")
Back to Journals » OncoTargets and Therapy » Volume 8
GSTM1 null genotype and gastric cancer risk in the Chinese population: an updated meta-analysis and review
Authors Zhang X, Cui Y, Peng X
Received 11 December 2014
Accepted for publication 2 March 2015
Published 28 April 2015 Volume 2015:8 Pages 969—975
DOI https://doi.org/10.2147/OTT.S79099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jianmin Xu
Xi-Liang Zhang, Yong-Hui Cui
Department of Gastroenterology, The First People’s Hospital of Shangqiu City, Shangqiu, Henan, People’s Republic of China
Abstract: Although a number of studies have been conducted on the association between the GSTM1 null genotype and gastric cancer in People’s Republic of China, this association remains elusive and controversial. To clarify the effects of the GSTM1 null genotype on the risk of gastric cancer, an updated meta-analysis was performed in the Chinese population. Related studies were identified from PubMed, Springer Link, Ovid, Chinese Wanfang Data Knowledge Service Platform, Chinese National Knowledge Infrastructure (CNKI), and Chinese Biology Medicine (CBM) up to November 5, 2014. A total of 25 studies including 3,491 cases and 5,921 controls were included in this meta-analysis. Overall, a significant association (odds ratio [OR] =1.47, 95% CI: 1.28–1.69) was found between the null GSTM1 and gastric cancer risk when all studies in Chinese population were pooled into the meta-analysis. In subgroup analyses stratified by quality score, geographic area, and source of controls, the same results were observed. Additionally, a significant association was found both in smokers and non-smokers. This meta-analysis showed that the null GSTM1 may be a potential biomarker for gastric cancer risk in Chinese, and further studies with gene–gene and gene–environment interactions are required for definite conclusions.
Keywords: meta-analysis, GSTM1, polymorphism, gastric cancer
Introduction
The incidence and mortality of gastric cancer have declined dramatically over the past several decades. Nonetheless, gastric cancer remains a major public health issue as the fourth most common cancer and the second most frequent cause of cancer death worldwide.1 A total of 989,600 new stomach cancer cases and 738,000 deaths are estimated to have occurred in 2008, accounting for 8% of the total cases and 10% of total deaths.1 Over 70% of new cases and deaths occur in developing countries, with the majority in People’s Republic of China.1 The mechanism of gastric carcinogenesis is still not fully understood. It has been suggested that low-penetrance susceptibility genes combining with environmental factors may be important in the development of cancer.2 In recent years, several common low-penetrant genes have been identified as potential gastric cancer susceptibility genes. An important one is glutathione S-transferase (GST), which consists of five distinct classes, namely alpha (GSTA), sigma (GSTS), mu (GSTM), pi (GSTP), and theta (GSTT).3 Located on the chromosome 1p13.3, the GSTM1 plays an important role in the detoxification of xenobiotics. The most common genotype of GSTM1 gene is a homozygous deletion (null genotype), which has been suggested to be associated with the loss of enzyme activity and increased vulnerability to cytogenetic damage that resulted in the increased susceptibility to cancer.4,5 An association between the GSTM1 null genotype and gastric cancer was first reported by Strange et al in 1991 among Britain’s population.6 As a consequence, many studies analyzed the influence of the GSTM1 null genotype on gastric cancer risk; however, no clear consensus was reached. Meta-analyzes of studies of the GSTM1 null genotype in other ethnic groups have been reported elsewhere and produced conflicting results.7–13 In order to lessen the impact of different genetic backgrounds, we performed this update meta-analysis to assess the relationship of the GSTM1 null genotype with risk of gastric cancer in Chinese population.
Materials and methods
Search strategy
The studies were searched in PubMed, Springer Link, Ovid, Chinese Wanfang Data Knowledge Service Platform, Chinese National Knowledge Infrastructure (CNKI), and Chinese Biology Medicine (CBM) up to November 5, 2014. The keywords used were combinations of the following terms: (1) GSTM1 or GST M1; (2) gastric cancer or gastric neoplasm or stomach tumor; (3) polymorphism or variant or variation; and (4) Chinese or China or Taiwan. The search was performed without any restrictions on language and focused on studies conducted in humans. Besides, the references from retrieved articles were also searched.
Inclusion and exclusion criteria
The criteria used to select studies for this meta-analysis were as follows: (1) independent cohort or case–control studies for human; (2) all patients with the diagnosis of gastric cancer confirmed by pathological or histological examinations; (3) the distribution of the GSTM1 null genotype in patients and controls provided; and (4) all participants were Chinese. The reasons for exclusion of studies were: (1) duplicate publications; (2) incomplete data; (3) no control; and (4) meta-analyses, letters, reviews, or editorial articles.
Data extraction
Relevant data were extracted from all the eligible studies independently by the two reviewers according to the inclusion criteria listed above. Disagreement was resolved by discussion between the two authors. The following data were extracted from the identified studies: the first author, publication year, source of controls, geographic area, sample size, and the number of subjects with two GSTM1 genotypes. In this meta-analysis, the quality assessment of individual study was conducted according to the nine-star Newcastle–Ottawa Scale.14
Statistical analysis
We examined the association between the GSTM1 null genotype and gastric cancer risk by calculating pooled odds ratio (OR), with 95% confidence intervals (CIs). The significance of the pooled OR was determined by the Z-test. Given that there was distribution of null/present heterozygote in only one study selected, the Hardy–Weinberg equilibrium (HWE) test could not be conducted. Cochrane’s Q-test was performed to test the between-study heterogeneity. If there was heterogeneity, then the random-effects model was chosen to pool the ORs with 95% CIs, otherwise the fixed-effects model was used. Moreover, subgroup analyses were performed to test whether the effect size varied by the smoking status, quality score, geographic area, and the source of control population. Publication bias was investigated with the funnel plot, in which the standard error (SE) of log OR of each study was plotted against its OR. Funnel plot asymmetry was further assessed by the method of Egger’s linear regression test.15 All the P-values were two sided. P-value less than 0.05 was considered statistically significant. All statistical analysis was conducted by using Stata version 10.0 (Stata Corp, College Station, Texas, USA).
Results
Study selection
According to the inclusion criteria, 25 case–control studies16–40 were included and 54 articles were excluded. The publication year of involved studies ranged from 2000 to 2012. The flowchart of study selection is shown in Figure 1. In total, 3,491 gastric cancer cases and 5,921 controls were involved in this meta-analysis, which evaluated the relationship between GSTM1 polymorphism and gastric cancer risk. The source of controls was mainly based on a healthy population. The characteristics of the included studies are summarized in Table 1.
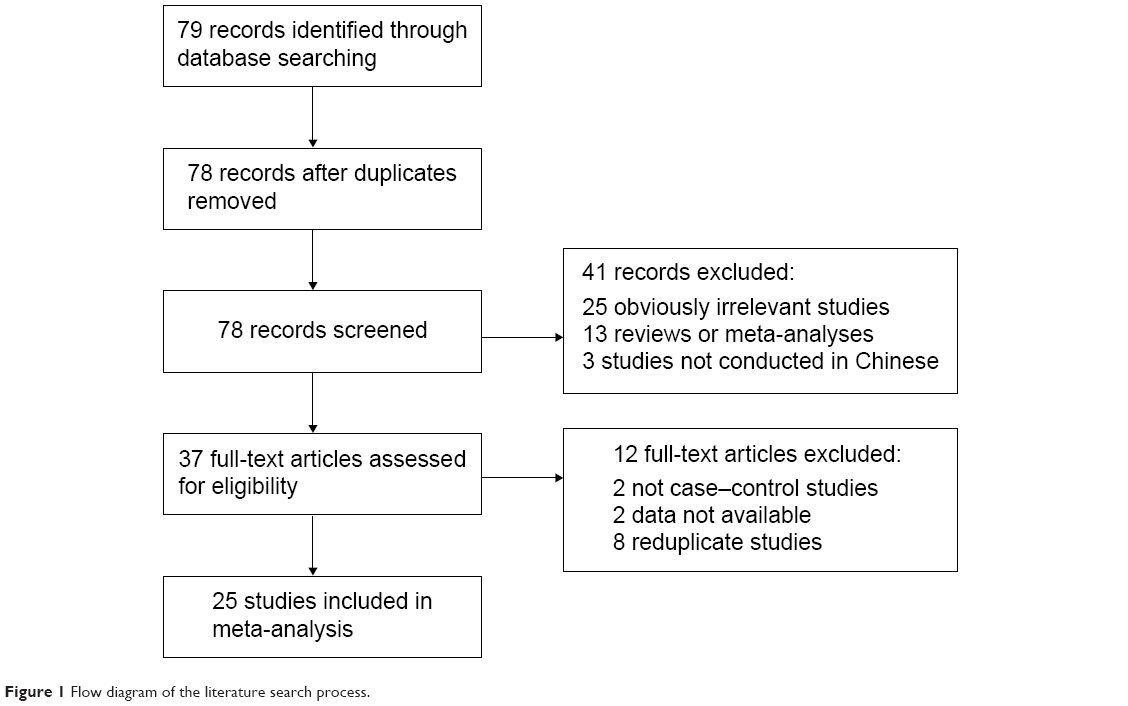 | Figure 1 Flow diagram of the literature search process. |
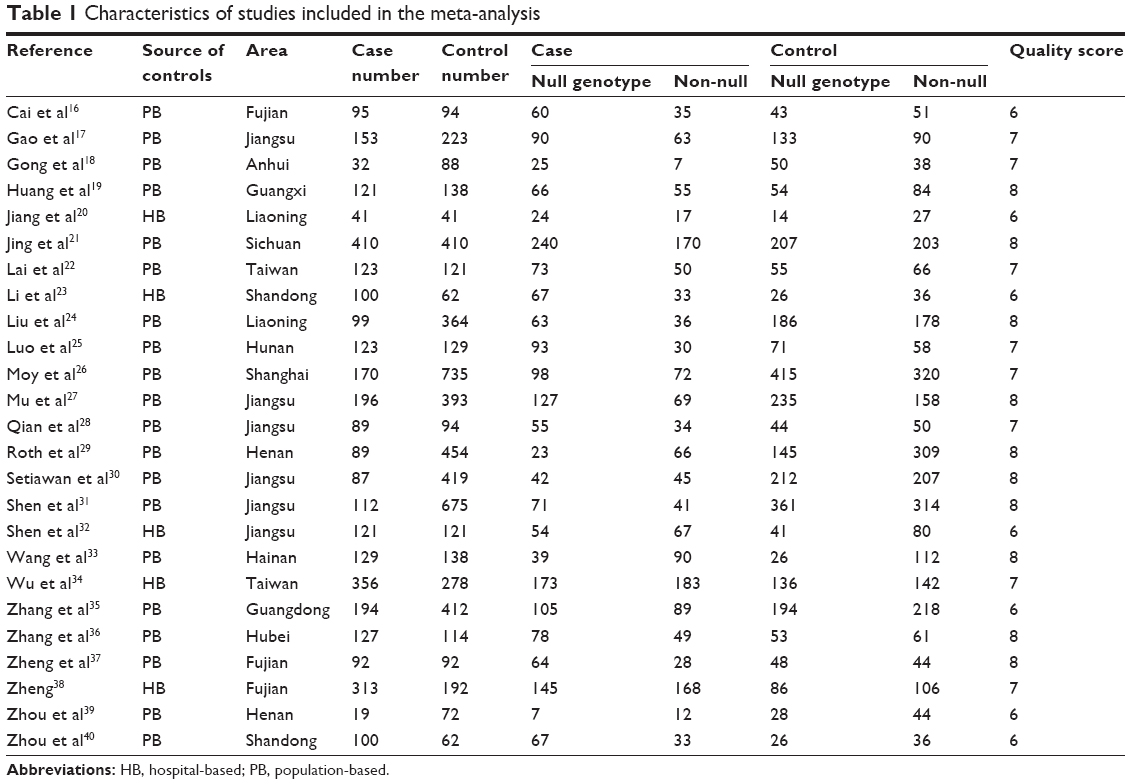 | Table 1 Characteristics of studies included in the meta-analysis |
Overall analysis
There was evidence of between-study heterogeneity in all included studies (χ2=49.62, P=0.002). Therefore, the random-effects model was used in overall analysis. The results showed that the pooled OR with 95% CI for gastric cancer in Chinese with the GSTM1 null genotype was 1.47 (1.28–1.69) (Figure 2).
 | Figure 2 The forest plot of all selected studies on the association between GSTM1 polymorphism and gastric cancer risk in Chinese. |
Subgroup analysis
In the subgroup analysis based on smoking status, the results showed that the GSTM1 null genotype was significantly related to gastric cancer risk among smokers (OR =1.98, 95% CI: 1.28–3.06), as well as among non-smokers (OR =1.42, 95% CI: 1.11–1.81) (Table 2). In addition, we also performed stratified analysis based on the source of control, quality score, and geographic area. It revealed similar results with all the studies (Table 2).
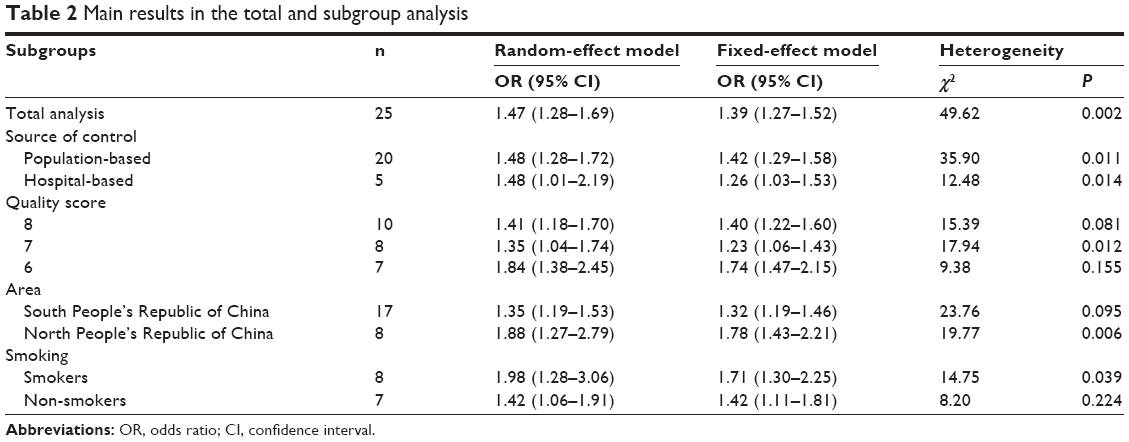 | Table 2 Main results in the total and subgroup analysis |
Sensitive analysis
To evaluate the stability of the results, we performed a sensitivity analysis by a different model. All the results were not materially altered (Table 2). Hence, the results of the sensitivity analysis suggest that the data in this meta-analysis are relatively stable and credible.
Bias diagnosis
The Begg’s funnel plot and Egger’s test were performed to assess the publication bias of literatures. As shown in Figure 3, the shape of the funnel plots did reveal obvious asymmetry. Similarly, the Egger’s test indicated some publication bias in the 25 reviewed studies (t=−2.65, P=0.014).
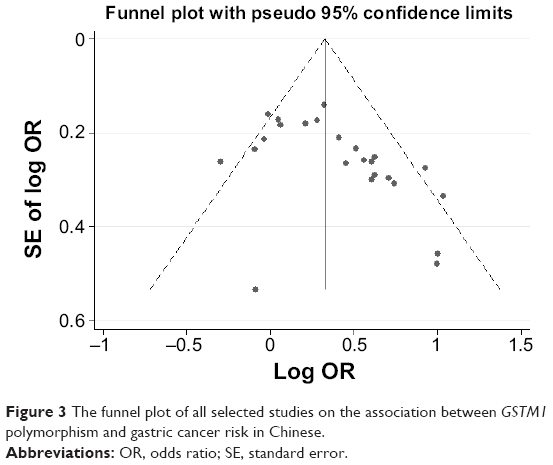 | Figure 3 The funnel plot of all selected studies on the association between GSTM1 polymorphism and gastric cancer risk in Chinese. |
Discussion
The GSTM1 enzyme is responsible for the metabolism of reactive electrophilic intermediates, including environmental pollutants and other polycyclic aromatic hydrocarbons, which are potent carcinogenic agents. Thus, impaired GSTM1 function may lead to serious DNA damage and carcinogenesis. Considering that null genotype causes a complete loss of GSTM1 enzyme activity, it is biologically plausible that the GSTM1 null genotype may increase risk of gastric cancer. Up to this time, a series of studies in People’s Republic of China have focused on the relation between the GSTM1 null genotype and gastric cancer risk. Nevertheless, the results were inconclusive and inconsistent. Some papers have reported that a statistically significant correlation was found between null GSTM1 and gastric cancer risk. Conversely, the results from other studies suggested that the null GSTM1 was not associated with gastric cancer risk. Therefore, we conducted this update meta-analysis by critically reviewing 25 individual studies on the GSTM1 null genotype with gastric cancer risk in the Chinese population. In the meta-analysis, we found that the GSTM1 null variant was significantly associated with gastric cancer risk in overall and subgroup analyses by source of control, quality score, and geographic area. To our knowledge, our study represented the first meta-analysis with a large sample size on the interaction of GSTM1 variant with gastric cancer in the Chinese population.
Furthermore, the interaction between the GSTM1 null genotype and tobacco smoking as a risk factor for gastric cancer has been evaluated by several studies with inconsistent results, possibly because of small sample size.41 Thus, we performed a stratified analysis by smoking status to ascertain the interaction by pooling all available studies. We found that the GSTM1 null genotype significantly increases the risk of gastric cancer, both in smokers and non-smokers. However, the risk conferred by null genotype is higher among smokers (OR =1.98, 95% CI: 1.28–3.06) than in non-smokers (OR =1.42, 95% CI: 1.11–1.81). Smoking habit was quite heterogeneous among eligible studies. It might make attributions for other unknown factors, such as dietary habits, drinking status, other environmental exposures, family history of cancer, other genetic-related respiratory diseases, as well as other related genetic polymorphisms. Moreover, the association between the extent of smoke exposure and gastric cancer risk was not clear; further studies with larger sample sizes are needed to provide insights into the interaction association.
The pathways of carcinogen metabolism are complex, mediated by the activity of multiple enzymes. The effect of any single gene might have a limited impact on gastric cancer risk than have so far been anticipated. The knowledge of environmental determinants and large studies with detailed exposure information are crucial to evaluate reliably any moderate genetic effects. Many controversial data are present in literature. Positive associations were found in certain populations and not confirmed in others. In addition to an expected interethnic variability in allele frequencies, variability has also been found within ethnic groups,42 resulting in heterogeneity in association studies. Gene–environment interactions could be a confounding factor in these studies, with controversial findings on cancer risk.
This study has some limitations. First, only published studies were included in the meta-analysis; therefore, publication bias may have occurred probably due to the exclusion of negative studies. It is evident that positive results had a greater probability of being published with respect to negative ones, even though unpublished studies are generally of lesser quality with respect to published ones. Second, we could not obtain information from most studies regarding infection with Helicobacter pylori, a strong risk factor for gastric cancer, and other several factors like salt intake, age, alcohol drinking, etc. Third, our results were based on unadjusted estimates.
Conclusion
In conclusion, this meta-analysis suggests that the GSTM1 null genotype is associated with gastric cancer among Chinese populations. The null genotype increased susceptibility to gastric cancer both in smokers and non-smokers. The risk conferred by the null genotype is higher among smokers than in non-smokers. Further studies analyzing gene–gene and gene–environment interactions are required. Such studies may eventually lead to have a better, comprehensive understanding of the association between the GSTM1 null genotype and gastric cancer risk.
Disclosure
The authors report no conflicts of interest in this work.
References
Jemal A, Bray F, Center MM, Ferlay F, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. | ||
Lichtenstein P, Holm NV, Verkasalo PK, et al. Environmental and heritable factors in the causation of cancer – analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000;343(2):78–85. | ||
Soya SS, Vinod T, Reddy KS, Gopalakrishnan S, Adithan C. Genetic polymorphisms of glutathione-S-transferase genes (GSTM1, GSTT1 and GSTP1) and upper aerodigestive tract cancer risk among smokers, tobacco chewers and alcoholics in an Indian population. Eur J Cancer. 2007;43(18):2698–2706. | ||
Hayes JD, Flanagan JU, Jowsey IR. Glutathione transferases. Annu Rev Pharmacol Toxicol. 2005;45:51–88. | ||
McIlwain CC, Townsend DM, Tew KD. Glutathione S-transferase polymorphisms: cancer incidence and therapy. Oncogene. 2006;25(11):1639–1648. | ||
Strange RC, Matharoo B, Faulder GC, et al. The human glutathione S-transferases: a case-control study of the incidence of the GST1 0 phenotype in patients with adenocarcinoma. Carcinogenesis. 1991;12(1):25–28. | ||
Meng X, Liu Y, Liu B. Glutathione S-transferase M1 null genotype meta-analysis on gastric cancer risk. Diagn Pathol. 2014;9:122. | ||
Zhao Y, Deng X, Song G, Qin S, Liu Z. The GSTM1 null genotype increased risk of gastric cancer: a meta-analysis based on 46 studies. PLoS One. 2013;8(11):e81403. | ||
Zhu Y, He Q, Wang J, Pan HF. The association between GSTM1 polymorphism and gastric cancer risk: a meta-analysis. Mol Biol Rep. 2012;39(1):685–691. | ||
Qiu LX, Wang K, Lv FF, et al. GSTM1 null allele is a risk factor for gastric cancer development in Asians. Cytokine. 2011;55(1):122–125. | ||
Chen B, Zhou Y, Yang P, Wu XT. Glutathione S-transferase M1 gene polymorphism and gastric cancer risk: an updated analysis. Arch Med Res. 2010;41(7):558–566. | ||
Wang H, Zhou Y, Zhuang W, et al. Glutathione S-transferase M1 null genotype associated with gastric cancer among Asians. Dig Dis Sci. 2010;55(7):1824–1830. | ||
La Torre G, Boccia S, Ricciardi G. Glutathione S-transferase M1 status and gastric cancer risk: a meta-analysis. Cancer Lett. 2005;217(1):53–60. | ||
Wells GA, Shea B, O’Connell D, et al. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality if Nonrandomized Studies in Meta-Analyses. Available from: www.ohri.ca/programs/clinical_epidemiology/oxford.htm | ||
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. | ||
Cai L, Yu SZ, Zhang ZF. Glutathione S-transferases M1, T1 genotypes and the risk of gastric cancer: a case-control study. World J Gastroenterol. 2001;7(4):506–509. | ||
Gao CM, Takezaki T, Wu JZ, et al. Glutathione-S-transferases M1 (GSTM1) and GSTT1genotype, smoking, consumption of alcohol and tea and risk of esophageal and stomach cancers: a case-control study of a high-incidence area in Jiangsu Province, China. Cancer Lett. 2002;188(1–2):95–102. | ||
Gong L, Sun HL, Xu YQ. [The study of correlations between the deletion of GSTM1 gene and gastric cancer]. Wan Nan Yi Xue Yuan Xue Bao. 2002;21(3):181–183. Chinese. | ||
Huang X, Lu YF, Xie NC, Zhang HT, Ning Z, Tan ZR. [A case-control study on the association between genetic polymorphism of GSTM1 and gastric cancer susceptibility in population from Guangxi province of China]. Wei Chang Bing Xue He Gan Bing Xue Za Zhi. 2009;18(2):97–99. Chinese. | ||
Jiang YH, Ju ZY, Ren CS. [Study on the relationship between the glutathiones-transferase gene deletion environmental factors and susceptibility to gastric carcinoma]. Zhong Guo Gong Gong Wei Sheng. 2000;16(10):877–879. Chinese. | ||
Jing C, Huang ZJ, Duan YQ, et al. Glulathione-S-transferases gene polymorphism in prediction of gastriccancer risk by smoking and Helicobacter pylori infection status. Asian Pac J Cancer Prev. 2012;13(7):3325–3328. | ||
Lai KC, Chen WC, Tsai FJ, Li SY, Chou MC, Jeng LB. Glutathione S-transferase M1 gene null genotype and gastric cancer risk in Taiwan. Hepatogastroenterology. 2005;52(66):1916–1919. | ||
Li H, Chen XL, Li HQ. Polymorphism of CYPIA1 and GSTM1 genes associated with susceptibility of gastric cancer in Shandong Province of China. World J Gastroenterol. 2005;11(37):5757–5762. | ||
Liu Y, Xu RT, Sun GF, Shang XL, Wang Q. [The relationship of GSTM1 gene homozygous deletion polymorphism and occurrence of gastric cancer]. Zhong Guo Yi Ke Da Xue Xue Bao. 2000;29(4):287–289. Chinese. | ||
Luo YP, Chen HC, Khan MA, et al. Genetic polymorphisms of metabolic enzymes-CYP1A1, CYP2D6, GSTM1, and GSTT1, and gastric carcinoma susceptibility. Tumour Biol. 2011;32(1):215–222. | ||
Moy KA, Yuan JM, Chung FL, et al. Isothiocyanates, glutathione S-transferase M1 and T1 polymorphisms and gastric cancer risk: a prospective study of men in Shanghai. China Int J Cancer. 2009;125(11): 2652–2659. | ||
Mu LN, Lu QY, Yu SZ, et al. Green tea drinking and multigenetic index on the risk of stomach cancer in a Chinese population. Int J Cancer. 2005;116(6):972–983. | ||
Qian Y, Xu YC, Shen HB, et al. [A molecular epidemiological study on the relationship between glutathione S-transferase M1, T1 genetic polymorphism and susceptibility to gastric cancer]. Zhong Guo Gong Gong Wei Sheng. 2001;17(1):101–103. Chinese. | ||
Roth MJ, Abnet CC, Johnson LL, et al. Polymorphic variation of Cyp1A1is associated with the risk of gastric cardia cancer: a prospective case-cohort study of cytochrome P-450 1A1 and GST enzymes. Cancer Causes Control. 2004;15(10):1077–1083. | ||
Setiawan VW, Zhang ZF, Yu GP, et al. GSTT1 and GSTM1 null genotypes and the risk of gastric cancer: a case-control study in a Chinese population. Cancer Epidemiol Biomarkers Prev. 2000;9(1):73–80. | ||
Shen J, Wang R, Xu X. Application of the interaction models between the polymorphism(s) of metabolic gene(s) and environmental exposure. Zhonghua Liu Xing Bing Xue Za Zhi. 2001;22(1):61–64. | ||
Shen XB, Pu XP, Zhang J, Zhu LJ. [Influence of GSTM1 and GSTT1 genotypes and smoking, alcohol exposure on the occurrence of gastric cancer: case-control study from Nanjing, China]. Huan Jing Yu Zhi Ye Yi Xue. 2005;22(4):325–329,382. Chinese. | ||
Wang WW, Yang WM, Zhang YX, Zhao SY. [Research on the relationship of the susceptibility to elderly gastric cancer and GSTM1 gene polymorphism in Hainan]. Xian Dai Yu Fang Yi Xue. 2012;39(23):6273–6274.Chinese. | ||
Wu MS, Chen CJ, Lin MT, et al. Genetic polymorphisms of cytochrome p450 2E1, glutathione S-transferase M1 and T1, and susceptibility to gastric carcinoma in Taiwan. Int J Colorectal Dis. 2002;17(5):338–343. | ||
Zhang AP, Liu BH, Wang L, Gao Y, Li F, Sun SX. Glutathione S-transferasegene polymorphisms and risk of gastric cancer in a Chinese population. Asian Pac J Cancer Prev. 2011;12(12):3421–3425. | ||
Zhang YC, Deng CS, Zhou Y, Zhu YQ. [Association of glutathione S-transferase M1 and T1 genetic polymorphisms with Helicobacter pyloriinfection and gastric adenocarcinoma]. Shi Jie Hua Ren Xiao Hua Za Zhi. 2003;11(9):1306–1309. Chinese. | ||
Zheng TR, Zheng QH, Gong FS, Xie YQ, Wang XR. [Gene deletion polymorphisms of GSTT1 and GSTM1 and susceptibility to stomach neoplasm]. Shi Yong Zhong Liu Za Zhi. 2002;17(3):155–157. Chinese. | ||
Zheng ZL. CYP2E1, GSTM1, GSTT1 polymorphisms and susceptibilities to cardia and non-cardia gastric cancer in high-risk area of China, The Master Thesis of Fujian Medical University, 2003. Chinese. | ||
Zhou Q, Zheng ZY, Wang LD, et al. [Prevalence of genetic polymorphisms of GSTM1, GSTT1 and GSTP1 in subjects with gastric cardia adenocarcinoma at Linzhou, Henan]. Zheng Zhou Da Xue Xue Bao (Yi Xue Ban). 2003;38(3):327–329. Chinese. | ||
Zhou T, Fan W, Han W, et al. [The study of the association of GSTM1 gene polymorphism with susceptibility to gastric cancer]. Chin J Curr Adv Gen Surg. 2006;9(6):355–358. Chinese. | ||
Shen J, Wang RT, Xu YC, Wang LW, Wang XR. Interaction models of CYP1A1, GSTM1 polymorphisms and tobacco smoking in intestinal gastric cancer. World J Gastroenterol. 2005;11(38):6056–6060. | ||
García-Martín E, Martínez C, Ladero JM, Agúndez JA. Interethnic and intraethnic variability of CYP2C8 and CYP2C9 polymorphisms in healthy individuals. Mol Diagn Ther. 2006;10(1):29–40. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.