")
Back to Journals » Open Access Emergency Medicine » Volume 7
Emergency department ultrasound probe infection control: challenges and solutions
Authors Shokoohi H, Armstrong P, Tansek R
Received 28 June 2014
Accepted for publication 5 September 2014
Published 5 January 2015 Volume 2015:7 Pages 1—9
DOI https://doi.org/10.2147/OAEM.S50360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hans-Christoph Pape
Hamid Shokoohi, Paige Armstrong, Ryan Tansek
Department of Emergency Medicine, George Washington University Medical Center, Washington DC, USA
Abstract: Point-of-care ultrasound (US) has become a cornerstone in the diagnosis and treatment of patients in the emergency department (ED). Despite the beneficial impact on patient care, concern exists over repeat use of probes and the role as a vector for pathogen transmission. US probes are used for various applications, with the level of infection risk, based on the Spaulding Classification, ranging from noncritical with common practice to semicritical with endocavitary probes. To date, the most closely studied organisms are Staphylococcus aureus and human papilloma virus. Current evidence does confirm probe colonization but has not established a causative role in human infection. Based on current literature, US use during invasive procedures remains an infection control concern, but routine use on intact skin does not appear to cause significant risk to patients. Various barrier methods are available, each with indications based on extent of procedure and likelihood of contact with mucosal surfaces. Additionally, chemical cleansing methods have been shown to be effective in limiting probe contamination after use. New technologies utilizing ultraviolet light are available and effective but not widely used in the ED setting. As our understanding of the critical factors in US probe cleaning and disinfection improves, it is important to assess the challenges found in our current practice and to identify potential solutions to improve practices and procedures in infection control across the spectrum of US probe use in various applications in the ED. This article serves as a summary of the current literature available on infection control topics with the utilization of point-of-care US, and discusses challenges and potential solutions to improve the current practice of probe-related infection control.
Keywords: ultrasound probe, Staphylococcus aureus, disinfection, infection risk, endocavitary probe, human papilloma virus
Introduction
The use of point-of-care ultrasound (US) has become increasingly integrated into the diagnosis and management of patients presenting to the emergency department (ED). Initially accepted for its role in evaluating patients with trauma and procedural guidance, it is now regularly used in the evaluation of most organ systems and various different conditions.1 US also remains fundamental in the performance of several procedures completed in the ED. The use of US as a readily available adjunct has not only improved the quality of patient care but also led to more expeditious management.
Despite acceptance within the emergency medicine community, the risks of use may not be fully understood. As with every piece of equipment used for patient care, we must be diligent in our evaluation and understanding of the hazards associated with its use, and ensure that we are not harming the patient through spread of infection. US probes, machines, conductive gel, and also providers stand to be vehicles for transmission. US probes are in constant use in the ED, with a high potential for infection transmission between patients. These US probes are used for various applications, with infection classification risks ranging from noncritical with common practice uses of US to semicritical risk with endocavitary US probes.
There have been many improvements and innovative practices in recent years, but there remains a substantial need to better understand the clinical importance and magnitude of infection risk related to the common practice of using US for different applications in the ED. This article focuses on the common infectious risks with US use, the effectiveness of current disinfectants, and the evolving technological advances. We describe important elements of probe cleaning and disinfection, and discuss challenges and potential solutions to improve the current practice of probe-related infection control.
Types of probes and common uses
Several types of US probes are used in the ED setting, each with properties that make them more desirable for certain uses. Common applications of bedside US for both diagnostic purposes and US-guided procedures in the ED are listed in Table 1. The four most often used probes are linear, curvilinear, phased array, and endocavitary.
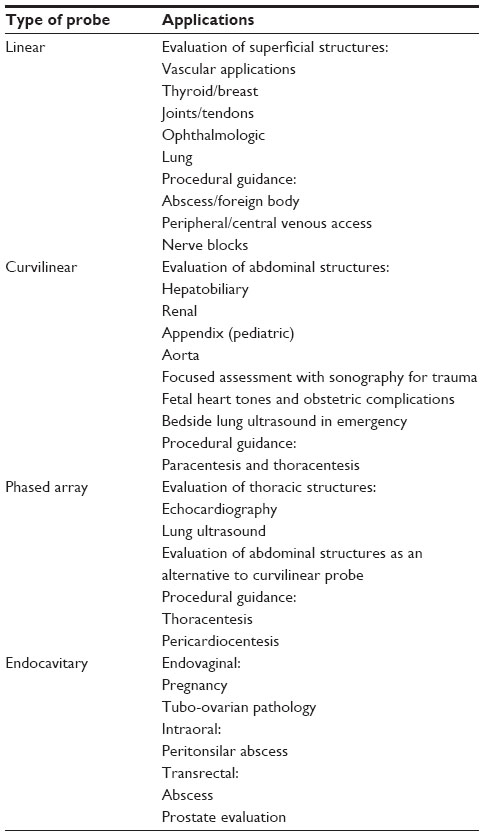 | Table 1 Types of ultrasound probes and their point-of-care ultrasound applications in the emergency department |
Linear probes, also referred to as straight probes, operate with a higher frequency and create high-resolution images of structures near the body surface. This makes the probe ideal for US evaluations of soft tissue, superficial vasculature, tendons, and ophthalmological applications. Specifically, when performing US-guided peripheral or central venous access, linear probes offer superior visualization of vessels and surrounding structures. Linear probes may also be used for superficial abscess drainage, foreign body removal, and joint effusion aspiration. Some ultrasonographers choose linear probes for lung US and assistance with thoracenteses in patients with limited subcutaneous tissue volume.
For deep structures, particularly intra-abdominal, curvilinear probes produce better-quality images. The curvilinear probes use lower-frequency waves, providing deeper penetration and a wider depth of field, ideal for viewing intra-abdominal structures. These are routinely used for focused assessment with sonography in trauma and evaluation of the aorta, gallbladder, kidneys, and uterus. Curvilinear probes can also be helpful in lung evaluation and US-guided thoracentesis and paracentesis.
Many institutions use the phased array or sector probe in a similar fashion to the curvilinear probe, and for the purposes of infection control, they can be grouped together. This probe is commonly used for echocardiography, chest US, and even abdominal US. It provides a broad depth of field with a small footprint, allowing the sonographer to view deep structures though a small acoustic window, such as between the ribs.
Endocavitary probes are used less frequently in the ED but do afford advantages for specific studies. The wand-shaped design of this type of probe allows for examination of body cavities such as the oropharynx, female pelvic organs, and the male prostate. Pelvic pathology may not be evident on transabdominal examination, and internal evaluation provides superior visualization of pelvic structures and fetus assessment in early pregnancy. Endocavitary probes can also help guide procedures such as drainage of peritonsilar abscesses.
Isolates and pathogens of concern in the ED
Extensive efforts are made to reduce infection transmission both in the ED and throughout the health care industry. This becomes of particular significance when considering a diagnostic tool that is used repeatedly and for interventions ranging from central vascular access to drainage of pustulant material. There are particular isolates of heightened concern due to prevalence and the possibility of increased morbidity and mortality in patients.2 The more commonly evaluated pathogens are methicillin-resistant Staphylococcus aureus (MRSA) and human papilloma virus (HPV). Both of these organisms are prevalent in the community and their transmission would have significant impact on patients.
The spread of both community- and hospital-acquired MRSA has been the topic of substantial research efforts.2 Since abscesses often require US evaluation and subsequent incision and drainage, the concern exists that this practice may contribute to the spread of MRSA infection with a high potential for probe contamination. It has been suggested that both probes and transmission gel are potential vectors for S. aureus, both methicillin-sensitive and methicillin-resistant. The literature on this topic is not conclusive, and rates of measured MRSA probe contamination vary widely; however, it is generally proposed that MRSA spread by US probe is unlikely (Table 2).3–6One observational study sampled eleven probes on ten separate occasions. Even when probes appeared grossly soiled, of the 110 samples collected, there were no cultures positive for MRSA.6
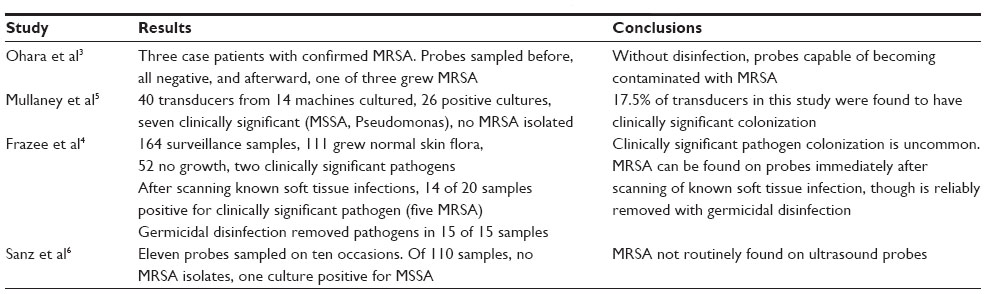 | Table 2 Studies on ultrasound probe contamination with MRSA in the emergency department |
Furthermore, attention has been given to the shear prevalence of MRSA on surfaces in the ED. Of 40 samples taken from inanimate objects in an urban ED, only one grew MRSA. The one positive sample came from the security pad on a doorway, an area unlikely to be cleaned as regularly as patient care areas.7 Other elements of the US machine also stand to become contaminated, leading to cross-infection; these include the keyboard, control settings, cords, and even documentation sites.4 One can hypothesize that in a fast-paced environment, with the US machine passing from one room to the next, it is unlikely that the operator will disinfect the entire device. With low prevalence of infectious pathogens both throughout the ED and specifically on US machines, it stands to reason that the risk of spreading MRSA is low.
Another infectious agent heavily studied in relation to US transmission is HPV. Infection confers potential lifelong morbidity and even possible mortality, especially in the immunocompromised. It has been shown that despite appropriate cleaning measures, endocavitary probes pose risk of contamination.8,9 In a study of endocavitary probe surveillance, 120 samples were obtained, revealing nine (7.5%) positive for HPV deoxyribonucleic acid (DNA).9 Pooled meta-analyses have also shown that endocavitary probes can remain contaminated with viruses, including herpes simplex virus, HPV, and cytomegalovirus, as well as pathogenic bacteria.10 These studies have failed to establish a direct relationship to transmission and resultant infection.
While MRSA and HPV contamination have been the focus of many surveillance studies, there are many other clinically significant bacterial pathogens. For instance, multidrug-resistant organisms such as extended spectrum beta-lactamase Escherichia coli or carbapenemase-producing Klebsiella pneumoniae would also be of great interest. Transmission of these aggressive and virulent bacteria could carry significant morbidity and mortality. At this time, there is minimal data studying this group of pathogens specifically in regards to transmission via ultrasonography.
Management of infection control with US probes
Guidelines and infection control policy
The Centers for Disease Control and Prevention (CDC) and the Healthcare Infection Control Practices Advisory Committee offer guidelines and recommendations on the disinfection of patient care equipment. More recently, the American Institute of Ultrasound in Medicine (AIUM) adopted and approved similar guidelines. The majority of these guidelines employ a similar rational approach to disinfection and sterilization of patient care items and equipment as suggested by Earle H Spaulding more than 30 years ago.2 This classification scheme is a logical approach that has been retained, refined, and successfully used for the purpose of infection control.
The Spaulding Classification
The Spaulding Classification system is a widely accepted practice standard designed to help determine the risk of infection from, and degree of disinfection required for, various medical devices. This classification system has three categorizations: critical, semicritical, and noncritical (Table 3).2
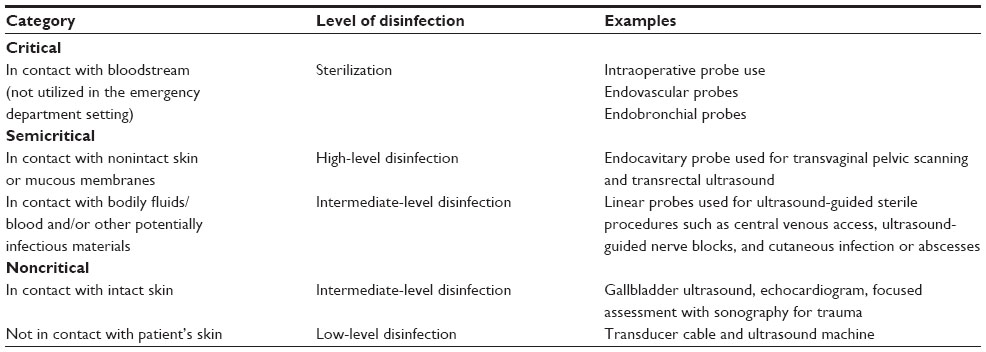 | Table 3 The Spaulding Classification for disinfection of ultrasound probes and equipment |
A device that enters normally sterile tissue or the vascular system through which blood flows are classified as critical. Endovascular probes and intraoperative use of transducer are among examples in this category. Such devices should be sterilized, which is defined as the destruction of all microbial life.
Devices that come into contact with nonintact skin or mucous membranes and do not ordinarily penetrate sterile tissue are categorized as semicritical instruments. Endocavitary US probes (vaginal, rectal, and intraoral) are some examples of this category. The cleaning process must achieve a high level of disinfection, which is defined as the destruction of all vegetative microorganisms, mycobacterium, small or nonlipid viruses, medium or lipid viruses, fungal spores, and some bacterial spores.
Noncritical devices are those that do not ordinarily come into contact with a patient or interface with only intact skin. These devices should be cleaned by low-level disinfection techniques.11 Low-level disinfection eliminates some viruses and bacteria, typically through use of a chemical germicidal agent, registered as a hospital disinfectant by the United States Environmental Protection Agency (EPA). Based upon common practice and the AIUM recommendations, noncritical devices should be cleaned with either water or a germicidal detergent such as a quaternary ammonium spray or wipe (low-level disinfectant) after each use.12 And whereas it might be ideal from a purely infection control standpoint to consistently use high-level disinfectants, this practice may cause equipment deterioration as well as chemical exposure to patients and practitioners.13
The Spaulding Classification also acknowledges a level of disinfection not available in routine practice: intermediate-level disinfection. While this classification is helpful in a conceptual sense, we do not currently practice this level of cleansing. Consequently, any probe used in a semicritical way requires high-level disinfection, and those used in a noncritical manner receive low-level disinfection.
Current methods of infection control
Barrier methods utilized
Cleansing with disinfectants attempts to limit colonization and subsequent transmission. Though it has been shown that the presence of clinically significant microbes is uncommon, barrier methods provide an additional level of protection to prevent pathogen spread (Table 4). In some instances, adhesive barriers such as Tegaderm© are placed over the end of the US probe as a makeshift barrier. This is particularly common when the probe is being used in a way that confers only a slightly higher risk of infection transmission, such as peripheral venous access or ophthalmologic examination. This method has not been adequately studied to determine if it confers any benefit.
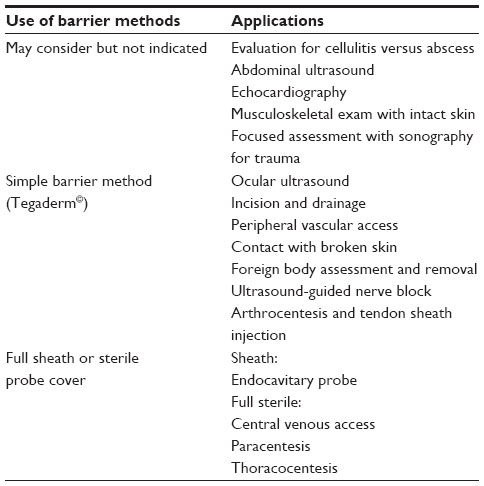 | Table 4 Use of barrier methods for various ultrasound examinations |
Probe cover and sheath
Probe covers or condoms are consistently used during evaluation with the endocavitary probe, particularly because these evaluations permit contact with mucosal surfaces. These barriers fit tightly over the probe tip and are extended over the entire wand-like projection of the probe. Given common use for oropharyngeal, vaginal, and rectal exam, it remains standard of care to use a mechanical barrier to prevent spread. Pathogens of particular concern for transmission are HPV, herpes simplex virus, and other sexually transmitted infections known to be passed through contact with mucosal surfaces. Blood-borne pathogens can also contaminate US probes, especially if biopsy or incision and drainage is occurring. And, as with many barrier methods, the cover may tear during exam or procedure, increasing the risk of probe contamination.14,15 Barrier methods have been shown to be effective in preventing further probe contamination.16 When used in conjunction with disinfection, low rates of clinically significant colonization have been reported. In a study performed specifically evaluating a standard probe condom cover, 0.9% were found to have perforated upon visual inspection, none showed small perforations after being filled with water, and, through swab samples, only one was suggested to have a microperforation allowing bacterial translocation.15
Full sterile
Sterile covers should be used during invasive US-guided procedures: eg, the placement of a US-guided central venous catheter or thoracentesis. Sterile US conduction gel is also available for these procedures and should be used consistently for them.
In patients with latex allergy, prior to the use of a transducer cover, specific inquiry should be directed to the patient, and, if appropriate, special nonlatex covers may need to be utilized.
Cleansing methods, effectiveness, and targeted organisms
Manual cleaning is an essential prerequisite for all effective disinfection processes. All the gel and residues from previous scans should be removed from the transducer. The current protocols propose that standard household-type detergents and soaps are not a recommended cleaner due to their high foaming properties, which increases the residue left behind and decreases the effectiveness of the cleaning. The transducer must be thoroughly cleaned and then dried with a soft, disposable towel.17
Several methods have been developed for the cleansing of US equipment after patient use. The most prevalent in EDs are those requiring mechanical cleansing. Additional methods exist, such as ultraviolet (UV) light or other automated disinfecting technologies. There is debate in the literature regarding what method for cleaning the probes is best; however, the provider can be best guided by recommendations such as those published by the AIUM.18,19
Several types of compounds have been used to disinfect US probes. These are frequently divided into low-level and high-level disinfectants. Low-level disinfectants include chemicals such as quaternary ammonium compounds and phenolics. These solutions can be found in a variety of delivery methods such as sprays and wipes, but the chemical composition remains the same. A common product available in many EDs is the Sani-Cloth; the active ingredient in these wipes is a quaternary ammonium. These are not effective against nonenveloped viruses, fungi, or bacterial spores. High-level disinfectants include hydrogen peroxide, glutaraldehyde, and peracetic acid. Often, this may be in the form of a soak, spray, or wipes. These disinfectants do eliminate nonenveloped viruses.11
As mentioned earlier, the CDC determines which disinfectant is deemed standard of use based upon the medical equipment classification system.11 The routine cleansing of US equipment after patient use reduces contamination by clinically significant pathogens.5,20 Germicidal wipes containing quaternary ammonia have been shown to be effective at reducing contamination after US examination of skin and soft tissue infections.21 Some have argued for the use of simpler cleansing methods, such as the use of dry paper wipes or saline and soap.22,23 While basic gross decontamination may remove contaminants, only germicidal products confer bacteriocidal benefits even after decontamination.5 For instance, low-level disinfectants may not be sufficient for probes used in high-risk settings, even when probe covers are employed. A French study evaluated endovaginal probes after removal of barrier protection and subsequent disinfection with quaternary ammonium and chlorhexidine.13 In sample sets of 100, HPV DNA remained on 13% of probes, Chlamydia trachomatis DNA on 20% of probes, and mycoplasma DNA on 8% of probes. Samples were also analyzed using nuclease treatment to determine what portion of positive samples had the potential to be virulent to human cells. The percent of pathogens that remained actively infectious was 7% for HPV, 2% for C. trachomatis, and 4% for mycoplasma. Again, research confirms that colonization is present on US probes, even when current cleansing methods are enacted; however, confirmation of transmission from one patient to another has not been firmly established.13
Alcohol-based disinfectants
The use of alcohol-based disinfectants including 70% isopropyl alcohol (rubbing alcohol) is not recommended for the disinfection of transducers due to the potential of drying out and destroying the rubber head transducers.24 Since alcohol swabs are commonplace in the ED, it is important that we relay this critical information to staff so as to prevent irreparable damage to these expensive pieces of equipment. The only parts that may be cleaned with isopropyl alcohol are the connector and transducer housing and the US machine and stand. Often, US manufacturers restrict use of alcohol-based wipes on any part of a transducer, as they can damage the sensitive parts of the transducer and often the damage is not covered by the limited warranty on devices.
The use of a multipurpose spray cleaner containing isopropyl alcohol, chlorhexidine gluconate, and a mild wetting agent, such as Transeptic® Cleansing Solution (T-spray, T-spray II), has not been restricted by some of the US manufacturers. We strongly recommend referring to the manufacturers’ recommendations for their appropriate use.
High-level disinfection for endocavitary probes
The CDC and the AIUM recommend high-level disinfection even for covered endocavitary probes.11,12 Multiple US Food and Drug Administration (FDA)-approved methods achieve high-level disinfection between patients for these probes. High-level disinfection technologies consist of immersion of the US probes in glutaraldehyde, hydrogen peroxide, or peracetic acid and then rinsing and drying. Manual chemical immersion of probes with a glutaraldehyde-based solution (Cidex; CIVCO Medical Solutions, Kalona, IA, USA) is a widely practiced method. This method, although effective, is logistically difficult, time-consuming, and involves several steps and quality control measures. Newer FDA-approved methods such as the Trophon system (Nanosonics, Alexandria, New South Wales, Australia) and other alternatives such as UV-C light disinfectant and gas plasma systems can be utilized for this purpose.
AIUM guidelines for cleaning and preparing endocavitary probes
The most recent AIUM guidelines (approved 4/2/2014) suggest that endocavitary probes should be cleansed and disinfected meticulously as per the following steps.12
Cleaning
- Cleaning probe immediately by using a soft brush with nonabrasive detergent
- Rinsing the probe with tap water and dry it with cloth/towel or air dry
- Visually inspect entire transducer to make sure that it is clean
- The use of sheathes does not change the type of processing that is recommended for the transducer, due to the potential for breakage of the probe covers.
Disinfection
High-level disinfection is recommended by soaking the probe in a high-level disinfectant or hydrogen peroxide gas plasma or vaporized hydrogen peroxide. Examples of such high-level disinfectants include but are not limited to:
- 2.4%–3.2% glutaraldehyde products (a variety of available proprietary products, including Cidex, Metricide, and Procide)
- Nonglutaraldehyde agents, including Cidex OPA (o-phthalaldehyde) and Cidex PA (hydrogen peroxide and peroxyacetic acid)
- 7.5% hydrogen peroxide solution
- Common household bleach (5.25% sodium hypochlorite) diluted to yield 500 parts per million chlorine (10 cc in 1 liter of tap water). This agent is effective but generally not recommended by US probe manufacturers because it can damage metal and plastic parts.
A complete list of FDA-cleared liquid sterilants and high-level disinfectants is available at http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm194429.htm.
In addition to traditional cleaning of US equipment, new technologies are providing further possibilities (Table 5). Automated disinfecting devices have shown promise in not only reducing pathogen burden but also limiting human exposure to potentially toxic cleansing products.19 UV light is another promising alternative for US equipment sterilization.18,26 However, these new techniques convey higher costs and are not routinely available in most EDs at this time.
 | Table 5 Examples of cleansing methods |
Challenges and solutions
Variety in recommendations
US probe manufacturers have widely varying recommendations for cleaning and disinfection. This is, in large part, due to the lack of clinically based standards for the testing of disinfectant chemicals and assessment of compatibility with probes. In addition, the manufacturer recommendations can be driven by the minimal requirements for commercialization or a financial relationship with another manufacturer. This loose guidance creates obstacles for institutions and practices attempting to implement protocols. Furthermore, attempting to comply with a wide range of recommendations can prove costly and difficult to regulate. Infection control efforts should therefore focus on the current CDC and AIUM guidelines and aim to create a standard of practice within the particular institution.11,12 Defining codes that are unifying can combat this confusion and be the basis for more widespread standardization.
Despite efforts to categorize different probes with a unifying classification system, there remains ambiguity with regard to which disinfectant is indicated. This is, at least in part, due to the fact that the same probe may be used in a variety of capacities. For example, the curvilinear probe can be used for both gallbladder evaluation as well as paracentesis. While there is the potential for confusion, the provider should rely on the invasiveness of the procedure to dictate the cleansing method employed. In general, applying a higher level of disinfection is preferred. Additionally, adopting common practices from other similar organizations and collaborative efforts to define the magnitude of risk and appropriate preventive measures are essential.11,12,27
Education and training
Medical providers and trainees who use, clean, and disinfect US probes may not be uniformly trained in the necessary procedures. It is imperative that all personnel who have access to US equipment receive sufficient training in equipment cleaning and disinfection. Providing this training in the ED setting, which tends to have high provider turnover, might be cumbersome. At a minimum, infection control training should be provided upon initial orientation and then with subsequent annual refreshers. Applying manufactured approved disinfectants and cleaning products can improve the safety of the transducer and may help avoid warranty-related issues or equipment damage. Note that alcohol is not an EPA-registered detergent/disinfectant, nor is it recommended by manufacturers.24,28,29
Endocavitary probes disinfection challenges
There are no consensus guidelines for transvaginal probe disinfection among health authorities and institutions. Endocavitary probe use conveys the added risk of infections commonly transmitted by genital secretions, including human immunodeficiency virus, hepatitis B virus, Neisseria gonorrhoea, C. trachomatis, Trichomonas vaginalis, and HPV. These organisms can remain infectious for days outside of the body, particularly if kept moist in blood or serum.
Currently, the CDC and the AIUM recommend a high-level disinfection for endovaginal probes between patients, although high-level disinfection practices are costly, time-consuming, and may pose health risks to patients and practitioners and damage transducers. Therefore, as a consequence, current practice compliance with this standard is poorly followed. While additional methods such as UV-C light and gas plasma systems are being developed, they must be FDA-approved and confirmed by manufacturers as appropriate for use, thus often delaying access. Currently, regulatory approval is based on efficacy of products under conditions that may not be reasonably found in ED settings. More novel options, such as UV disinfectants and methods that may be effective and efficient in ED settings, are needed; however, none is readily available or practical for ED use at this time.12,30
Coupling gel contamination
Regardless of the method of probe disinfection, there is the added concern of US conduction gel contamination. It remains unclear as to how often US gel contamination may be attributable to the manufacturer compared with the practitioner.31 If, in fact, contamination occurs at the level of production, the commonplace room temperature storage can allow for added bacterial growth. However, most recent studies have failed to show the growth of pathogenic organisms, including MRSA or other notable pathogens, when sampling coupling gel.32,33
Conclusion
In this article, we have discussed the common practices and challenges associated with US probe infection control. As ED physicians continue to become more proficient in the use of US, we must consider the implications of a nondisposable piece of equipment. Current literature is progressive in establishing colonization and even contamination of probes after use. While many of the barrier methods are thought to be adequate for sterile procedures, it is clear that even microperforations can allow for bacteria to enter a very sensitive field. This becomes of particular importance in the case of central venous access, where extensive efforts have already been taken to reduce line infections. Chemical disinfectant measures are necessary and can be very effective; however, they must be considered in the context of probe damage and potential exposure to subsequent patients and providers. For this reason, equipment classifications systems have been established to guide their use and disinfection based on critical and noncritical uses. New techniques such as gas and UV decontamination are promising, though expensive, and may not be applicable to the ED setting in the near future. However, the literature still lags in the clinical significance of bacterial colonization and transmission.
Acknowledgment
The authors would like to sincerely thank Dr Keith Boniface and Dr Ali Pourmand for their guidance, and preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Jain A, Stead L, Decker W. Ultrasound in emergency medicine: a colorful future in black and white. Int J Emerg Med. 2008;1(4):251–252. | |
Favero MS, Bond WW. Disinfection of medical and surgical materials. In: Block SS, editor. Disinfection, Sterilization, and Preservation. Philadelphia, PA: Lippincott Williams & Wilkins; 2001:881–917. | |
Ohara T, Itoh Y, Itoh K. Ultrasound instruments as possible vectors of staphylococcal infection. J Hosp Infect. 1998;40(1):73–77. | |
Frazee BW, Fahimi J, Lambert L, Nagdev A. Bacterial growth on ED ultrasound machines. Ann Emerg Med. 2011;58(1):56–63. | |
Mullaney PJ, Munthali P, Vlachou P, Jenkins D, Rathod A, Entwisle J. How clean is your probe? Microbiological assessment of ultrasound transducers in routine clinical use, and cost-effective ways to reduce contamination. Clin Radiol. 2007;62(7):694–698. | |
Sanz GE, Theoret J, Liao MM, Erickson C, Kendall JL. Bacterial contamination and cleanliness of emergency department ultrasound probes. CJEM. 2011;13(6):384–389. | |
Kei J, Richards JR. The Prevalence of methicillin-resistant staphylococcus aureus on inanimate objects in an urban emergency department. J Emerg Med. 2011;41(2):124–127. | |
Casalegno JS, Le Bail Carval K, Eibach D, et al. High risk HPV contamination of endocavity vaginal ultrasound probes: an underestimated route of nosocomial infection? PLoS One. 2012;7(10):e48137. | |
Ma ST, Yeung AC, Chan PK, Graham CA. Transvaginal ultrasound probe contamination by the human papillomavirus in the emergency department. Emerg Med J. 2013;30(6):472–475. | |
Leroy S. Infectious risk of endovaginal and transrectal ultrasonography: systematic review and meta-analysis. J Hosp Infect. 2013;83(2):99–106. | |
Centers for Disease Control and Prevention. Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008. Available from: http://www.cdc.gov/hicpac/pdf/guidelines/Disinfection_Nov_2008.pdf. Accessed September 15, 2014. | |
American Institute of Ultrasound in Medicine. Guidelines for cleaning and preparing external- and internal-use ultrasound probes between patients [webpage on the Internet]. 2014. Available from: http://www.aium.org/officialStatements/57. Accessed September 15, 2014. | |
M’Zali F, Bounizra C, Leroy S, Mekki Y, Quentin-Noury C, Kann M. Persistence of microbial contamination on transvaginal ultrasound probes despite low-level disinfection procedure. PLoS One. 2014;9(4):e93368. | |
Masood J, Voulgaris S, Awogu O, Younis C, Ball AJ, Carr TW. Condom perforation during transrectal ultrasound guided (TRUS) prostate biopsies: a potential infection risk. Int Urol Nephrol. 2007;39(4):1121–1124. | |
Milki AA, Fisch JD. Vaginal ultrasound probe cover leakage: implications for patient care. Fertil Steril. 1998;69(3):409–411. | |
Amis S, Ruddy M, Kibbler CC, Economides DL, MacLean AB. Assessment of condoms as probe covers for transvaginal sonography. J Clin Ultrasound. 2000;28(6):295–298. | |
Australasian Society for Ultrasound in Medicine. Promoting Excellence in Ultrasound Policies and Statements B2 Statement on the Disinfection of Transducers. 2011. Available from: http://www.nanosonics.com.au/_literature_85273/Regulatory_Update_-_Promoting_Excellence_in_Ultrasound. Accessed September 15, 2014. | |
Bloc S, Mercadal L, Garnier T, et al. Evaluation of a new disinfection method for ultrasound probes used for regional anesthesia ultraviolet C light. J Ultrasound Med. 2011;30(6):785–788. | |
Bloc S, Garnier T, Bounhiol C, et al. Ultrasound guided regional anaesthesia: an effective method for cleaning the probes. Ann Fr Anesth Reanim. 2008;27(12):994–998. | |
Bello TO, Taiwo SS, Oparinde DP, Hassan WO, Amure JO. Risk of nosocomial bacteria transmission: evaluation of cleaning methods of probes used for routine ultrasonography. West Afr J Med. 2005;24(2):167–170. | |
Frazee BW, Fahimi J, Lambert L, Nagdev A. Emergency department ultrasonographic probe contamination and experimental model of probe disinfection. Ann Emerg Med. 2011;58(1):56–63. | |
Muradali D, Gold WL, Phillips A, Wilson S. Can ultrasound probes and coupling gel be a source of nosocomial infection in patients undergoing sonography? An in vivo and in vitro study. AJR Am J Roentgenol. 1995;164(6):1521–1524. | |
Mirza WA, Imam SH, Kharal MS, et al. Cleaning methods for ultrasound probes. J Coll Physicians Surg Pak. 2008;18(5):286–289. | |
Koibuchi H, Fujii Y, Kotani K, et al. Degradation of ultrasound probes caused by disinfection with alcohol. J Med Ultrason. 2011;38: 97–100. | |
Vickery K, Gorgis VZ, Burdach J, Patel D. Evaluation of an automated high-level disinfection technology for ultrasound transducers. J Infect Public Health. 2014;7(2):153–160. | |
Kac G, Gueneret M, Rodi A, et al. Evaluation of a new disinfection procedure for ultrasound probes using ultraviolet light. J Hosp Infect. 2007;65(2):163–168. | |
Ontario Agency for Health Protection and Promotion (Public Health Ontario). Provincial Infectious Diseases Advisory Committee. Best Practices for Cleaning, Disinfection and Sterilization of Medical Equipment/Devices. 3rd ed. Toronto, ON: Queen’s Printer for Ontario; 2013. | |
Sonosite, Inc. Disinfectants for SonoSite Products. 2011. Available from: http://www.sonosite.com/sites/default/files/support_docs/Disinfectants_ENG_P06703-08A_e.pdf. Accessed September 15, 2014. | |
General Electric Company. GE Healthcare. GE Transducer Cleaning and Disinfection Guidelines. 2013. Available from: http://www3.gehealthcare.com/static/ge-transducers/GEHC-Guidelines-Transducer_Cleaning_Disinfection_Guidelines.pdf. Accessed on June 20, 2014. | |
Kac G, Podglajen I, Si-Mohamed A, Rodi A, Grataloup C, Meyer G. Evaluation of ultraviolet C for disinfection of endocavitary ultrasound transducers persistently contaminated despite probe covers. Infect Control Hosp Epidemiol. 2010;31(2):165–170. | |
Provenzano DA, Liebert MA, Steen B, Lovetro D, Somers DL. Investigation of current infection-control practices for ultrasound coupling gel. Reg Anesth Pain Med. 2013;38(5):415–424. | |
Ejtehadi F, Ejtehadi F, Teb JC, Arasteh MM. A safe and practical decontamination method to reduce the risk of bacterial colonization of ultrasound transducers. J Clin Ultrasound. 2014;42(7):395–398. | |
Lawrence MW, Blanks J, Ayala R, et al. Hospital-wide survey of bacterial contamination of point-of-care ultrasound probes and coupling gel. J Ultrasound Med. 2014;33(3):457. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.