")
Back to Journals » Clinical Ophthalmology » Volume 9
Extensive superior limbic keratoconjunctivitis in Graves’ disease: case report and mini-review of the literature
Authors Chelala E, El Rami H, Dirani A , Fakhoury H, Fadlallah A
Received 19 December 2014
Accepted for publication 14 February 2015
Published 10 March 2015 Volume 2015:9 Pages 467—468
DOI https://doi.org/10.2147/OPTH.S79561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Elias Chelala, Hala El Rami, Ali Dirani, Henry Fakhoury, Ali Fadlallah
Faculty of Medicine, Saint-Joseph University, Beirut, Lebanon
Background: Superior limbic keratoconjunctivitis (SLK) is characterized as an inflammation of the superior bulbar conjunctiva with predominant involvement of the superior limbus and adjacent epithelial keratitis.
Methods: A 51-year-old woman, with a history of medically controlled Graves’ disease was seen with an extensive SLK involving 5 mm of the superior cornea.
Results: Total remission was observed with topical steroids (DXM). Recurrence was observed 1 week after steroid discontinuation, and steroidal treatment was reintroduced with tapering over 1 month. Total remission was then observed for 1 year.
Conclusion: Extensive keratitis and vascular pannus in SLK is rarely reported. This form could be treated with topical steroids. Tapering treatment remains essential for long-term success.
Keywords: superior limbic keratoconjunctivitis, anti-inflammatory drugs, dexamethasone, triamcinolone, Graves’ disease
Case report
A 51-year-old woman, with a history of well-controlled Graves’ disease, presented to the emergency department with pain in her right eye. Visual acuity was 20/30. The slit lamp examination showed superior conjunctival hyperemia with pannus involving 5 mm of the superior cornea (Figure 1). Staining with fluorescein dye was used to assess the lacrimal tear film. There was no superficial punctate keratitis, and breakup time was moderately reduced. There were no corneal filaments, and there was no papillary hypertrophy of the tarsal conjunctiva upon eversion of the superior eyelid. Intraocular pressure (IOP) was 12 mmHg. A diagnosis of right superior limbic keratoconjunctivitis (SLK) was made, and a treatment including topical steroids (dexamethasone, 1 mg/mL qid for 1 week, then tid) and preservative-free artificial tears (qid) was started. At the two-week follow-up visit, the patient was asymptomatic, and we observed a notable regression of the superior hyperemia and pannus. IOP was 15 mmHg. Steroids were tapered over a period of 1 week. One week after steroid discontinuation, the patient complained of pain and redness in her right eye. We noted a recurrence of the superior hyperemia and pannus on slit lamp examination. There was no superficial punctate keratitis, no corneal filaments and no papillary reaction. IOP was 17 mmHg. Topical steroids (dexamethasone 1 mg/mL) were reintroduced, with tapering over 1 month. No significant rise in IOP was noted during follow-up. The patient was kept on preservative-free artificial tears as needed and remained free of symptoms and signs for the following year.
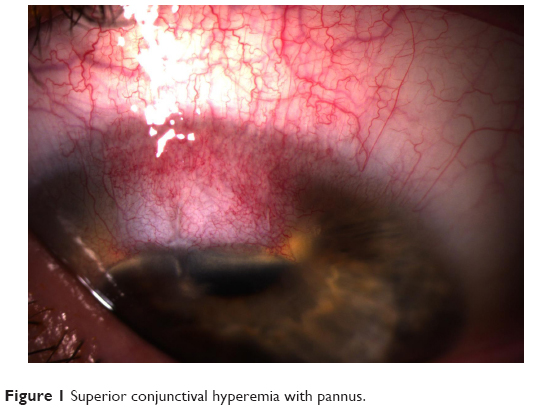 | Figure 1 Superior conjunctival hyperemia with pannus. |
Discussion
SLK is an inflammatory disorder of the superior bulbar and palpebral conjunctiva causing mild to moderate burning sensations, redness, and discharge. On slit lamp examination, the classical, usually bilateral, triad of clinical signs was first described by Theodore and included:1
- Papillary reaction of the superior palpebral conjunctiva
- Superior bulbar conjunctival hyperemia
- Superior superficial punctate keratoconjunctivitis.
The presence of associated corneal filaments and corneal pannus can also be found on examination.1
Mechanical factors such as the oculopalpebral asynergy found in Graves’ disease result in abnormal rubbing between the palpebral and the bulbar conjunctiva which causes chronic inflammation and SLK. Permanent superior conjunctivochalasis can develop and aggravate the mechanical disturbance.2,3 In advanced cases, superior limbal stem cell deficiency syndrome may occur from the repeated microtrauma to the limbal stem cells.
Topical anti-inflammatory drugs such as steroids relieve the inflammation and may result in long-term improvement. When eyedrops fail, supratarsal injections of triamcinolone may be considered.4 Topical lubricants are also an important asset to the medical management as they rehydrate and smoothen the ocular surface. Regular application of silver nitrate to the superior conjunctiva may also be considered.1 However, when conservative measures fail, surgical procedures that aim to restore a normal interaction between the palpebral and the bulbar conjunctiva might succeed. For instance, superior conjunctival resection is considered when there is a prominently lax superior conjunctiva as well as blepharoplasty and/or surgical correction of proptosis in Graves’ disease.5–7 In our case, no significant chalasis was found and proptosis was mild. Thus, sustained improvement was obtained with medical treatment alone.
Finally, it is important to keep in mind that at least one-third of SLK cases are linked to thyroid orbitopathy and that a well-controlled thyroid disease greatly improves the clinical manifestations of SLK.1
Disclosure
The authors report no conflicts of interest in this work.
References
Nelson JD. Superior limbic keratoconjunctivitis (SLK). Eye. 1989;3(Pt 2):180–189. | ||
Wilson FM II, Ostler HB. Superior limbic keratoconjunctivitis. Int Ophthalmol Clin. 1986;26:99–112. | ||
Cher I. Superior limbic keratoconjunctivitis: multifactorial mechanical pathogenesis. Clin Exp Ophthalmol. 2000;28:181–184. | ||
Shen YC, Wang CY, Tsai HY, Lee YF. Supratarsal triamcinolone injection in the treatment of superior limbic keratoconjunctivitis. Cornea. 2007;26(4):423–426. | ||
Passons GA, Wood TO. Conjunctival resection for supcrior limbic keratoconjunctivitis. Ophthalmology. 1986;91:966–968. | ||
Yokoi N, Komuro A, Maruyama K, Tsuzuki M, Miyajima S, Kinoshita S. New surgical treatment for superior limbic keratoconjunctivitis and its association with conjunctivochalasis. Am J Ophthalmol. 2003;135(3):303–308. | ||
Kadrmas EF, Bartley GB. Superior limbic keratoconjunctivitis: a prognostic sign for severe Graves ophthalmopathy. Ophthalmology. 1995;102(10):1472–1475. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.