")
Back to Journals » Drug Design, Development and Therapy » Volume 9
Efficacy and safety of different doses of a slow-release corticosteroid implant for macular edema: meta-analysis of randomized controlled trials
Authors Liu Q , He M, Shi H, Wang Q, Du Y, Liu J, Ren C, Xu D, Yu J
Received 15 February 2015
Accepted for publication 13 March 2015
Published 5 May 2015 Volume 2015:9 Pages 2527—2535
DOI https://doi.org/10.2147/DDDT.S82929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Shu-Feng Zhou
Qingyu Liu,1,2,* Mengmei He,1,2,* Hui Shi,1,3 Qianyi Wang,1,2 Yaru Du,1,3 Junling Liu,1,2 Chengda Ren,1,2 Ding Xu,1 Jing Yu1
1Department of Ophthalmology, Shanghai Tenth People’s Hospital, Shanghai, 2Tongji University School of Medicine, Shanghai, 3Department of First Clinical Medical College, Nanjing Medical University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Background: The purpose of this meta-analysis was to assess the efficacy and safety of intravitreal corticosteroid implants for macular edema.
Methods: A total of 3,586 patients from previously reported randomized controlled trials were included. The meta-analysis was performed using RevMan 5.2. Summary odds ratios (ORs) and 95% confidence intervals (CIs) were calculated, employing random-effects or fixed-effects models according to between-study heterogeneity. The main outcome measures were the ORs for effects and safety of intravitreal corticosteroid implants.
Results: Four eligible studies were included. Compared with the sham group, the ORs for ≥15 letter improvement of visual acuity in the high-dose and low-dose groups were 1.89 (95% CI 1.33–2.69, P=0.0004) and 1.62 (95% CI 1.10–2.41, P=0.02), respectively. The weight mean differences in central retinal thickness increases were -75.46 (95% CI -90.29, -60.63, P<0.0001) and -46.47 (95% CI -92.08, -0.86, P=0.05), respectively. However, the ORs for increased intraocular pressure in both intervention groups were higher than in the sham group, and were 11.50 (95% CI 7.24–18.28, P<0.00001) and 10.30 (95% CI 6.49–16.36, P<0.00001), respectively. The incidence of cataract was 7.25 (95% CI 5.68–9.25, P<0.00001) and 3.56 (95% CI 1.28–9.96, P=0.02) in the two intervention groups, respectively. There was no significant difference between the intervention groups except for the incidence of cataract in which the OR was 1.59 (95% CI 1.28–1.97, P<0.001).
Conclusion: Intravitreal corticosteroid implants are effective in treating macular edema. However, the efficacy is not related to corticosteroid dose.
Keywords: corticosteroid implant, intravitreal, macular edema, randomized controlled trial
A Letter to the Editor has been recieved and published for this article.
Corrigendum for this paper has been published
Introduction
Macular edema (ME) and its associated reduction in central vision are caused by abnormal retinal capillary permeability leading to extravascular swelling in the central retina.1 ME is associated with several disorders, including diabetic retinopathy, retinal vein occlusion, and uveitis, and is one of the leading causes of vision loss in patients with diabetes.2 A variety of processes have been implicated in the breakdown of the blood–retinal barrier that leads to ME. These processes include production of proinflammatory mediators (such as prostaglandins and interleukin-6), increased amounts of vascular permeability factors, such as vascular endothelial growth factor (VEGF), and loss of endothelial tight junction integrity.3
In recent years, anti-inflammatory and antiangiogenic strategies have been used to target vascular permeability and leakage to reduce ME and improve vision. Intraocular corticosteroids are used for a variety of ophthalmological conditions such as diabetic ME, posterior uveitis, and ME secondary to vascular occlusion.4 Corticosteroids have anti-inflammatory, antiangiogenic, and antipermeability properties that make them an attractive therapeutic option for a variety of posterior segment diseases.
The principal effects of steroids are thought to be mediated by stabilization of the blood–retinal barrier, reduction of exudates, and downregulation of inflammatory stimuli.5 Based on experimental studies, clinical observations, and pathogenic considerations, intravitreal delivery of steroids was suggested to suppress local intraocular inflammation, cell proliferation, and neovascularization.6,7 However, many of these conditions are chronic and require repeated injections for prolonged periods of time. This is inconvenient for patients and may increase the risk of complications secondary to the injection procedure, including endophthalmitis and vitreous hemorrhage.
In order to mitigate the cumulative risk associated with repeated intravitreal injections, extended-release steroid implants have been investigated for the treatment of ME. The three sustained-release corticosteroid implants currently available include Ozurdex® (Allergan Inc., Irvine, CA, USA), which releases dexamethasone, and Retisert® (Bausch and Lomb, Rochester, NY, USA) and Iluvien® (Alimera Science, Alpharetta, GA, USA), both of which release fluocinolone acetonide. However, long-acting steroid preparations have potential side effects including cataract and glaucoma, which are more likely to occur when treatment exceeds 6 months. This may result in additional intraocular surgery and can be considered a drawback of treatment.8
The objective of this meta-analysis was to assess the efficacy and safety of intravitreal corticosteroid implants.
Materials and methods
Literature search
A systematic English language search of MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, and Web of Science with language restriction was conducted from inception to November 2014. Key terms used for the systematic search were “macular edema/oedema”, “corticosteroid intravitreal implants”, “intravitreal dexamethasone drug delivery system”, “steroid implants”, “dexamethasone insert”, “Ozurdex”, “fluocinolone acetonide insert”, “Retisert”, and “Iluvien”. The search was restricted to randomized trials. We manually searched the reference lists of original studies and review articles identified by the electronic search for other potentially eligible articles.
Selection criteria
All selected publications were screened according to predefined selection criteria. Eligible studies met the following criteria: inclusion of a comparison of different doses of any intravitreal corticosteroid implant for the treatment of any type of ME, and use of visual acuity and central macular thickness as the main outcome measures. In publications with overlapping patients or controls, only the more current and complete data were included. Any study with inconsistent or erroneous data was excluded.
Data extraction
Two reviewers examined the electronic searches and obtained full reports of all citations that were likely to meet the selection criteria. Disagreements were resolved by consensus after discussion. The data extracted from each study contained the name of the first author, study design, study duration, study population characteristics (age, sex, number of patients, and eyes in study), treatment groups, comparison groups, outcome variables, and duration of follow-up.
Quality assessment
A Jadad quality assessment was conducted to assess the methodological quality of the included trials. In this assessment, quality was based upon four questions, with a score range of 0–7, and higher scores indicating better study quality.
Statistical analysis
A meta-analysis was conducted using RevMan5.2 software; during the data analysis, we performed separate meta-analyses for different treatment doses and control interventions, which were heterogeneous. Heterogeneity was assessed by calculating the I2 statistic and by performing a chi-square test (assessing the P-value). I2 is the proportion of total variation observed among the trials attributable to actual differences between the trials rather than to sampling error (chance), and I2 >50% is considered to be indicative of significant heterogeneity. Heterogeneity among the included studies can be tested using fixed-effect Poisson regression analysis. We chose patients who achieved a best corrected visual acuity improvement of more than 15 letters in studies in which the central retinal thickness (CRT) was the main result that indicated treatment effectiveness. Intraocular pressure (IOP) and presence of cataracts were the main data indicating treatment safety.
Results
Figure 1 shows a flow diagram of the selection process used to determine eligible studies. The first database query yielded 188 reports, the titles and abstracts of which were screened for potentially relevant articles. We identified 14 reports for which we obtained full-length articles. During examination of these full-length articles, ten were excluded from the present meta-analysis. Two studies were excluded because the control group was not a sham treatment.9,10 Several articles were from the same study group,11–18 and in these cases, the most informative and recent articles were included. As a result, four published19–22 articles were eligible for inclusion.
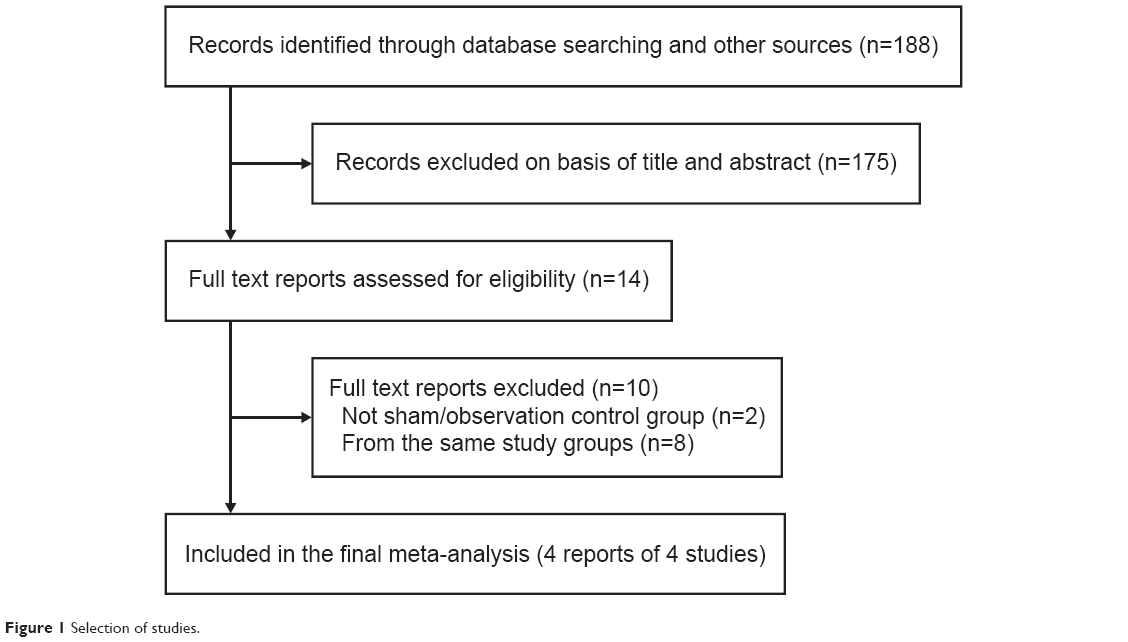 | Figure 1 Selection of studies. |
Included studies
The characteristics of the four included studies are outlined in Table 1. Study sample sizes ranged from 315 to 1,267 patients. Patient characteristics were similar among the trials, with the mean age ranging from 61.9 to 66.3 years. All patients in each study were randomized into three groups, ie, a high-dose group, a low-dose group, and a sham or observation group. The duration of follow-up ranged from 6 to 36 months. The methodological quality of the four studies was assessed based on the Jadad score, and all studies were determined to be of good quality.
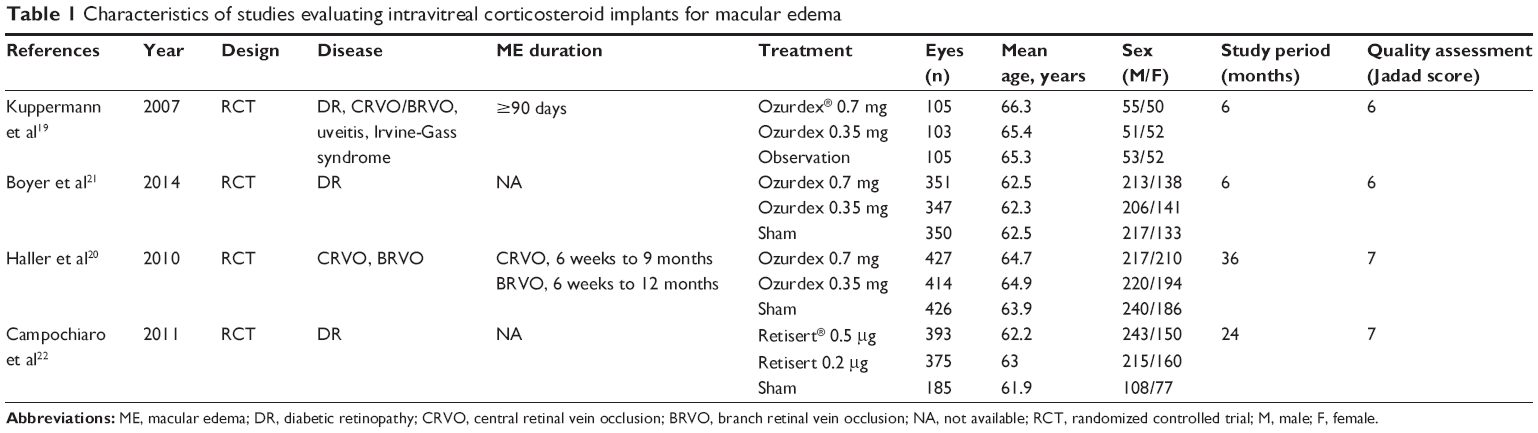 | Table 1 Characteristics of studies evaluating intravitreal corticosteroid implants for macular edema |
Effects of interventions
Improvement in visual acuity
Figure 2 shows the results of the meta-analysis for the effect of intravitreal corticosteroid implants on improvement in visual acuity of more than 15 letters. The odds ratio in the high-dose group was 1.89 (95% confidence interval [CI] 1.33–2.69, P=0.0004) and in the low-dose group was 1.62 (95% CI 1.10–2.41, P=0.02), with no significant difference between the two intervention groups.
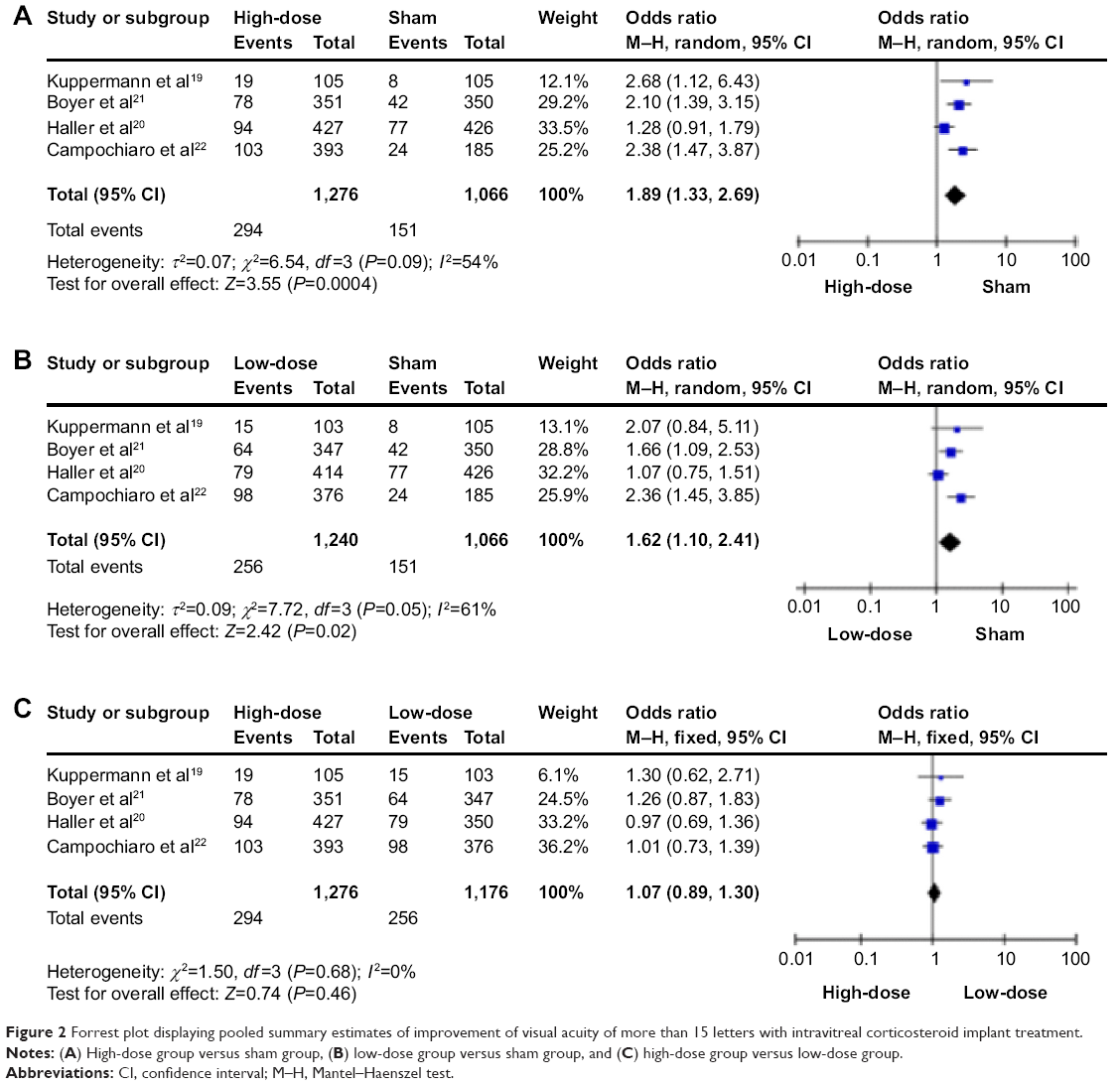 | Figure 2 Forrest plot displaying pooled summary estimates of improvement of visual acuity of more than 15 letters with intravitreal corticosteroid implant treatment. |
Central retinal thickness
Three studies measured the CRT as the main outcome measure. Figure 3 shows the effect of intravitreal corticosteroid implants on CRT. The CRT increased in the high-dose group when compared with the sham group (weight mean difference −75.46; 95% CI −90.29, −60.63, P<0.0001) and the low-dose group (weight mean difference −46.47; 95% CI −92.08, −0.86, P=0.05). There was no significant difference in CRT between the two intervention groups.
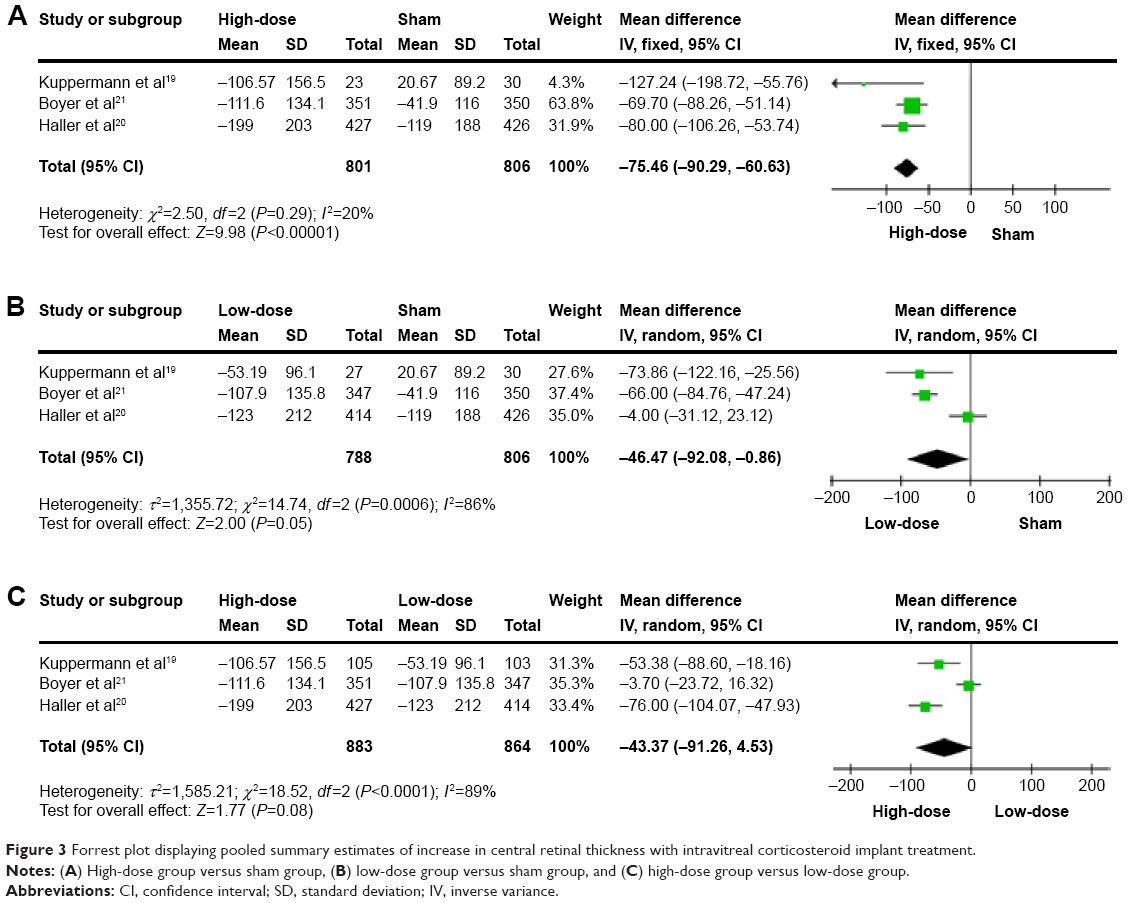 | Figure 3 Forrest plot displaying pooled summary estimates of increase in central retinal thickness with intravitreal corticosteroid implant treatment. |
Safety analysis
Increased IOP
High IOP is known to be one of the main side effects of intravitreal steroids. All studies reported that IOP increased in the treatment groups (Figure 4). The odds ratio in the high-dose group was 11.50 (95% CI 7.24–18.28, P<0.00001) and in the low-dose group was 10.30 (95% CI 6.49–16.36, P<0.00001). There was no significant difference between the two intervention groups.
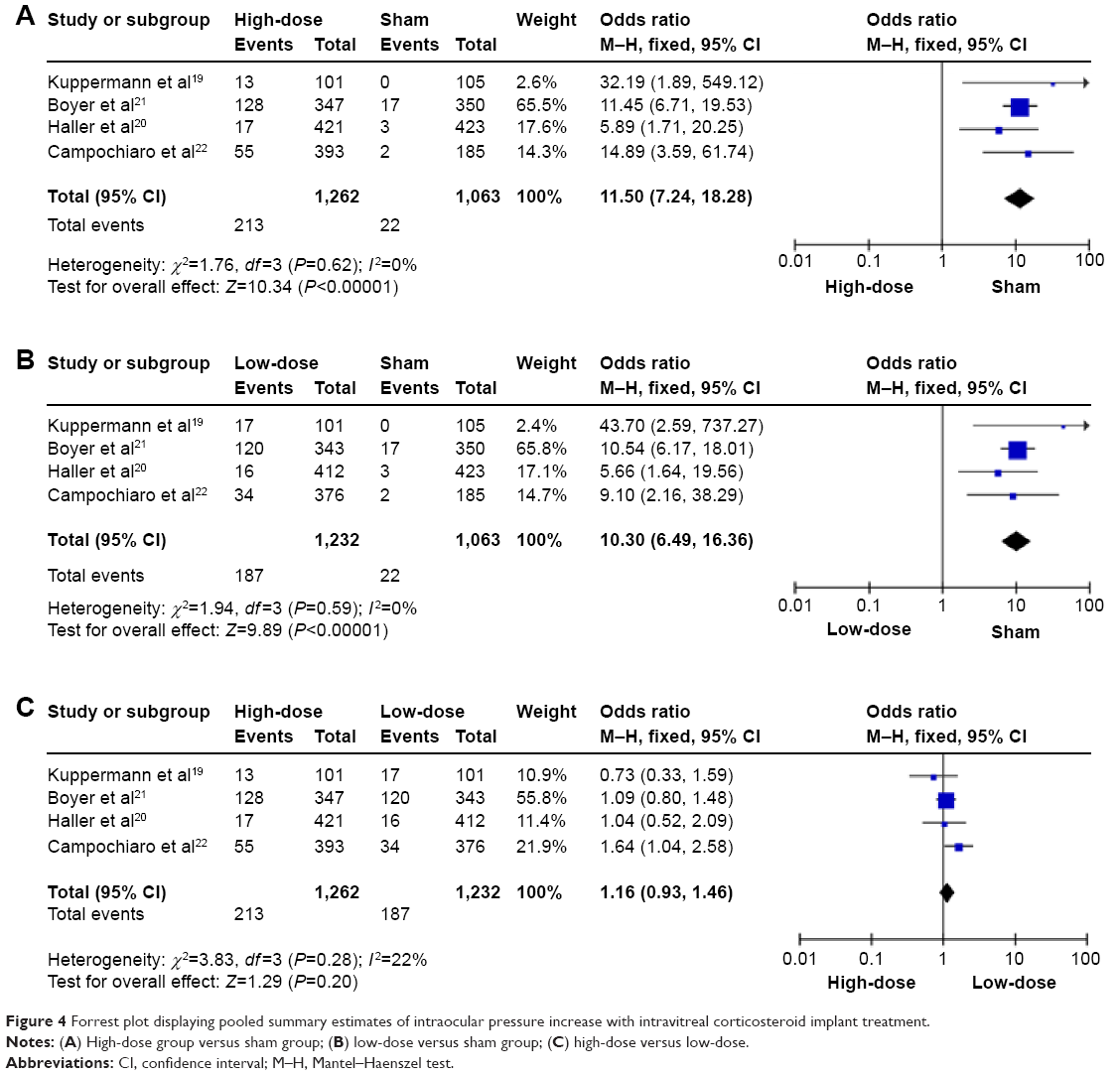 | Figure 4 Forrest plot displaying pooled summary estimates of intraocular pressure increase with intravitreal corticosteroid implant treatment. |
Incidence of cataracts
Three20–22 of the four studies (excluding Kuppermann et al19) reported a significant difference in the incidence of cataract between the intervention and sham groups. Figure 5 shows that the odds ratio in the high-dose group was 7.25 (95% CI 5.68–9.25, P<0.00001) and in the low-dose group was 3.56 (95% CI 1.28–9.96, P=0.02). When the high-dose group was compared with the low-dose group, the odds ratio was 1.59 (95% CI 1.28–1.97, P<0.001).
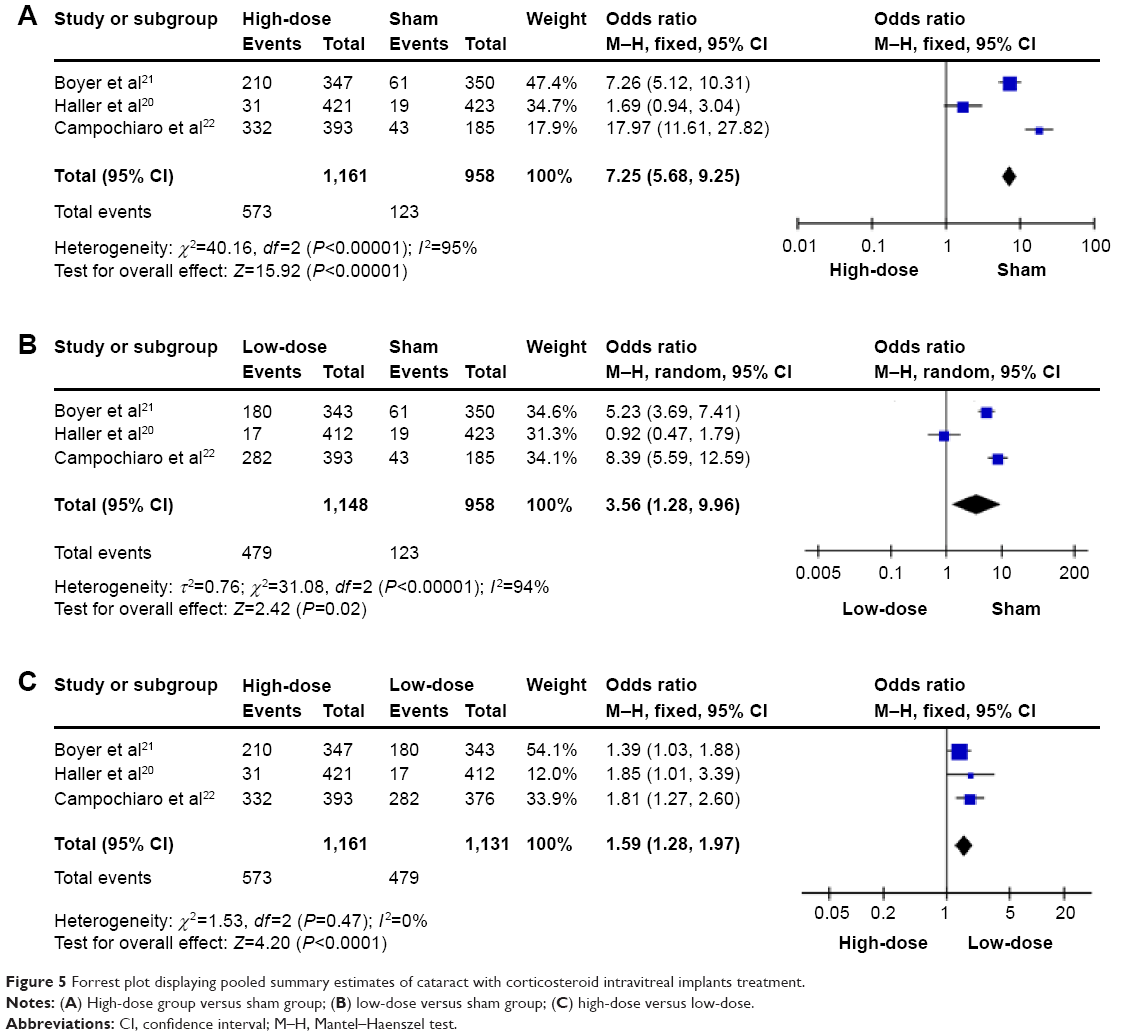 | Figure 5 Forrest plot displaying pooled summary estimates of cataract with corticosteroid intravitreal implants treatment. |
Other adverse events
There were other adverse events following the use of intravitreal steroids, including increased amounts of anterior chamber cells, eye pain, and vitreous floaters. Table 2 shows the common adverse events reported in the three studies. The incidence of increased amounts of anterior chamber cells in the high-dose group and the low-dose group was 3.34% (P<0.0001) and 4.80% (P<0.00001), respectively, compared with 0.46% in the sham group. Compared with the sham group, the percentages of conjunctival hemorrhage, eye pain, and vitreous floaters in the high-dose group were 19.33% (P=0.02), 7.36% (P<0.002), and 5.06% (P<0.0002), respectively. There were no significant differences between the low-dose group and the sham group. In the two intervention groups, the incidences of vitreous floaters and vitreous hemorrhage were 5.06% and 6.44% in the high-dose group, and 2.57% (P<0.007) and 9.24% (P<0.03) in the low-dose group, respectively.
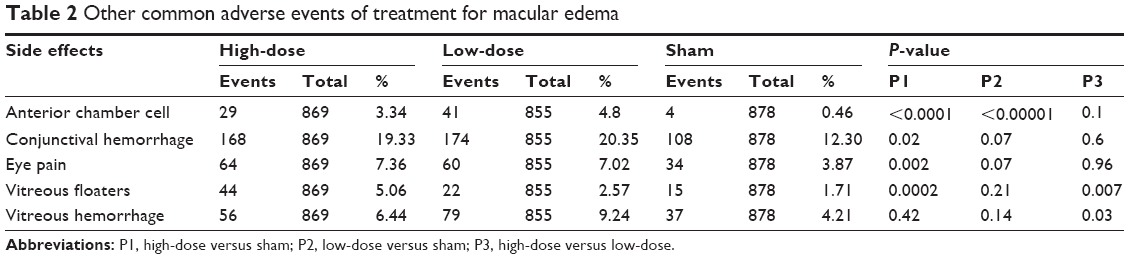 | Table 2 Other common adverse events of treatment for macular edema |
Discussion
Use of steroids for the treatment of ME has been studied for many years because of their strong anti-inflammatory and antiedema properties. Several studies have reported on the effects of steroids in reducing expression of VEGF, leukostasis, and production of inflammatory cytokines.23 Intravitreally administered steroids stabilize visual acuity and reduce ME, but are also frequently associated with side effects, the most common (reported for all types of steroids) of which is an increase in IOP and progression of cataract. For this reason, steroids are generally used in patients affected by persistent or refractory ME, particularly in pseudophakic eyes. The long-term efficacy and safety of implants is still under assessment.
A systematic review published by Pielen et al24 compared anti-VEGF agents (ranibizumab, bevacizumab, and aflibercept) versus steroids (triamcinolone and Ozurdex) for ME in central retinal vein occlusion and branch retinal vein occlusion. All anti-VEGF agents resulted in a better visual acuity gain compared with steroids after 12 months of treatment. The downside was that anti-VEGF therapy required more frequent injections (approximately eight injections per year, compared with two injections in the steroid group). The dexamethasone implant may be of value in vitrectomized eyes, where anti-VEGF has shown a significantly shorter half-life compared with nonvitrectomized eyes in previous reports,25 although some authors argue there is no difference.26 Ozurdex has also been proposed as a treatment for diabetic ME, and some case series have been published stating that Ozurdex is useful in recalcitrant diabetic ME.27,28
Retisert has been proposed as a treatment for diabetic ME. Compared with laser therapy, the percentage of eyes that gained three more lines of vision was significantly higher in the Retisert implant group.10 Retisert was evaluated in a prospective case series of 23 patients with central retinal vein occlusion,29 but a significant increase in visual acuity compared with baseline was not observed at 3-year follow up, despite improvements in CRT and 50% of eyes gaining ten or more letters of vision. Ocular adverse events were similar to those reported in previous studies. Iluvien failed to secure US Food and Drug Administration approval in the USA. No data are available for the treatment of ME arising from central or branch retinal vein occlusion. Nevertheless, Iluvien is approved in several European countries for the treatment of refractory/persistent diabetic ME.
We evaluated the efficacy of treatment with the steroid implant. Our analysis showed that both intervention groups were effective, with a higher proportion of improved visual acuity in treated eyes and a smaller increase in CRT than in the control group. However, it seemed that the effectiveness was not significantly related to dosage. Therefore, we propose that the lowest therapeutic dose would be the best choice to reduce side effects.
Ocular adverse events occurred more frequently in the treatment groups than in the control group, and could be divided into steroid-related and implant-related adverse events. The most important side effects of the two treatments were increased IOP and cataracts. Other side effects such as increased anterior chamber cells, conjunctival hemorrhage, eye pain, vitreous floaters, and vitreous hemorrhage were reported in three studies, and were regarded as side effects related to complications of the intravitreal implant.
Corticosteroids can cause elevation of IOP and formation of cataract regardless of route of administration. IOP elevation and cataract formation have been hypothesized to share the same mechanism, possibly involving activation of a common steroid receptor that may be located in the trabecular meshwork and lens.30 We found it interesting that there was no significant correlation between increased IOP and steroid dosage, whereas the incidence of formation of cataract was higher in the high-dose group than in the low-dose group. There might be several factors contributing to this phenomenon. First, some enrolled patients had pseudophakic eyes in which the side effect of cataract formation could not be considered; second, the study period ranged from 6 to 36 months, and this time frame may have affected cataract formation. Thus, larger and longer-term clinical trials are warranted to further explore the issue as to whether corticosteroid side effects are dose-related.
Comparisons of the intervention groups showed that the incidence of vitreous floaters was higher in the high-dose group than in the low-dose group, whereas the opposite was true for incidence of vitreous hemorrhage. We determined that the incidence of vitreous floaters was related to the corticosteroid dose, as the more drug that was released into the system, the more floaters there were in the vitreous cavity. However, with the higher dose, the incidence of vitreous hemorrhage decreased. This may result from the antiangiogenic properties of corticosteroids.
Considering all of the above information, this meta-analysis should be regarded as an indicator that intravitreal corticosteroid implants are effective in treating patients with ME caused by diabetic retinopathy or retinal vein occlusion. The efficacy of treatment was not significantly related to corticosteroid dose. The side effects of this treatment still need to be considered, and further study is required to demonstrate the relationship between the observed side effects and drug dosage. This meta-analysis is intended to serve as evidence for the use of intravitreal steroid implants in clinical therapy.
Acknowledgments
This work was financially supported by the National Natural Science Foundation of China in 2014 (81470648) and the project of Shanghai Health System Training Program for Outstanding Young Talents (XYQ2011067).
Disclosure
The authors report no conflicts of interest in this work.
References
Ferris FL 3rd, Patz A. Macular edema. A complication of diabetic retinopathy. Surv Ophthalmol. 1984;28 Suppl:452–461. | |||
Klein R, Klein BE, Moss SE, Cruickshanks KJ. The Wisconsin Epidemiologic Study of Diabetic Retinopathy. XV. The long-term incidence of macular edema. Ophthalmology. 1995;102(1):7–16. | |||
Antonetti DA, Barber AJ, Khin S, Lieth E, Tarbell JM, Gardner TW. Vascular permeability in experimental diabetes is associated with reduced endothelial occludin content: vascular endothelial growth factor decreases occludin in retinal endothelial cells. Penn State Retina Research Group. Diabetes. 1998;47(12):1953–1959. | |||
Cabrera M, Yeh S, Albini TA. Sustained-release corticosteroid options. J Ophthalmol. 2014;2014:164692. | |||
Sarao V, Veritti D, Boscia F, Lanzetta P. Intravitreal steroids for the treatment of retinal diseases. Scientific World Journal. 2014;2014:989501. | |||
Gillies MC, Sutter FK, Simpson JM, Larsson J, Ali H, Zhu M. Intravitreal triamcinolone for refractory diabetic macular edema: two-year results of a double-masked, placebo-controlled, randomized clinical trial. Ophthalmology. 2006;113(9):1533–1538. | |||
Jonas JB, Kamppeter BA, Harder B, Vossmerbaeumer U, Sauder G, Spandau UH. Intravitreal triamcinolone acetonide for diabetic macular edema: a prospective, randomized study. J Ocul Pharmacol Ther. 2006;22(3):200–207. | |||
Comyn O, Lightman SL, Hykin PG. Corticosteroid intravitreal implants vs ranibizumab for the treatment of vitreoretinal disease. Curr Opin Ophthalmol. 2013;24(3):248–254. | |||
Callanan DG, Gupta S, Boyer DS, et al. Ozurdex PLACID Study Group. Dexamethasone intravitreal implant in combination with laser photocoagulation for the treatment of diffuse diabetic macular edema. Ophthalmology. 2013;120(9):1843–1851. | |||
Pearson PA, Comstock TL, Ip M, et al. Fluocinolone acetonide intravitreal implant for diabetic macular edema: a 3-year multicenter, randomized, controlled clinical trial. Ophthalmology. 2011;118(8):1580–1587. | |||
Williams GA, Haller JA, Kuppermann BD, et al. Dexamethasone DDS Phase II Study Group. Dexamethasone posterior-segment drug delivery system in the treatment of macular edema resulting from uveitis or Irvine-Gass syndrome. Am J Ophthalmol. 2009;147(6):1048–1054. | |||
Haller JA, Kuppermann BD, Blumenkranz MS, et al. Dexamethasone DDS Phase II Study Group. Randomized controlled trial of an intravitreous dexamethasone drug delivery system in patients with diabetic macular edema. Arch Ophthalmol. 2010;128(3):289–296. | |||
Blumenkranz MS, Haller JA, Kuppermann BD, et al. Correlation of visual acuity and macular thickness measured by optical coherence tomography in patients with persistent macular edema. Retina. 2010;30(7):1090–1094. | |||
Haller JA, Bandello F, Belfort R Jr, et al; Ozurdex GENEVA Study Group. Dexamethasone intravitreal implant in patients with macular edema related to branch or central retinal vein occlusion twelve-month study results. Ophthalmology. 2011;118(12):2453–2460. | |||
Yeh WS, Haller JA, Lanzetta P, et al. Effect of the duration of macular edema on clinical outcomes in retinal vein occlusion treated with dexamethasone intravitreal implant. Ophthalmology. 2012;119(6):1190–1198. | |||
Sadda S, Danis RP, Pappuru RR, et al. Vascular changes in eyes treated with dexamethasone intravitreal implant for macular edema after retinal vein occlusion. Ophthalmology. 2013;120(7):1423–1431. | |||
Campochiaro PA, Brown DM, Pearson A, et al; FAME Study Group. Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema. Ophthalmology. 2012;119(10):2125–2132. | |||
Cunha-Vaz J, Ashton P, Iezzi R, et al; FAME Study Group. Sustained delivery fluocinolone acetonide vitreous implants: long-term benefit in patients with chronic diabetic macular edema. Ophthalmology. 2014;121(10):1892–1903. | |||
Kuppermann BD, Blumenkranz MS, Haller JA, et al. Dexamethasone DDS Phase II Study Group. Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch Ophthalmol. 2007;125(3):309–317. | |||
Haller JA, Bandello F, Belfort R Jr, et al; Ozurdex Geneva Study Group. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010;117(6):1134–1146.e3. | |||
Boyer DS, Yoon YH, Belfort R Jr, et al; Ozurdex MEAD Study Group. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014;121(10):1904–1914. | |||
Campochiaro PA, Brown DM, Pearson A, et al; FAME Study Group. Long-term benefit of sustained-delivery fluocinolone acetonide vitreous inserts for diabetic macular edema. Ophthalmology. 2011;118(4):626–635.e2. | |||
Tamura H, Miyamoto K, Kiryu J, et al. Intravitreal injection of corticosteroid attenuates leukostasis and vascular leakage in experimental diabetic retina. Invest Ophthalmol Vis Sci. 2005;46(4):1440–1444. | |||
Pielen A, Feltgen N, Isserstedt C, Callizo J, Junker B, Schmucker C. Efficacy and safety of intravitreal therapy in macular edema due to branch and central retinal vein occlusion: a systematic review. PLoS One. 2013;8(10):e78538. | |||
Moisseiev E, Waisbourd M, Ben-Artsi E, et al. Pharmacokinetics of bevacizumab after topical and intravitreal administration in human eyes. Graefes Arch Clin Exp Ophthalmol. 2014;252(2):331–337. | |||
Ahn J, Kim H, Woo SJ, et al. Pharmacokinetics of intravitreally injected bevacizumab in vitrectomized eyes. J Ocul Pharmacol Ther. 2013;29(7):612–618. | |||
Dutra Medeiros M, Postorino M, Navarro R, Garcia-Arumí J, Mateo C, Corcóstegui B. Dexamethasone intravitreal implant for treatment of patients with persistent diabetic macular edema. Ophthalmologica. 2014;231(3):141–146. | |||
Pacella E, Vestri AR, Muscella R, et al. Preliminary results of an intravitreal dexamethasone implant (Ozurdex®) in patients with persistent diabetic macular edema. Clin Ophthalmol. 2013;7:1423–1428. | |||
Jain N, Stinnett SS, Jaffe GJ. Prospective study of a fluocinolone acetonide implant for chronic macular edema from central retinal vein occlusion: thirty-six-month results. Ophthalmology. 2012;119(1):132–137. | |||
Gillies MC, Kuzniarz M, Craig J, Ball M, Luo W, Simpson JM. Intravitreal triamcinolone-induced elevated intraocular pressure is associated with the development of posterior subcapsular cataract. Ophthalmology. 2005;112(1):139–143. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.