")
Back to Journals » Patient Preference and Adherence » Volume 9
Factors associated with adherence to nucleos(t)ide analogs in chronic hepatitis B patients: results from a 1-year follow-up study
Authors Peng J, Yin J, Cai S, Yu T, Zhong C
Received 21 July 2014
Accepted for publication 29 September 2014
Published 7 January 2015 Volume 2015:9 Pages 41—45
DOI https://doi.org/10.2147/PPA.S71510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Jie Peng, Junhua Yin, Shaohang Cai, Tao Yu, Chunxiu Zhong
Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong Province, People’s Republic of China
Abstract: Little is known about the factors associated with patient compliance with nucleos(t)ide analog (NUC) treatment for chronic hepatitis B (CHB). The purpose of this study was to examine the association between sociodemographic and clinical characteristics and adherence to NUCs among patients with CHB. A total of 211 CHB patients receiving NUC monotherapy were asked to report the number of prescribed doses of medication they had taken during the last 90 days. A total of four 3-month adherence scores were averaged to obtain a combined rate of NUC adherence during a 1-year follow up period. The mean age of the patients was 29.6 years, 79% were men, and 68% had no prior NUC treatment for CHB. Females, patients without a previous NUC treatment, and those who had NUC drug resistance showed better adherence to NUC treatment, and compliance was better with telbivudine than with lamivudine and entecavir.
Keywords: chronic hepatitis B, nucleos(t)ide analogues, adherence, follow-up, resistance
Introduction
Hepatitis B virus (HBV) infection affects approximately 400 million people worldwide.1 In the People’s Republic of China, it is estimated that 20 million people suffer from chronic hepatitis B (CHB).2 Five nucleos(t)ide analogs (NUCs) approved to treat CHB include lamivudine, telbivudine, entecavir, adefovir dipivoxil, and tenofovir disoproxil fumarate.3 Although NUCs are potent medications that achieve long-term viral suppression, it is difficult to eradicate the virus.4 A recent study indicated that adults with CHB need more than 2 years of treatment with NUCs to reduce the risk of cirrhosis, CHB-related death, and hepatocellular carcinoma.5 In order to achieve virologic suppression and to avoid virologic breakthrough, medication adherence is very important.6 However, a study conducted by Ha et al7 found that nonadherence rates increased over time, with cumulative nonadherence rates at year 4 reaching 10% and 12% for patients taking adefovir and entecavir, respectively.
Optimal adherence to medication is necessary to achieve undetectable levels of HBV DNA. Consequently, the concern is that patients will not adhere to treatment over long periods and risk virologic failure.
Lieveld et al8 searched PubMed, Embase, the Cochrane Library, and the Web of Knowledge for articles on compliance with NUCs in the treatment of CHB and only found six that met their criteria. Mean adherence to various NUC treatment protocols varied from 81% to 91%, as reported in three studies.3,4,9 Two studies showed significant associations between good or perfect adherence and complete virologic suppression.10,11 Older age, a history of treatment for CHB using NUCs, use of NUCs other than lamivudine, and high income were shown to be associated with better NUC adherence.3,4,9,10 However, Giang et al12 found no association between age and adherence, and researchers dispute whether sex or baseline viral load are predictors of adherence.3,4 ,10–12
We feel that further study is warranted to help clarify these disputes. In the current study, we examined factors associated with adherence to NUC treatment for CHB prospectively in a Chinese population. NUCs are well tolerated, with minimal side effects,13–16 and we controlled for the influence of cost by providing medications at no charge. We show that female sex, no previous NUC treatment, and a history of NUC resistance are factors that promote adherence to NUCs. The difference between our findings and previous reports is discussed.
Materials and methods
Participating patients
A total of 222 CHB patients between 17 and 56 years of age who were either hepatitis B e antigen (HBeAg) positive or negative were recruited from the Nan-Fang Hospital of the Southern Medical University. Among them eleven patients were excluded because of coinfection with hepatitis C, hepatitis D, or human immunodeficiency virus; evidence of hepatic decompensation; cirrhosis or hepatocellular carcinoma; autoimmune hepatitis; and pregnancy. Patients with renal dysfunction and chronic renal failure were also excluded from the study. Because tenofovir was not approved for treatment of hepatitis B in Mainland China during the study period, a total of 211 CHB patients received NUC monotherapy of telbivudine, lamivudine, entecavir, or adefovir dipivoxil. There were 31 patients who developed drug resistance to lamivudine prior to the current study.
Study design
The study was conducted between November 2002 and July 2008. The protocol was approved by the Institutional Review Board of the Nan-Fang Hospital of the Southern Medical University. All patients signed informed consent forms before participating in the study. They were randomly assigned to receive 600 mg of telbivudine, 100 mg of lamivudine, 0.5 mg of entecavir, or 10 mg of adefovir dipivoxil once daily as oral treatment. At enrollment, demographic characteristics (age and sex) were collected and height and body weight were assessed. Information such as current and previous HBV treatments, family history of CHB, and HBV markers were examined. Patients were asked to return for a follow-up visit every 3 months for 1 year to assess adherence to treatment. Pills were counted at each visit, and patients were asked about the numbers of tablets taken and missed in the last 90 days.
Adherence was measured by patient self-reports. The patients were asked how many prescribed doses of medication they had taken during the last 90 days. Because the rate of adherence is usually expressed as the percentage of prescribed dosages the patient consumed,17 the rates of four periods were averaged for each participant.
Statistical analyses
The data analyses were done with SAS (version 9.2), and a P-value <0.05 was considered statistically significant. We used generalized estimating equations (GEEs)18 to test the relationship of interest because GEEs have better control than other statistical measures for within-subject correlations over time as a result of multiple visits. In the GEE model, the dependent variable was the percentage of consumed dosages of medication prescribed (adherence to NUCs), and the independent variables were age, sex, HBeAg status, types of NUC medication (telbivudine, lamivudine, entecavir, or adefovir dipivoxil), history of NUC treatment, and history of drug resistance.
Results
Sociodemographic and clinical characteristics of the study patients
Table 1 outlines the baseline characteristics of all patients. A total of 211 CHB patients who participated in the NUC monotherapy were included in the analysis. Of the 211 patients, the mean age was 29.6±7.8 years. Overall, 137 (65%) of the 211 patients were positive for HBeAg. A total of 143 (68%) patients were NUC-naïve, and 68 (32%) patients had received prior NUC treatment. There were 63 (30%), 27 (13%), 20 (9%), and 101 (48%) patients taking telbivudine, lamivudine, entecavir, and adefovir, respectively.
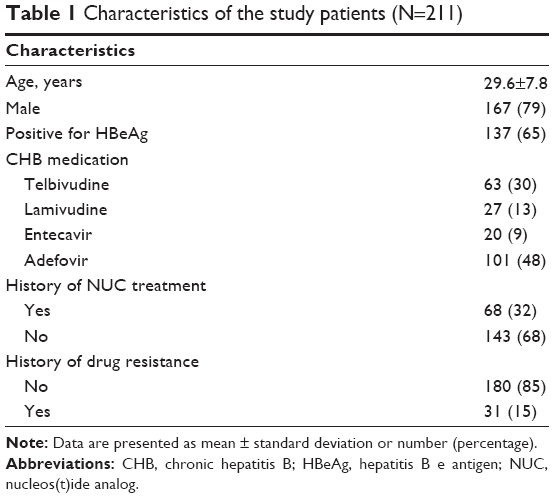 | Table 1 Characteristics of the study patients (N=211) |
Factors associated with adherence
Results of the regression analysis using GEEs are presented in Table 2. Female sex (b=0.96, P<0.001), the absence of prior NUC treatment (b=1.19, P<0.01), and a history of NUC drug resistance were significantly associated with better adherence to NUCs (b=2.07, P<0.001). Further analysis showed the adherence rate of NUC-naïve patients was 1.28% higher than of those with a history of NUC treatment. Compared to patients taking telbivudine, those who took lamivudine or entecavir showed worse adherence (b=−1.21, P=0.02; b=−1.05, P=0.01, respectively). Although adherence to adefovir was lower than to telbivudine, the difference did not achieve statistical significance (b=−0.29, P=0.31). Figure 1 shows the mean adherence rates across the four time periods (12, 24, 36, 48 weeks) separately for the four different NUC medications.
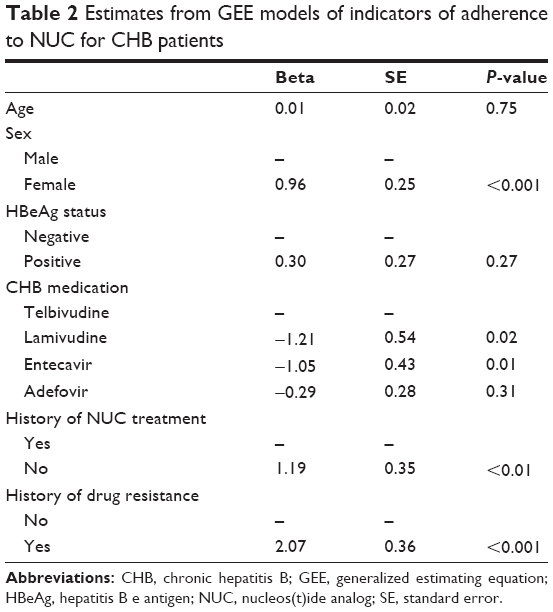 | Table 2 Estimates from GEE models of indicators of adherence to NUC for CHB patients |
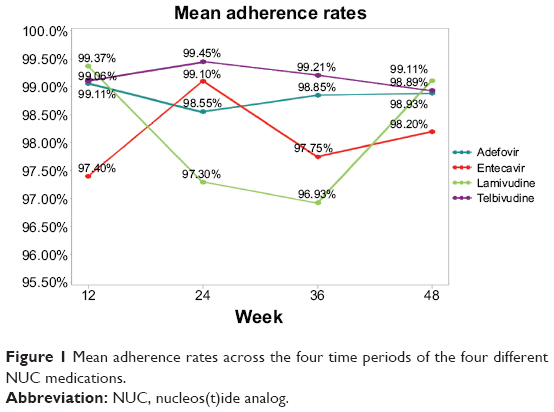 | Figure 1 Mean adherence rates across the four time periods of the four different NUC medications. |
Discussion
Although NUCs have been shown to be efficacious in the treatment of CHB,19,20 the concern remains that nonadherence may lead to treatment failure.11 With one out of 20 CHB sufferers worldwide living in the People’s Republic of China and drugs available to treat the disease, it is important to determine the factors associated with adherence in this population.1 Here we report that female sex, the absence of previous NUC treatment, and a history of NUC drug resistance are factors associated with greater NUC adherence, and patients adhere to telbivudine better than to lamivudine and entecavir.
In studies of adherence to antihypertensive medications, it was found that female patients have higher medication adherence rates than males.21,22 However, according to a systematic review on the factors affecting therapeutic compliance, inconsistent results have been obtained regarding sex-related adherence.23 Chotiyaputta et al3,4 reported that men and women did not differ in adherence rates. The reasons for the disagreement between their findings and our results are not known. Possible contributing factors are different ages, cultural and educational background, and household income level. Moreover, in the studies by Chotiyaputta et al there were near perfect adherence rates, which might be inflated in the patients’ self-reporting to health providers.3,4 This high rate may have some masking effect on the actual adherence rate. Another possible factor is that we provided free medicines to the participating patients. In future studies, these factors need to be considered and carefully controlled.
Chotiyaputta et al4 suggested that the history of HBV treatment was not correlated with adherence. However, we found that new patients without a NUC treatment history showed better adherence rates than previously treated patients. This result is in agree with a report by Sevim et al24 who found that tuberculosis patients with a history of treatment had less adherence than new patients. Again, the variances between different studies may be explained by the different geographical and cultural background, the level of medical education, and the different experimental designs and strategies in different studies.
It has been suggested that adherence increases with increasing age25,26 and that the elderly (over 55 years old) might have higher adherence rates.3,4,9,27,28 In contrast, we found that age was not a factor affecting adherence to NUCs. Participating patients in our study had younger average age and smaller age range (17–56 years, with only one case over 55 years) than those of other studies that included larger numbers of elderly patients.4,9 Thus, it is possible that in our study, the age range is too small to reveal a difference in NUC adherence in different age groups.
In spite of the widely acknowledged notion that side effects are associated with nonadherence for many drugs,29,30 the four NUCs have minimal side effects and have similar adverse events records.13–16 Nevertheless, we found that lamivudine and entecavir were less adhered to than telbivudine. Therefore, the different adherence rates of different NUCs may not be attributable to their side effects. Our results partially agree with those of Chotiyaputta et al4 who showed that lamivudine was less adhered to than other NUCs. The mechanisms of this difference remain to be elucidated.
We report for the first time that a history of NUC resistance conferred better adherence. Thus, it appears that patients with previous NUC treatment are less adherent to NUCs in the absence of drug resistance, but are better adherent when resistance is developed. It should be mentioned that our data only show the influence of resistance to lamivudine on adherence. Whether resistance to other NUCs has a similar impact on adherence remains to be investigated.
Results are greatly diversified in studies of factors associated with NUC adherence. The diversity may be explained by the differences in experimental designs and strategies; different study population; different cultural, educational, and economic background; and different definitions of “good adherence rate.” Some studies used the most stringent method of pill counts to assess adherence and reported low adherence rate,3,4,8–10,12,31 while in other studies, physician assessment or patient self-reporting to health providers adopted less stringent methods and may have led to overestimation of adherence and inadequate recognition of poor adherence.4,7
Our study used a moderately stringent method. We found a less than perfect rate of adherence, and the assessment scores are less likely to be inflated. In addition, a study by Giang et al12 showed that NUC adherence is vulnerable to a variety of factors, such as forgetfulness, change of routine, being too busy, etc. Therefore, application of the results of NUC adherence investigations has certain geographical limitations and should be taken into consideration by doctors in different parts of the world. We did not collect disease severity data in this study. However, all of the patients had CHB and those with hepatic dysfunction, liver cirrhosis, and liver cancer were excluded. For determination of disease severity, the most objective standard is liver biopsy, and unfortunately, our patients did not have liver biopsy before treatment.
In conclusion, our data suggest that in the People’s Republic of China, female sex, no previous NUC treatment, and NUC resistance are factors associated with adherence to NUCs for CHB treatment. We report that CHB patients had better adherence to telbivudine than lamivudine and entecavir. To our knowledge, this is the first report to have investigated the factors associated with adherence to NUCs in CHB treatment in the People’s Republic of China, and the first to show NUC resistance as a factor associated with NUC adherence. Our findings should potentially benefit CHB patients’ through better control of adherence to NUCs and thus improve the treatment outcomes.
Conclusion
Key messages
- Optimal adherence to NUC medications is necessary to achieve undetectable levels of HBV DNA in patients with CHB and is necessary to prevent the sequelae of liver cirrhosis and hepatocellular carcinoma common in this disease.
- The factors associated with adherence to treatment regimens remain unclear.
- We found that adherent patients were more likely to be female and were more likely to be NUC-naïve.
- With approximately 400 million patients worldwide with CHB, it is important to understand the factors associated with medication adherence in order to be able to assist patients in improving their adherence rates.
Disclosure
The authors report no conflicts of interest in this work.
References
Kose S, Turken M, Cavdar G, Akkoclu G. The effectiveness of nucleoside analogues in chronic hepatitis B patients unresponsive to interferon therapy: our clinical trials for one year. Hepat Mon. 2010;10(4):289–293. | ||
Liang X, Bi S, Yang W, et al. Epidemiological serosurvey of hepatitis B in China – declining HBV prevalence due to hepatitis B vaccination. Vaccine. 2009;27(47):6550–6557. | ||
Chotiyaputta W, Peterson C, Ditah FA, Goodwin D, Lok AS. Persistence and adherence to nucleos(t)ide analogue treatment for chronic hepatitis B. J Hepatol. 2011;54(1):12–18. | ||
Chotiyaputta W, Hongthanakorn C, Oberhelman K, Fontana RJ, Licari T, Lok AS. Adherence to nucleos(t)ide analogues for chronic hepatitis B in clinical practice and correlation with virological breakthroughs. J Viral Hepat. 2012;19(3):205–212. | ||
Zhang QQ, An X, Liu YH, et al. Long-term nucleos(t)ide analogues therapy for adults with chronic hepatitis B reduces the risk of long-term complications: a meta-analysis. Virol J. 2011;8:72. | ||
Hongthanakorn C, Chotiyaputta W, Oberhelman K, et al. Virological breakthrough and resistance in patients with chronic hepatitis B receiving nucleos(t)ide analogues in clinical practice. Hepatology. 2011;53(6): 1854–1863. | ||
Ha NB, Ha NB, Garcia RT, et al. Medication nonadherence with long-term management of patients with hepatitis B e antigen-negative chronic hepatitis B. Dig Dis Sci. 2011;56(8):2423–2431. | ||
Lieveld FI, van Vlerken LG, Siersema PD, van Erpecum KJ. Patient adherence to antiviral treatment for chronic hepatitis B and C: a systematic review. Ann Hepatol. 2013;12(3):380–391. | ||
Berg AT, Berkovic SF, Brodie MJ, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia. 2010;51(4):676–685. | ||
Hilleret MN, Larrat S, Stanke-Labesque F, Leroy V. Does adherence to hepatitis B antiviral treatment correlate with virological response and risk of breakthrough? J Hepatol. 2011;55(6):1468–1469; author reply 1469. | ||
Sogni P, Carrieri MP, Fontaine H, et al. The role of adherence in virological suppression in patients receiving anti-HBV analogues. Antivir Ther. 2012;17(2):395–400. | ||
Giang L, Selinger CP, Lee AU. Evaluation of adherence to oral antiviral hepatitis B treatment using structured questionnaires. World J Hepatol. 2012;4(2):43–49. | ||
Khungar V, Han SH. A systematic review of side effects of nucleoside and nucleotide drugs used for treatment of chronic hepatitis B. Curr Hepatitis Rep. 2010;9(2):75–90. | ||
Liaw YF, Raptopoulou-Gigi M, Cheinquer H, et al. Efficacy and safety of entecavir versus adefovir in chronic hepatitis B patients with hepatic decompensation: a randomized, open-label study. Hepatology. 2011; 54(1):91–100. | ||
Su QM, Ye XG. Effects of telbivudine and entecavir for HBeAg-positive chronic hepatitis B: a meta-analysis. World J Gastroenterol. 2012; 18(43):6290–6301. | ||
Jiang H, Wang J, Zhao W. Lamivudine versus telbivudine in the treatment of chronic hepatitis B: a systematic review and meta-analysis. Eur J Clin Microbiol Infect Dis. 2013;32(1):11–18. | ||
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. | ||
Liang KY, Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73(1):13–22. | ||
Lai CL, Gane E, Liaw YF, et al; Globe Study Group. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med. 2007; 357(25):2576–2588. | ||
Wiens A, Lenzi L, Venson R, et al. Comparative efficacy of oral nucleoside or nucleotide analog monotherapy used in chronic hepatitis B: a mixed-treatment comparison meta-analysis. Pharmacotherapy. 2013; 33(2):144–151. | ||
Choi-Kwon S, Kwon SU, Kim JS. Compliance with risk factor modification: early-onset versus late-onset stroke patients. Eur Neurol. 2005; 54(4):204–211. | ||
Fodor GJ, Kotrec M, Bacskai K, et al. Is interview a reliable method to verify the compliance with antihypertensive therapy? An international central-European study. J Hypertens. 2005;23(6):1261–1266. | ||
Jin J, Sklar GE, Min Sen Oh V, Chuen Li S. Factors affecting therapeutic compliance: a review from the patient’s perspective. Ther Clin Risk Manag. 2008;4(1):269–286. | ||
Sevim T, Aksoy E, Ataç G, et al. Treatment adherence of 717 patients with tuberculosis in a social security system hospital in Istanbul, Turkey. Int J Tuberc Lung Dis. 2002;6(1):25–31. | ||
Caspard H, Chan AK, Walker AM. Compliance with a statin treatment in a usual-care setting: retrospective database analysis over 3 years after treatment initiation in health maintenance organization enrollees with dyslipidemia. Clin Ther. 2005;27(10):1639–1646. | ||
Lacasse Y, Archibald H, Ernst P, Boulet LP. Patterns and determinants of compliance with inhaled steroids in adults with asthma. Can Respir J. 2005;12(4):211–217. | ||
Senior V, Marteau TM, Weinman J; Genetic Risk Assessment for FH Trial (GRAFT) Study Group. Self-reported adherence to cholesterol-lowering medication in patients with familial hypercholesterolaemia: the role of illness perceptions. Cardiovasc Drugs Ther. 2004;18(6): 475–481. | ||
Hertz RP, Unger AN, Lustik MB. Adherence with pharmacotherapy for type 2 diabetes: a retrospective cohort study of adults with employer-sponsored health insurance. Clin Ther. 2005;27(7):1064–1073. | ||
Hovinga CA, Asato MR, Manjunath R, et al. Association of non-adherence to antiepileptic drugs and seizures, quality of life, and productivity: survey of patients with epilepsy and physicians. Epilepsy Behav. 2008;13(2):316–322. | ||
Ho PM, Bryson CL, Rumsfeld JS. Medication adherence: its importance in cardiovascular outcomes. Circulation. 2009;119(23):3028–3035. | ||
Leifeld J, Angers DA, Chenu C, Fuhrer J, Kätterer T, Powlson DS. Organic farming gives no climate change benefit through soil carbon sequestration. Proc Natl Acad Sci U S A. 2013;110(11):E984. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.