")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Heart rate and blood pressure responses during hypoxic cycles of a 3-week intermittent hypoxia breathing program in patients at risk for or with mild COPD
Authors Faulhaber M, Gatterer H, Haider T, Linser T, Netzer N, Burtscher M
Received 13 October 2014
Accepted for publication 6 December 2014
Published 11 February 2015 Volume 2015:10(1) Pages 339—345
DOI https://doi.org/10.2147/COPD.S75749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Martin Faulhaber,1 Hannes Gatterer,1 Thomas Haider,2 Tobias Linser,1 Nikolaus Netzer,1 Martin Burtscher1
1Department of Sport Science, University of Innsbruck, Innsbruck, Austria; 2Institute of Veterinary Physiology, University of Zurich, Zurich, Switzerland
Abstract: The aim of this study was to provide information on heart rate and blood pressure responses during a 3-week intermittent hypoxia breathing program in COPD patients. Sixteen participants with COPD symptoms were randomly assigned to a hypoxia or control group and completed a 3-week intermittent hypoxia breathing program (five sessions per week, each consisting of three to five breathing cycles, each cycle lasting 3–5 minutes with 3-minute breaks between cycles). During the breathing cycles, the hypoxia group received hypoxic air (inspired fraction of oxygen 15%–12%), whereas the control group received normal air (sham hypoxia). During the breaks, all participants breathed normoxic room air. Arterial oxygen saturation, systolic and diastolic blood pressure, and heart rate were measured during the normoxic and hypoxic/sham hypoxic periods. For each breathing cycle, changes from normoxia to hypoxia/sham hypoxia were calculated, and changes were averaged for each of the 15 sessions and for each week. Changes in arterial oxygen saturation were significantly different between groups in the course of the 3 weeks (two-way analysis of variance for repeated measures), with post hoc differences in weeks 1, 2, and 3. During the course of the intermittent hypoxia application, no between-group differences were detected for blood pressure or rate pressure product values. Changes in heart rate were significantly different between groups in the course of the 3 weeks (two-way analysis of variance for repeated measures), with post hoc differences only in week 3. Averages over all 15 sessions were significantly higher in the hypoxia group for heart rate and rate pressure product, and tended to be increased for systolic blood pressure. The applied intermittent hypoxia breathing program resulted in specific and moderate heart rate and blood pressure responses, and did not provoke a progressive increase in blood pressure during the hypoxic cycles in the course of the application.
Keywords: interval hypoxia, blood pressure, cardiovascular responses
Introduction
Intermittent hypoxia (IH) is defined as repeated episodes of hypoxia interspersed with normoxic periods.1 Physiological effects of IH on the cardiorespiratory system depend on the severity of hypoxia, the duration of a single hypoxic exposure, the relation of hypoxic and normoxic phases, the total time of the IH application and eventual concomitant stimuli during the hypoxic periods (eg, exercise, hypo- or hypercapnia).2 Among the broad variety of IH protocols in clinical and physiologic studies, repeated passive short-term (3–5 minutes) hypoxic cycles (inspired fraction of oxygen [FiO2] 0.15–0.09) with normoxic intervals have been applied in patients and healthy subjects by physicians of the former Soviet Union for many years.3,4 Recently, well-controlled studies confirmed the positive effects of IH application in elderly with and without coronary artery disease5 and in patients with various diseases,6–10 and proposed IH as a preventive and therapeutic tool even for patients with mild COPD.6,7 Although the authors reported that the IH application was well tolerated by all subjects without adverse effects, these studies focused on changes from the pre- to the postapplication period, and little is known on hemodynamic responses of COPD patients during the course of an IH breathing program.6,7
For a safe application of IH, it is important not to provoke potentially dangerous hemodynamic responses during the repeated short-term exposures to hypoxia. Acute hypoxic exposure increases heart rate and cardiac output via β-adrenergic stimulation, and can result in higher blood pressure and rate pressure product.11,12 Chronic IH has been shown to result in long-term facilitation in sympathetic nerve activity associated with augmented blood pressure responses to hypoxia.13 Since an abrupt and clinically relevant rise in heart rate or blood pressure might be a potential risk for patients, the goal of the present study was to provide information on the arterial oxygen saturation, heart rate, and blood pressure responses during a 3-week IH breathing program, and to analyze if the responses depend on the severity of the hypoxia provided during the breathing sessions.
Materials and methods
The present study was part of an IH project performed in Innsbruck (Austria). Parts of the project have already been published, and the recruitment of the study participants, including inclusion and exclusion criteria and the baseline examination are described in detail in our previous publication.6 In brief, the study was approved by the ethics committee of the Medical University Innsbruck (Austria) and carried out in conformity with the ethical standards laid down in the 1975 Declaration of Helsinki. Eighteen female and male patients with symptoms of COPD volunteered to participate in the study and gave written informed consent. After baseline examination, the participants were randomly assigned in a single-blind fashion to the hypoxia group (HG) or the control group (CG) with sham hypoxia. In two study participants, complete measurements during all sessions of the IH application were not possible. Therefore, the present evaluation includes data of 16 study participants. Baseline characteristics and medication of the study participants of the HG and the CG are shown in Table 1.
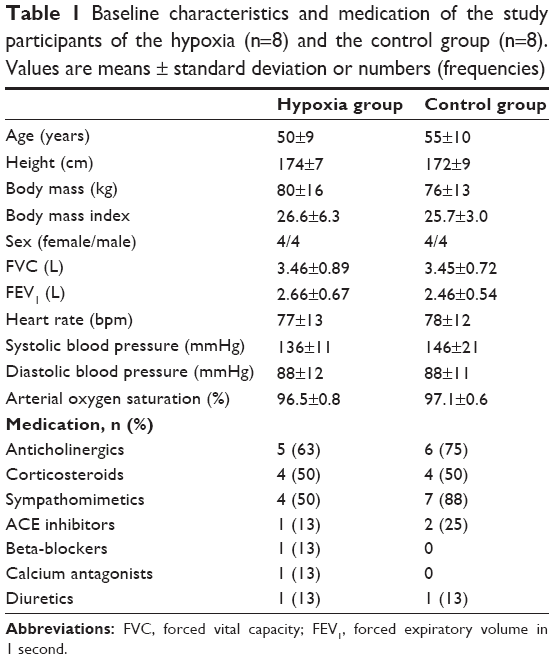 | Table 1 Baseline characteristics and medication of the study participants of the hypoxia (n=8) and the control group (n=8). Values are means ± standard deviation or numbers (frequencies) |
Both groups completed a 3-week IH breathing program (HypoxyComplex HypO2; HypoMed, Moscow, Russia), comprising five sessions per week, each consisting of three to five breathing cycles, which was conducted at the Department of Sport Science of the University of Innsbruck, Austria (590 m altitude). The characteristics of the breathing program are described in Table 2. The breathing sessions started in the late morning at least 1 hour after a usual breakfast, and participants performed no intense physical exercise for at least 1 hour prior to the breathing sessions. The breathing sessions started after about 10 minutes’ rest in a sitting position, and the complete breathing sessions were conducted in a sitting position. During the breathing cycles, the HG received hypoxic air (FiO2 15%–12%), whereas the CG (sham) received normal air (FiO2 21%). Hypoxia and sham hypoxia were administered via air-cushion face mask directly connected to a T-valve to minimize dead space. The breathing cycles lasted 3–5 minutes and were separated by 3-minute breaks, during which all participants breathed normoxic room air (FiO2 21%) without a face mask. The participants were advised not to change nutrition or exercise habits during the breathing program.
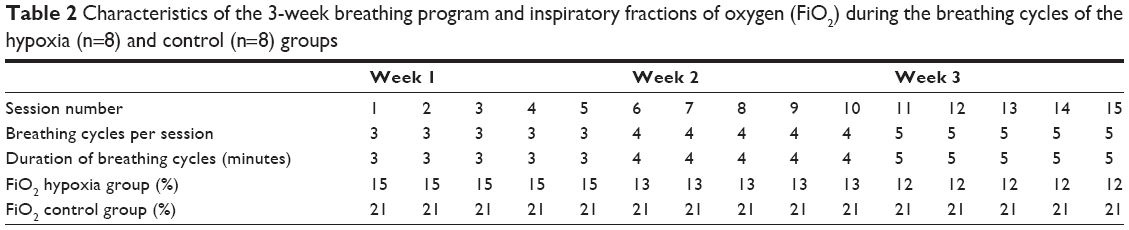 | Table 2 Characteristics of the 3-week breathing program and inspiratory fractions of oxygen (FiO2) during the breathing cycles of the hypoxia (n=8) and control (n=8) groups |
Heart rate and arterial oxygen saturation (SaO2) were continuously monitored during the sessions via a pulse oximeter (Hypoxia Patient Monitor; HypoMed) attached to a fingertip, and values were recorded at the end of the normoxic and of the hypoxic/sham hypoxic period of each breathing cycle. Systolic and diastolic blood pressure were measured during the last 30 seconds of the normoxic and of the hypoxic/sham hypoxic periods of each breathing cycle using an automatic wrist blood pressure monitor (RX3 Plus; Omron, Mannheim, Germany). No measures were visible for the participants.
For data evaluation, changes (Δ) between normoxia and hypoxia/sham hypoxia of each breathing cycle were calculated, and values of the three (week 1) to five (week 3) breathing cycles of each session were averaged. Therefore, the values of SaO2 (ΔSaO2), systolic and diastolic blood pressure (ΔBPsys, ΔBPdia), mean arterial blood pressure (ΔMAP), heart rate (ΔHR), and rate pressure product (ΔRPP) represent mean differences from normoxia to hypoxia/sham hypoxia of each breathing session. These values were used for the descriptive presentation of the physiological responses in the course of the IH application. Mean values of each week were calculated (Δweek-SaO2, Δweek-BPsys, Δweek-BPdia, Δweek-HR, Δweek-RPP) for the statistical analysis of FiO2-related differences between groups, and a two-way analysis of variance for repeated measures (week × group) was applied. If a significant interaction was found, post hoc unpaired t-tests with Bonferroni correction were applied to find the source of difference. Additionally, averages over all 15 sessions (Δtot-SaO2, Δtot-BPsys, Δtot-BPdia, Δtot-MAP, Δtot-HR, Δtot-RPP) were calculated and compared between groups by unpaired t-tests. Data analyses were conducted by PASW Statistics 19 (IBM, Vienna, Austria). P-values <0.05 were considered to indicate statistical significance. Values are presented as means ± standard deviation.
Results
Arterial oxygen saturation
Changes in SaO2 from normoxia to hypoxia/sham hypoxia (Δ-SaO2) of each breathing session are shown in Figure 1. There was a significant interaction (week × group) for Δweek-SaO2. Post hoc analysis revealed significant differences between groups for week 1 (HG −3.7%±2.3%, CG 0.2%±0.6%, P<0.01), week 2 (HG −7.8%±3.9%, CG 0.3%±0.9%; P<0.01), and week 3 (HG −10.0%±3.3%, CG 0.3%± 0.7%; P<0.01). Δtot-SaO2 differed between groups (HG −7.2%±3.0%, CG −0.3%±0.7%; P<0.01). With respect to reoxygenation between the breathing cycles, SaO2 during room-air breathing (mean value of all 15 sessions) was not different between the two groups (HG 95.9%±0.5%, CG 96.2%±0.8%; P=0.29 for comparison by unpaired t-test).
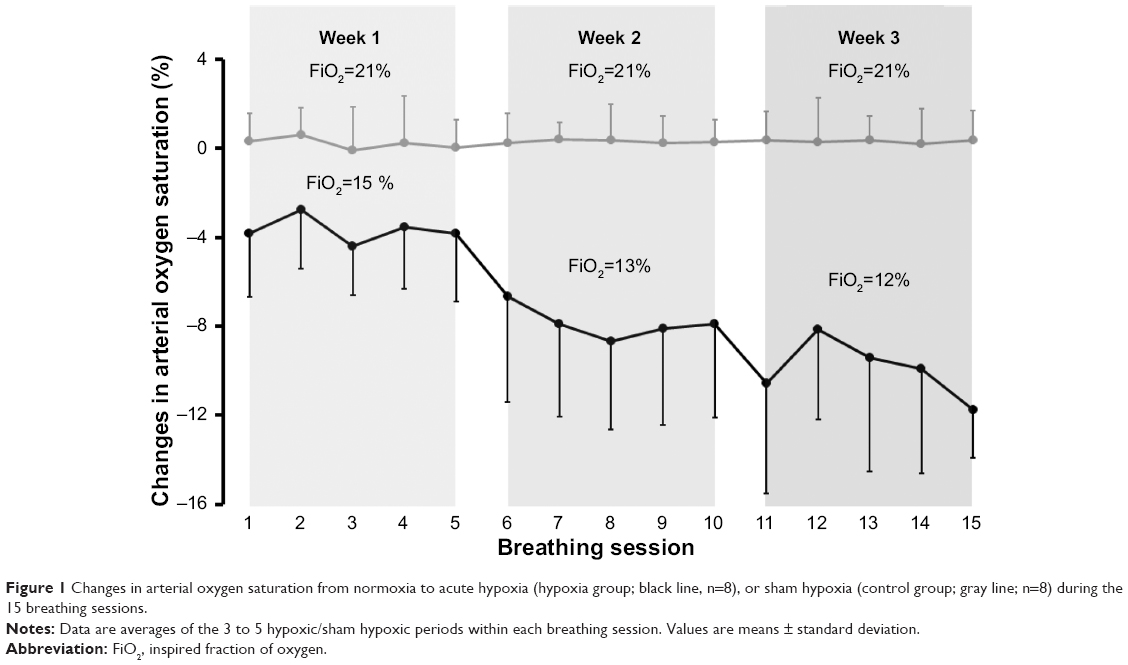 | Figure 1 Changes in arterial oxygen saturation from normoxia to acute hypoxia (hypoxia group; black line, n=8), or sham hypoxia (control group; gray line; n=8) during the 15 breathing sessions. |
Blood pressure, heart rate, and rate pressure product
ΔBPsys, ΔBPdia, ΔMAP, ΔHR, and ΔRPP from normoxia to hypoxia/sham hypoxia of each breathing session are shown in Figure 2. ΔBPsys ranged from −2.4±6.1 to 4.9±10.5 mmHg in the HG and from −6.0±9.4 to 1.9±8.4 mmHg in the CG. ΔBPdia varied from −0.3±3.8 to 3.1±4.1 mmHg in the HG and from −2.8±4.2 to 1.3±2.1 mmHg in the CG. ΔMAP ranged from −0.7±4.1 to 3.7±6.1 mmHg in the HG and from −3.1±3.4 to 0.9±4.2 mmHg in the CG. ΔHR varied from 0.3±3.7 to 5.3±3.4 bpm in the HG and from −1.5±2.3 to 2.5±5.9 bpm in the CG. ΔRPP ranged from 1.6±11.9 to 7.7±8.4 in the HG and from −5.9±11.2 to 3.8±12.1 in the CG. There was no significant interaction (week × group) for Δweek-BPsys, Δweek-BPdia, Δweek-MAP, or Δweek-RPP, whereas a significant interaction was observed for Δweek-HR (P=0.03). Post hoc analysis revealed a significant between-group difference for week 3 (HG 6.0%±4.0%, CG −1.5±3.6 bpm, P<0.01) (see Figure 3). Δtot-BPsys tended to differ between groups (HG 1.0±3.2 mmHg, CG −2.2±3.5 mmHg; P=0.08). Δtot-BPdia (HG 1.1±2.7 mmHg, CG −0.8±2.5 mmHg) and Δtot-MAP (HG 1.0±2.7 mmHg, CG −1.3±2.7 mmHg) showed no differences between groups (P=0.17 and P=0.11, respectively). Δtot-HR (HG 3.3±2.4 bpm, CG 0.7±2.1 bpm; P=0.04) and Δtot-RPP (HG 5.0±4.4, CG −0.6±4.8; P=0.03) were different between groups.
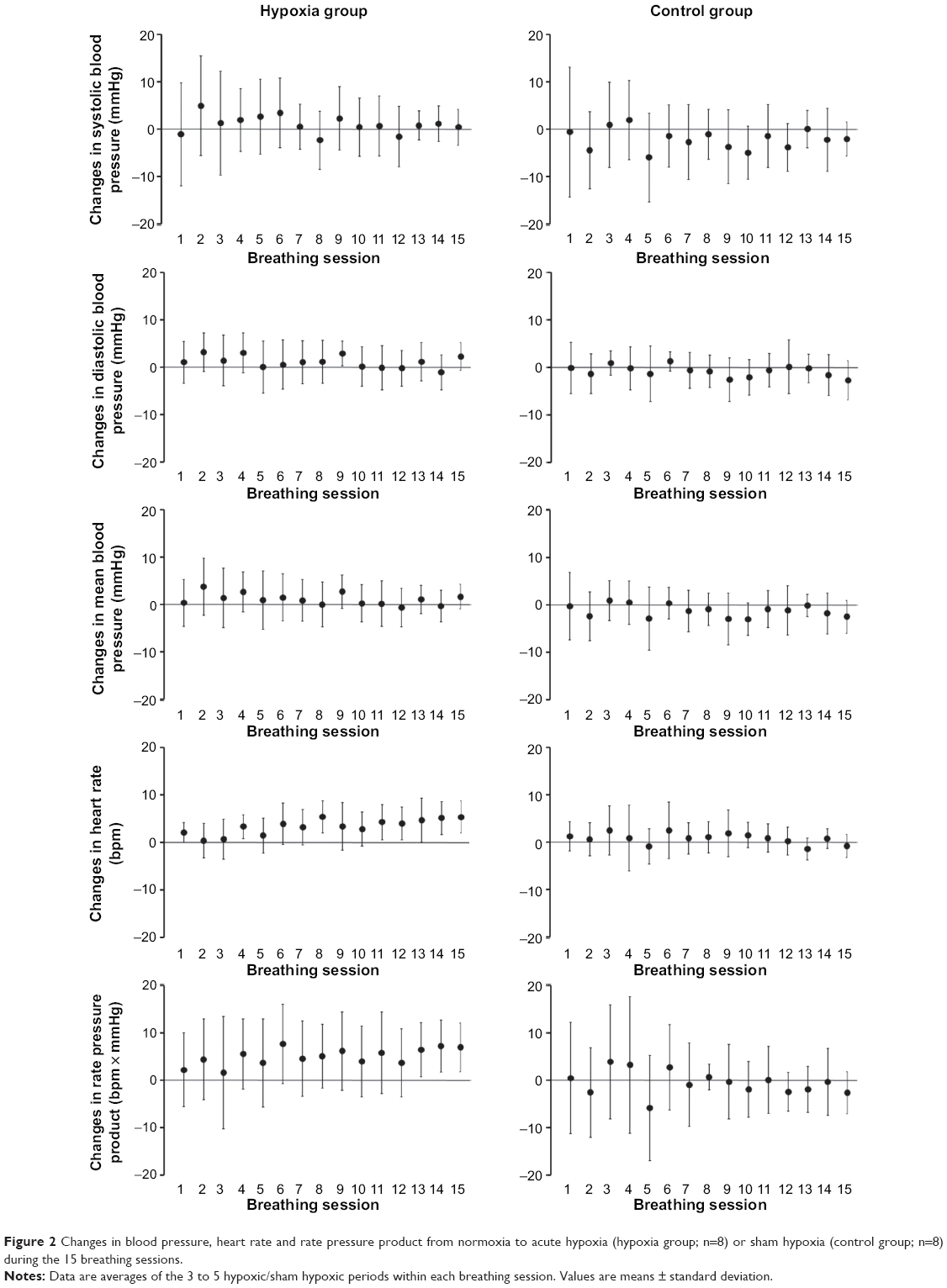 | Figure 2 Changes in blood pressure, heart rate and rate pressure product from normoxia to acute hypoxia (hypoxia group; n=8) or sham hypoxia (control group; n=8) during the 15 breathing sessions. |
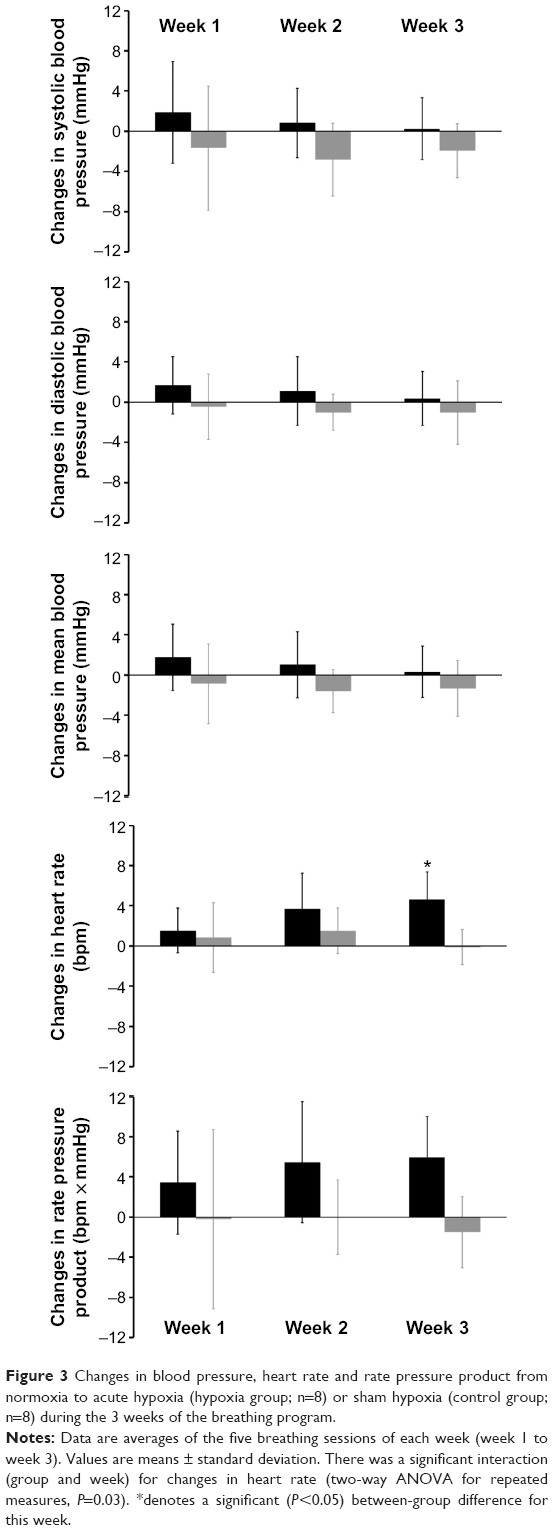 | Figure 3 Changes in blood pressure, heart rate and rate pressure product from normoxia to acute hypoxia (hypoxia group; n=8) or sham hypoxia (control group; n=8) during the 3 weeks of the breathing program. |
Discussion
To the best of our knowledge, this is the first study analyzing heart rate and blood pressure responses during 3 weeks’ repeated short-term (3–5 minutes) hypoxia provoked by a decreasing FiO2. The applied IH protocol provoked a marked decrease in SaO2 during the hypoxic cycles in weeks 1, 2, and 3. Although slightly increased, blood pressure values were not significantly influenced by the hypoxic periods. Heart rate was significantly increased during the hypoxic cycles, and increases were dependent on the degree of hypoxia. As a consequence of the hypoxia-induced modulations of blood pressure and heart rate, the rate pressure product was affected by the hypoxic cycles, and a significant difference between the HG and CG was detected for means over all 15 sessions.
The hypoxia-induced heart rate increase in the HG was relatively low, with a maximal ΔHR of 5.3 bpm in sessions 8 and 15. Δtot-HR was (about 4 bpm) significantly higher in the HG compared to the CG. The observed heart rate responses were unsurprising, since acute hypoxic exposure has been shown to increase resting heart rate and cardiac output to counteract the reduced arterial oxygen content and to match oxygen delivery to the tissues.14,15 Additionally, acute hypoxia reduces peripheral vascular resistance, which may contribute to a heart rate increase via baroreflex.
With respect to individual heart rate responses, the maximal heart rate increase from normoxia to hypoxia/sham hypoxia was 13 bpm in both groups. The increase in ΔHR over the course of the 15 breathing sessions might have been caused by lowered inspired fraction of oxygen from week 1 to week 3 that resulted in an SaO2 decrease in the participants of the HG (see Figure 1). When compared to physical activity, eg, an endurance-training program, the applied IH program provoked heart rate increases in all participants that were below low-intensity exercise.
IH provoked only minor changes in blood pressure values, which did not differ between groups. On the one hand, normotensive subjects seemed not to respond with increased blood pressure to acute hypoxia, since the effects of the increased cardiac output are counteracted by peripheral vasodilation.16 On the other hand, repeated exposures to hypoxia can increase sympathetic activation, with increased blood pressure responses in normoxia and during hypoxic exposures.17 Our results indicate that the increased cardiac output was compensated by peripheral vasodilation, resulting in nearly unchanged blood pressure, which is in line with the results of Fu et al.18 The reasons for the divergent effects of IH application on blood pressure parameters might be the different study populations (eg, patients, athletes, etc). However, it is more likely that the pattern of IH and the duration of application are responsible for the effects on blood pressure.19
According to the heart rate and blood pressure responses, the rate pressure product was increased during the hypoxic cycles compared to sham hypoxia predominantly caused by changes in heart rate. From a practical point of view, the moderate increases in rate pressure product seem not to be a cardiovascular provocation and support the records of previous studies that the application of repeated hypoxic short-term exposures at rest are well tolerated by healthy and mildly diseased persons, even by patients after myocardial infarction.5–7
The present results are based on a relatively small sample size of patients with mild COPD. This is responsible for the relatively low statistical power. Although all participants had normal SaO2 values, determined in the baseline examination,6 it cannot be excluded, that these persons were already preconditioned by COPD-related hypoxic periods before starting the breathing program. Therefore, the results cannot be transferred to healthy subjects or patients with more severe COPD without limitations. The measurements were performed at the end of each breathing cycle. Due to the short circulation time from the lungs to the carotid bodies,13 it might be possible that physiological responses were exaggerated during the first minute of the hypoxic cycles and were not detected by our measurements.
It has to be stated that IH was applied as a training period in this study setting. IH was present for about 20–40 minutes per day and the application was limited to 3 weeks. In COPD patients with additional obstructive sleep apnea, the repeated hypoxic episodes during the night seem to be responsible for a higher hospitalization and mortality rate.20 In contrast, sleep-related oxygen desaturation in COPD patients without obstructive sleep apnea seems to have no detrimental effect.21 The applied IH protocol in this study differs from IH in obstructive sleep apnea in the duration of the single hypoxic periods, the duration of normoxic phases, concomitant hypocapnia instead of hypercapnia, and the limited duration per day and in total. These differences might be responsible for the positive effects of the applied IH protocol on exercise tolerance6 and for the mild heart rate and blood pressure responses observed in this study, which were in contrast to the detrimental effects of IH in obstructive sleep apnea patients.
In conclusion, the applied IH program resulted in specific heart rate and blood pressure responses, ie, a moderate increase in heart rate, during the hypoxic cycles. Although hypoxia was progressively increased from week 1 to week 3, the applied IH program seems not to provoke a progressive increase in blood pressure during the hypoxic cycles. Therefore, IH using repeated 3- to 5-minute cycles can be considered a mild stimulus accompanied by effective adaptations in patients with mild COPD.6,7 However, larger clinical trials including patients with various COPD stages are needed to assess the clinical utility of IH training in COPD patients.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Neubauer JA. Invited review: Physiological and pathophysiological responses to intermittent hypoxia. J Appl Physiol (1985). 2001;90(4):1593–1599. | ||
Faulhaber M, Gatterer H, Haider T, Patterson C, Burtscher M. Intermittent hypoxia does not affect endurance performance at moderate altitude in well-trained athletes. J Sports Sci. 2010;28(5):513–519. | ||
Meerson FZ, Ustinova EE, Orlova EH. Prevention and elimination of heart arrythmias by adaptation to intermittent high altitude hypoxia. Clin Cardiol. 1987;10(12):783–789. | ||
Serebrovskaya TV. Intermittent hypoxia research in the former Soviet Union and the Commonwealth of Independent States: history and review of the concept and selected applications. High Alt Med Biol. 2002;3(2):205–221. | ||
Burtscher M, Pachinger O, Ehrenburg I, et al. Intermittent hypoxia increases exercise tolerance in elderly men with and without coronary artery disease. Int J Cardiol. 2004;96(2):247–254. | ||
Burtscher M, Haider T, Domej W, et al. Intermittent hypoxia increases exercise tolerance in patients at risk for or with mild COPD. Respir Physiol Neurobiol. 2009;165(1):97–103. | ||
Haider T, Casucci G, Linser T, et al. Interval hypoxic training improves autonomic cardiovascular and respiratory control in patients with mild chronic obstructive pulmonary disease. J Hypertens. 2009;27(8):1648–1654. | ||
Lyamina NP, Lyamina SV, Senchiknin VN, Mallet RT, Downey HF, Manukhina EB. Normobaric hypoxia conditioning reduces blood pressure and normalizes nitric oxide synthesis in patients with arterial hypertension. J Hypertens. 2011;29(11):2265–2272. | ||
Duennwald T, Gatterer H, Groop PH, Burtscher M, Bernardi L. Effects of a single bout of interval hypoxia on cardiorespiratory control and blood glucose in patients with type 2 diabetes. Diabetes Care. 2013;36(8):2183–2389. | ||
Duennwald T, Bernardi L, Gordin D, et al. Effects of a single bout of interval hypoxia on cardiorespiratory control in patients with type 1 diabetes. Diabetes. 2013;62(12):4220–4227. | ||
Ledderhos C, Pongratz H, Exner J, Gens A, Roloff D, Honig A. Reduced tolerance of simulated altitude (4200 m) in young men with borderline hypertension. Aviat Space Environ Med. 2002;73(11):1063–1066. | ||
Naeije R. Physiological adaptation of the cardiovascular system to high altitude. Prog Cardiovasc Dis. 2010;52(6):456–466. | ||
Prabhakar NR, Peng YJ, Jacono FJ, Kumar GK, Dick TE. Cardiovascular alterations by chronic intermittent hypoxia: importance of carotid body chemoreflexes. Clin Exp Pharmacol Physiol. 2005;32(5–6):447–449. | ||
Buchheit M, Richard R, Doutreleau S, Lonsdorfer-Wolf E, Brandenberger G, Simon C. Effect of acute hypoxia on heart rate variability at rest and during exercise. Int J Sports Med. 2004;25(4):264–269. | ||
Naeije R, Mélot C, Mols P, Hallemans R. Effects of vasodilators on hypoxic pulmonary vasoconstriction in normal man. Chest. 1982;82(4):404–410. | ||
Wolfel EE, Levine BD. The cardiovascular system at high altitude: heart and systemic circulation. In: Hornbeit TF, Schoene RB, editors. High Altitude: An Exploration of Human Adaptation. New York: Marcel Dekker; 2001:235–292. | ||
Katayama K, Shima N, Sato Y, et al. Effect of intermittent hypoxia on cardiovascular adaptations and response to progressive hypoxia in humans. High Alt Med Biol. 2001;2(4):501–508. | ||
Fu Q, Townsend NE, Shiller SM, et al. Intermittent hypobaric hypoxia exposure does not cause sustained alterations in autonomic control of blood pressure in young athletes. Am J Physiol Regul Integr Comp Physiol. 2007;292(5):R1977–R1984. | ||
Serebrovskaya TV, Manukhina EB, Smith ML, Downey HF, Mallet RT. Intermittent hypoxia: cause of or therapy for systemic hypertensionΔ Exp Biol Med. 2008;233(6):627–650. | ||
Marin JM, Soriano JB, Carrizo SJ, Boldova A, Celli BR. Outcomes in patients with obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Am J Respir Care Med. 2010;182(3):325–331. | ||
Chaouat A, Weitzenblum E, Kessler R, et al. Outcome of COPD patients with mild daytime hypoxaemia with or without sleep-related oxygen desaturation. Eur Respir J. 2001;17(5):848–855. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.