledged and should be improved in further research, when deeper reviews on a well-defined set of research questions are warranted.91 Third, the review relied heavily on systematic search strategies, but less focus was directed at gray-literature searches. Gray literature in original articles should be further explored if the research question is to be more focused. Though the reviewed literature ransacked evidence from LMICs, it has not been possible to delve into the details of each individual country. Finally, when applying the findings of this review to actual practice, one should bear in mind that this study drew experiences only from LMICs that served as destination sites for migrants. More primary research is required to obtain better understanding of the interacting mechanisms between migrants and the general health systems available for native populations, taking into account differences in socioeconomic background and contextual environment between countries.
Last but not least, it should be noted that extrapolating the results of this study to a wider population should be done with caution, as the study concentrated on cross-country migrants, who were identified by specified search terms like “migrants” and “refugees.” However, in real practice, it is difficult to distinguish migrants or refugees with other hard-to-reach population subgroups, such as people with citizenship problems, ethnic minorities, and other transient populations, due to an overlapping in definition. Regardless of the obscurity in definition, health systems should enable these populations to access standard quality services in equitable fashion. How to achieve such a goal is worth exploring in any future studies.
Conclusion
It was clearly suggested that HIV/AIDS epidemics among cross-country migrants are a major concern in many LMICs, especially for those residing in sub-Saharan Africa. The high prevalence of HIV/AIDS was associated with a number of factors hindering access to health care services in migrant populations. These impediments included inadequate management of guidelines and referral systems, discriminatory attitudes, language differences, and financial hardship. Health systems management for HIV/AIDS in migrant populations had great varieties in benefit packages, human resources, health care financing, and types of collaborations between implementing institutes. Although there are many global partners involved heavily in HIV/AIDS care, there was little evidence concerning either the sustainability or the effectiveness of such involvement. Future studies are recommended to determine the interaction between HIV/AIDS health care services for migrant populations and existing health systems for native populations, taking into account differences in socioeconomic background and contextual environment between countries.
Author contributions
RS, PL, and WP jointly designed the study; data collection was conducted by RS, KK, and PL. RS, AS, CK, CT, KK, PJ, TT, and TW contributed to analyzing the data. All authors contributed to the drafting, revision, finalization, and approval of the manuscript.
Acknowledgments
The authors would like to thank Dr Viroj Tangcharoensathien, Dr Phusit Prakongsai, and Dr Suwit Wibulpolprasert, who continuously supported everyone involved in this study. We also appreciate all IHPP staff for their kind coordination and facilitating the whole working process. This study was funded by IHPP core resources.
Disclosure
The authors report no conflicts of interest in this work.
References
De Cock KM, Ekpini E, Gnaore E, Kadio A, Gayle HD. The public health implications of AIDS research in Africa. JAMA. 1994;272(6):481–486. | |
Dixon S, McDonald S, Roberts J. The impact of HIV and AIDS on Africa’s economic development. BMJ. 2002;324(7331):232–234. | |
Rosen S, Vincent JR, MacLeod W, Fox M, Thea DM, Simon JL. The cost of HIV/AIDS to businesses in southern Africa. AIDS. 2004;18(2):317–324. | |
Umenai T, Narula M, Onuki D, Yamamoto T, Igari T. International HIV and AIDS prevention: Japan/United States collaboration. J Acquir Immune Defic Syndr Hum Retrovirol. 1997;14 Suppl 2:S58–S67. | |
Hecht R, Alban A, Taylor K, Post S, Andersen NB, Schwarz R. Putting it together: AIDS and the millennium development goals. PLoS Med. 2006;3(11):e455. | |
United Nations Programme on HIV/AIDS. Global Report: UNAIDS report on the Global AIDS Epidemic 2012. Geneva: UNAIDS; 2012. | |
Gupta RK, Wainberg MA, Brun-Vezinet F, et al. Oral antiretroviral drugs as public health tools for HIV prevention: global implications for adherence, drug resistance, and the success of HIV treatment programs. J Infect Dis. 2013;207 Suppl 2:S101–S106. | |
Carney DN. The biology of lung cancer. Curr Opin Oncol. 1992;4(2):292–298. | |
World Health Organization. Health of Migrants – The Way Forward: Report of a Global Consultation, Madrid, Spain, March 3–5, 2010. France: WHO; 2010. | |
Bandyopadhyay M, Thomas J. Women migrant workers’ vulnerability to HIV infection in Hong Kong. AIDS Care. 2002;14(4):509–521. | |
Li L, Morrow M, Kermode M. Rural-to-urban male migrant workers’ vulnerability to HIV infection in Chengdu, China: qualitative findings from a mixed-method study. Work. 2010;37(4):375–386. | |
Albarran CR, Nyamathi A. HIV and Mexican migrant workers in the United States: a review applying the vulnerable populations conceptual model. J Assoc Nurses AIDS Care. 2011;22(3):173–185. | |
Shedlin MG, Drucker E, Decena CU, et al. Immigration and HIV/AIDS in the New York Metropolitan Area. J Urban Health. 2006;83(1):43–58. | |
Poudel KC, Poudel-Tandukar K, Jimba M. HIV/AIDS vulnerability of Nepali migrants to India: whose concern? Lancet. 2006; 368(9548):1648. | |
Sherer R, Stieglitz K, Narra J, et al. HIV multidisciplinary teams work: support services improve access to and retention in HIV primary care. AIDS Care. 2002;14 Suppl 1:S31–S44. | |
Desclaux A, Kouanda S, Obermeyer CM. Stakeholders’ participation in operational research on HIV care: insights from Burkina Faso. AIDS. 2010;24 Suppl 1:S79–S85. | |
United Nations Programme on HIV/AIDS. Background Paper: People on the Move – Forced Displacement and Migrant Populations. Geneva: UNAIDS; 2009. | |
World Health Organization. Workers’ Health: Global Plan of Action. Geneva: WHO; 2007. | |
World Health Organization. Health of Migrants. Geneva: WHO; 2008. | |
Mladovsky P, Rechel B, Ingleby D, McKee M. Responding to diversity: an exploratory study of migrant health policies in Europe. Health Policy. 2012;105(1):1–9. | |
Rechel B, Mladovsky P, Deville W. Monitoring migrant health in Europe: a narrative review of data collection practices. Health Policy. 2012;105(1):10–16. | |
Gray BH, van Ginneken E. Health care for undocumented migrants: European approaches. Issue Brief (Commonw Fund). 2012;33:1–12. | |
European Centre for Disease Prevention and Control. Thematic report: HIV Treatment, Care and Support. Monitoring Implantation of the Dublin Declaration on Partnership to Fight HIV/AIDS in Europe and Central Asia: 2012 Progress Report. Stockholm: ECDC; 2013. | |
International Organization for Migration. International Dialogue on Migration (IDM): addressing mixed migration Flows. 2009. Available from: http://www.iom.int/jahia/webdav/shared/shared/mainsite/about_iom/en/council/96/Mixed_Migration_Flows_FINAL.pdf. Accessed December 6, 2013. | |
United Nations Secretary-General. Globalization and Interdependence: International Migration and Development. Geneva: UN; 2006. | |
Weeks L, Strudsholm T. A scoping review of research on complementary and alternative medicine (CAM) and the mass media: looking back, moving forward. BMC Complement Altern Med. 2008;8:43. | |
European Union Agency for Fundamental Rights. Migrants in an Irregular Situation: Access to Healthcare in 10 European Union Member States. Luxembourg: FRA; 2011. | |
World Health Organization. Everybody Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action. Geneva: WHO; 2007. | |
World Health Organization. A Conceptual Framework for Action on the Social Determinants of Health. Geneva: WHO; 2010. | |
World Bank. World development indicators. 2013. Available from: http://data.worldbank.org/data-catalog/world-development-indicators. Accessed September 30, 2013. | |
Rees D, Murray J, Nelson G, Sonnenberg P. Oscillating migration and the epidemics of silicosis, tuberculosis, and HIV infection in South African gold miners. Am J Ind Med. 2010;53(4):398–404. | |
Stephen H, Roberts B. A case study of the provision of antiretroviral therapy for refugees in Tanzania. Med Confl Surviv. 2009;25(2):134–147. | |
Spiegel PB, Bennedsen AR, Claass J, et al. Prevalence of HIV infection in conflict-affected and displaced people in seven sub-Saharan African countries: a systematic review. Lancet. 2007;369(9580):2187–2195. | |
Karkee R, Shrestha DB. HIV and conflict in Nepal: relation and strategy for response. Kathmandu Univ Med J (KUMJ). 2006;4(3):363–367. | |
Nepal B. Population mobility and spread of HIV across the Indo-Nepal border. J Health Popul Nutr. 2007;25(3):267–277. | |
United Nations Development Programme Asia-Pacific Regional Centre. Regional Dialogue on the Health Challenges for Asian Labour Migrants. Bangkok: UNDP; 2010. | |
Caballero-Hoyos R, Torres-Lopez T, Pineda-Lucatero A, Navarro-Nuñez C, Fosados R, Valente TW. Between tradition and change: condom use with primary sexual partners among Mexican migrants. AIDS Behav. 2008;12(4):561–569. | |
Holt BY, Effler P, Brady W, et al. Planning STI/HIV prevention among refugees and mobile populations: situation assessment of Sudanese refugees. Disasters. 2003;27(1):1–15. | |
Busza J, Baker S. Protection and participation: an interactive programme introducing the female condom to migrant sex workers in Cambodia. AIDS Care. 2004;16(4):507–518. | |
Magis-Rodríguez C, Gayet C, Negroni M, et al. Migration and AIDS in Mexico: an overview based on recent evidence. J Acquir Immune Defic Syndr. 2004;37 Suppl 4:S215–S226. | |
Trippayya V. Botswana: Refugees not entitled to same services as citizens. HIV AIDS Policy Law Rev. 2005;10(3):27–28. | |
Lippman SA, Kerrigan D, Chinaglia M, Díaz J. Chaos, co-existence, and the potential for collective action: HIV-related vulnerability in Brazil’s international borders. Soc Sci Med. 2007;64(12):2464–2475. | |
Olshefsky AM, Zive MM, Scolari R, Zuñiga M. Promoting HIV risk awareness and testing in Latinos living on the US-Mexico border: the Tú No Me Conoces social marketing campaign. AIDS Educ Prev. 2007;19(5):422–435. | |
Poudel KC, Jimba M, Poudel-Tandukar K, Wakai S. Reaching hard-to-reach migrants by letters: an HIV/AIDS awareness programme in Nepal. Health Place. 2007;13(1):173–178. | |
Rachlis B, Brouwer KC, Mills EJ, Hayes M, Kerr T, Hogg RS. Migration and transmission of blood-borne infections among injection drug users: understanding the epidemiologic bridge. Drug Alcohol Depend. 2007;90(2–3):107–119. | |
Ford K, Chamratrithirong A. Migrant seafarers and HIV risk in Thai communities. AIDS Educ Prev. 2008;20(5):454–463. | |
Plewes K, Lee T, Kajeechewa L, et al. Low seroprevalence of HIV and syphilis in pregnant women in refugee camps on the Thai-Burma border. Int J STD AIDS. 2008;19(12):833–837. | |
Sowell RL, Holtz CS, Velasquez G. HIV infection returning to Mexico with migrant workers: an exploratory study. J Assoc Nurses AIDS Care. 2008;19(4):267–282. | |
Weine S, Bahromov M, Mirzoev A. Unprotected Tajik male migrant workers in Moscow at risk for HIV/AIDS. J Immigr Minor Health. 2008;10(5):461–468. | |
Michinobu R. “HIV is irrelevant to our company”: everyday practices and the logic of relationships in HIV/AIDS management by Japanese multinational corporations in northern Thailand. Soc Sci Med. 2009;68(5):941–948. | |
Golobof A, Weine S, Bahromov M, Luo J. The roles of labor migrants’ wives in HIV/AIDS risk and prevention in Tajikistan. AIDS Care. 2011;23(1):91–97. | |
Munyewende P, Rispel LC, Harris B, Chersich M. Exploring perceptions of HIV risk and health service access among Zimbabwean migrant women in Johannesburg: a gap in health policy in South Africa? J Public Health Policy. 2011;32 Suppl 1: S152–S161. | |
Rangel MG, Martinez-Donate AP, Hovell MF, et al. A two-way road: rates of HIV infection and behavioral risk factors among deported Mexican labor migrants. AIDS Behav. 2012;16(6):1630–1640. | |
United Nations Institute for Training and Research. Briefing Report: HIV, AIDS and Migration. New York: UNITAR; 2006. | |
United Nations Institute for Training and Research. Summary Report: Panel on Migration, Brain Drain and Caregiving. New York: UNITAR; 2009. | |
International Organization for Migration. Migration Health: Report of Activities 2008-2009. Geneva: IOM; 2009. | |
International Organization for Migration. Migration and Health in South Africa: A Review of the Current Situation and Recommendations for Achieving the World Health Assembly Resolution on the Health of Migrants. Pretoria: IOM; 2010. | |
World Health Organization Regional Office for Europe. How Health Systems Can Address Health Inequities Linked to Migration and Ethnicity. Copenhagen: WHO Regional Office for Europe; 2010. | |
Mooney A, Sarangi S. An ecological framing of HIV preventive intervention: a case study of non-government organizational work in the developing world. Health (London). 2005;9(3):275–296. | |
Poudel KC, Jimba M, Okumura J, Joshi AB, Wakai S. Migrants’ risky sexual behaviours in India and at home in far western Nepal. Trop Med Int Health. 2004;9(8):897–903. | |
Weine SM, Kashuba AB. Labor migration and HIV risk: a systematic review of the literature. AIDS Behav. 2012;16(6):1605–1621. | |
Tanaka Y, Kunii O, Hatano T, Wakai S. Knowledge, attitude, and practice (KAP) of HIV prevention and HIV infection risks among Congolese refugees in Tanzania. Health Place. 2008;14(3):434–452. | |
Rutta E, Gongo R, Mwansasu A, et al. Prevention of mother-to-child transmission of HIV in a refugee camp setting in Tanzania. Glob Public Health. 2008;3(1):62–76. | |
Tansey E, Theyise N, Borland R, West H. Southern Africa ports as spaces of HIV vulnerability: case studies from South Africa and Namibia. Int Marit Health. 2010;62(4):233-240. | |
Smart R. HIV/AIDS Guide for the Mining Sector. Washington: International Finance Corporation; 2004. | |
World Bank. Additional Financing for Total War Against HIV and AIDS (TOWA) Project: Indigenous Peoples Planning Framework. Nairobi: World Bank; 2010. | |
Mboup S, Musonda R, Mhalu F, Essex M. HIV/AIDS. In: Jamison DT, Feachem RG, Makgoba MW, et al, editors. Disease and Mortality in Sub-Saharan Africa. 2nd ed. Washington: World Bank; 2006:237–246. | |
United Nations Economic and Social Commission for Asia and the Pacific. International migration. Available from: http://www.unescapsdd.org/international-migration. Accessed September 30, 2013. | |
International Organization for Migration. Asia and the Pacific: regional overview. 2013. Available from: http://www.iom.int/cms/en/sites/iom/home/where-we-work/asia-and-the-pacific.html. Accessed September 30, 2013. | |
Pellowski JA. Barriers to care for rural people living with HIV: a review of domestic research and health care models. J Assoc Nurses AIDS Care. 2013;24(5):422–437. | |
Govindasamy D, Ford N, Kranzer K. Risk factors, barriers and facilitators for linkage to antiretroviral therapy care: a systematic review. AIDS. 2012;26(16):2059–2067. | |
Deblonde J, De Koker P, Hamers FF, Fontaine J, Luchters S, Temmerman M. Barriers to HIV testing in Europe: a systematic review. Eur J Public Health. 2010;20(4):422–432. | |
Nkulu Kalengayi FK, Hurtig AK, Ahlm C, Krantz I. Fear of deportation may limit legal immigrants’ access to HIV/AIDS-related care: a survey of Swedish language school students in Northern Sweden. J Immigr Minor Health. 2012;14(1):39–47. | |
Mahajan AP, Sayles JN, Patel VA, et al. Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. AIDS. 2008;22 Suppl 2:S67–S79. | |
Arah OA, Klazinga NS, Delnoij DM, Asbroek AH, Custers T. Conceptual frameworks for health systems performance: a quest for effectiveness, quality, and improvement. Int J Qual Health Care. 2003;15(5):377–398. | |
Suphanchaimat R, Wisaijohn T, Thammathacharee N, Tangcharoensathien V. Projecting Thailand physician supplies between 2012 and 2030: application of cohort approaches. Hum Resour Health. 2013;11(1):3. | |
Hall T. Why plan human resources for health? Hum Resour Health. 1998;2(2):77–86. | |
Selke HM, Kimaiyo S, Sidle JE, et al. Task-shifting of antiretroviral delivery from health care workers to persons living with HIV/AIDS: clinical outcomes of a community-based program in Kenya. J Acquir Immune Defic Syndr. 2010;55(4):483–490. | |
Fairall L, Bachmann MO, Lombard C, et al. Task shifting of antiretroviral treatment from doctors to primary-care nurses in South Africa (STRETCH): a pragmatic, parallel, cluster-randomised trial. Lancet. 2012;380(9845):889–898. | |
Emdin CA, Millson P. A systematic review evaluating the impact of task shifting on access to antiretroviral therapy in sub-Saharan Africa. Afr Health Sci. 2012;12(3):318–324. | |
Culyba RJ, McGee BT, Weyer D. Changing HIV clinical knowledge and skill in context: the impact of longitudinal training in the Southeast United States. J Assoc Nurses AIDS Care. 2011;22(2):128–139. | |
O’Brien K, Bone G, Sinclair L, Solomon P. Rehabilitation in the context of HIV: an interprofessional multi-stakeholder process for curriculum development. J Allied Health. 2010;39(3):131–137. | |
Martin P. The Economic Contribution of Migrant Workers to Thailand: Towards Policy Development. 1st ed. Bangkok: ILO Subregional Office for East Asia; 2007. | |
Patcharanarumol W, Thammatacharee N, Kittidilokkul S, et al. Thailand’s HIV/AIDS program after weaning-off the global fund’s support. BMC Public Health. 2013;13(1):1008. | |
The Global Fund. Policy on eligibility criteria, counterpart financing requirements, and prioritization of proposals for funding from the Global Fund. Paper presented at: Twenty-Third Board Meeting; May 11–12, 2011; Geneva. | |
Weine S, Bahromov M, Loue S, Owens L. Trauma exposure, PTSD, and HIV sexual risk behaviors among labor migrants from Tajikistan. AIDS Behav. 2012;16(6):1659–1669. | |
Huang W, Operario D, Dong Y, et al. HIV-related risk among female migrants working in entertainment venues in China. Prev Sci. Epub August 7, 2013. | |
Wong JP, Li AT, Poon MK, Fung KP. An exploratory study on the mental health of immigrants, refugees and non-status people living with HIV in Toronto. Int J Migr Health Soc Care. 2013;9(3):122–134. | |
Levac D, Colquhoun H, O’Brien K. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. | |
Brien S, Lorenzetti D, Lewis S, Kennedy J, Ghali W. Overview of a formal scoping review on health system report cards. Implement Sci. 2010;5:2. | |
Smith V, Devane D, Begley C, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol. 2011;11(1):15. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.