")
Back to Journals » Drug Design, Development and Therapy » Volume 8
Difference in the effects of switching from Candesartan to Olmesartan or Telmisartan to Olmesartan in hypertensive patients with type 2 diabetes: the COTO study
Authors Daikuhara H, Fukunaga K, Ohshima T
Received 19 August 2013
Accepted for publication 28 November 2013
Published 17 February 2014 Volume 2014:8 Pages 219—226
DOI https://doi.org/10.2147/DDDT.S53253
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Hiroyuki Daikuhara, Kensaku Fukunaga, Tomie Ohshima
Department of Internal Medicine, Sakaide City Hospital, Kagawa, Japan
Purpose: This open-label controlled study compared the therapeutic efficacy of three representative angiotensin II receptor blockers (ARBs) in hypertensive patients with type 2 diabetes attending a hospital outpatient clinic. The primary measure in this study was morning home blood pressure (BP).
Patients and methods: Two studies were done concurrently to investigate the effects of switching from two different ARBs to olmesartan. Patients prescribed candesartan (8 mg once daily in the morning) or telmisartan (40 mg once daily in the morning) for 16 weeks were switched to olmesartan (20 mg once daily in the morning) for 16 weeks. Then, they were switched back to candesartan (CO group) or telmisartan (TO group) for another 16 weeks.
Results: Data from all patients in the CO group (n=165) and the TO group (n=152) were analyzed. Clinic and morning home BP and urinary albumin levels showed a significant decrease from baseline at 16 weeks after switching to olmesartan in both the CO and the TO group (clinic BP, morning home diastolic BP, and urinary albumin, P<0.05; morning home systolic BP, P<0.01). In contrast, clinic BP, morning home BP, and urinary albumin were significantly increased again 16 weeks after switching back to candesartan or telmisartan (clinic BP, morning home diastolic BP, and urinary albumin, P<0.05; morning home systolic BP, P<0.01). No subjects experienced an adverse reaction that required withdrawal from the study. No adverse reactions attributable to the study drugs were observed.
Conclusion: Olmesartan is a promising ARB for BP control in hypertensive type 2 diabetics.
Keywords: type 2 diabetes, morning home blood pressure, albuminuria, olmesartan
Introduction
The Japanese Society of Hypertension (JSH) Guideline for the Management of Hypertension (JSH 2009) mentions the necessity for tight blood pressure (BP) control in patients with type 2 diabetes.1 JSH 2009 recommends that the target BP for hypertensive type 2 diabetics should be 130/80 mmHg as the clinic BP, and 125/75 mmHg as the home BP. Despite this recommendation of the JSH 2009, the target BP is achieved in only 30%–40% of patients.2 Based on evidence for the improvement of glucose metabolism and cardiorenal protection, the JSH 2009 recommends angiotensin II receptor blockers (ARBs) as first-line antihypertensive drugs for hypertensive patients with type 2 diabetes.1 However, hypertensive type 2 diabetics are commonly treated with various combinations of drugs, because these patients do not respond well to antihypertensive therapy. Therefore, it would be desirable to include at least one drug that shows efficacy for hypertensive diabetics in the case of combined therapy.
Among ARBs, olmesartan has been reported to show the highest level of binding with the angiotensin II type 1 receptor and, thus, has a strong hypotensive effect.3–5 Recently, it was reported that olmesartan effectively controlled both the clinic BP and the morning home BP after 16 weeks of treatment, indicating that its antihypertensive effect is stable over the medium term.6 As for candesartan, basic studies have shown that it can improve insulin sensitivity, but only limited clinical data that support this action of the drug have been published.7 Similarly, telmisartan has been shown to selectively bind with peroxisome proliferator-activated receptor gamma (PPARγ) in preclinical studies, and it has been suggested that this action may improve insulin sensitivity.8 However, the clinical data are insufficient to support this action of telmisartan.
In Japan, seven ARBs are currently marketed. However, there have been few reports regarding differences among these drugs in terms of achieving BP control in hypertensive patients with type 2 diabetes. Therefore, the purpose of this study was to compare the effects of three representative ARBs on morning home BP, urinary albumin excretion, and parameters of glucose metabolism in hypertensive patients with type 2 diabetes mellitus.
Patients and methods
Patients
Treated hypertensive patients with type 2 diabetes mellitus who were attending the outpatient clinic for diabetes mellitus at Sakaide City Hospital (Sakaide, Japan) were invited to participate in this single-center, open-label, controlled study. The study protocol was approved by the Institutional Ethical Committee at Sakaide City Hospital. All the patients were given an explanation of the study, and written consent to participate and for the use of their data was obtained before enrolment. We also explained to the patients that no personal information would be disclosed during the publication of the results.
Patients meeting the following criteria were eligible for inclusion: hypertension in the presence of type 2 diabetes mellitus; systolic BP or diastolic BP at medical examination of ≥130 mmHg or ≥80 mmHg, respectively; and no planned changes in antidiabetic therapy.
Patients meeting any of the following criteria were excluded: secondary hypertension or grade 3 hypertension; contraindication for any of the test drugs; uncontrolled diabetes mellitus; diabetic nephropathy (urinary albumin excretion ≥300 mg/g of creatinine [Cr]) before the late stage of overt nephropathy (because blood insulin clearance may decrease after the late stage of overt nephropathy and may mask glucose metabolic status); history of acute coronary syndrome or cerebrovascular disorders within 1 year of enrolment; severe infection before or after surgery, or serious trauma; history of hypersensitivity to the study drugs; pregnant women or women with the possibility of being pregnant; other reasons for ineligibility, as determined by the investigator.
Study design and treatment
The COTO study was, in effect, comprised of two studies done concurrently to investigate the effects of switching from candesartan to olmesartan, and from telmisartan to olmesartan (Figure 1).
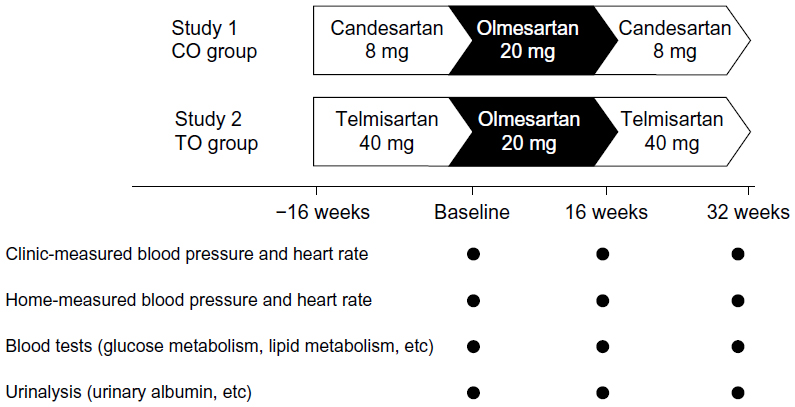 | Figure 1 Study design. |
In study 1, hypertensive patients with type 2 diabetes were treated with 8 mg of candesartan once daily in the morning for 16 weeks; these individuals were part of the CO group. Candesartan was switched to olmesartan, which was administered at 20 mg once daily in the morning for 16 weeks. Olmesartan was then switched back to candesartan, which was administered at 8 mg once daily for another 16 weeks.
In study 2, hypertensive patients with type 2 diabetes were treated with 40 mg of telmisartan once daily in the morning for 16 weeks; these individuals were part of the TO group. Telmisartan was switched to olmesartan, which was administered at 20 mg once daily in the morning for 16 weeks. Then, olmesartan was switched back to telmisartan, which was administered at 40 mg once daily for another 16 weeks.
The hypotensive effect of ARBs is influenced by the season when therapy is instituted, so the subjects were enrolled in this study evenly across the four seasons to avoid any seasonal bias on treatment effects.
The primary measure in this study was morning home BP. The secondary measures were clinic BP, glucose metabolism parameters, and urinary albumin.
In both groups, BP and heart rate were measured in the outpatient clinic and at home at baseline, 16 weeks, and 32 weeks. Fasting blood glucose, hemoglobin A1c (HbA1c) (US National Glycohemoglobin Standardization Program [NGSP]), and urinary albumin levels were measured at baseline, 16 weeks, and 32 weeks. During the treatment period, the type and dosage of concomitant antihypertensive drugs and antidiabetic treatments were not to be changed.
BP was measured in the clinic multiple times at 1- or 2-minute intervals, with the patient resting in a seated position. The mean value of two measurements that provide a stable value (difference in the values <5 mmHg) was recorded. BP was also measured at home after waking in the morning, using a pressure measurement device for the upper arm. The patient was instructed to measure BP while in the sitting position, with a 1- to 2-minute rest, after urination, but before the administration of hypotensive drugs, as recommended by the JSH 2009.1 Additional parameters were determined using blood and urine samples. Changes in BP and heart rate measured in the early morning at home, urinary albumin, HbA1c (NGSP), and fasting blood glucose between the start of therapy and after 16 weeks and 32 weeks of therapy were defined as endpoints in this study. HbA1c was measured by column chromatography at our institute. Urinary albumin levels were measured by a turbidimetric immunoassay at Shikoku Chuken, Inc. (Takamatsu, Japan) Values are expressed in all patients as means ± standard deviation, except for the urinary albumin level values, which are expressed as means ± standard error.
Unpaired t-tests and paired t-tests were used to determine the significance of the differences between the two groups and within each group, respectively. The number of patients who achieved their target BP was compared using the χ2-test. The level of significance was set at 5%. Intention-to-treat analytical procedures were applied.
Results
Between January 2011 and January 2012, hypertensive patients with type 2 diabetes were enrolled. After enrollment, 165 patients received candesartan (CO group) and 152 patients received telmisartan (TO group) for 16 weeks. The baseline characteristics of these two groups are listed in Table 1. The baseline values are measurements that are performed before treatment with olmesartan, but after the patients had received candesartan or telmisartan. Both groups were comparable with respect to their patients’ baseline characteristics.
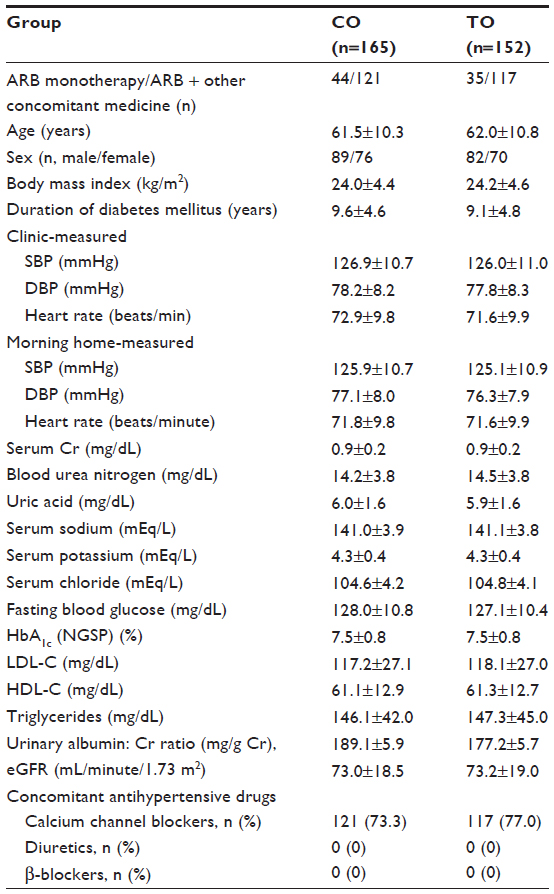 | Table 1 Patient characteristicsa |
Data from all patients in the CO group and TO group were analyzed. Changes in the clinic BP, morning home BP, as well as parameters of glucose metabolism and urinary albumin obtained during the study are shown in Tables 2 and 3.
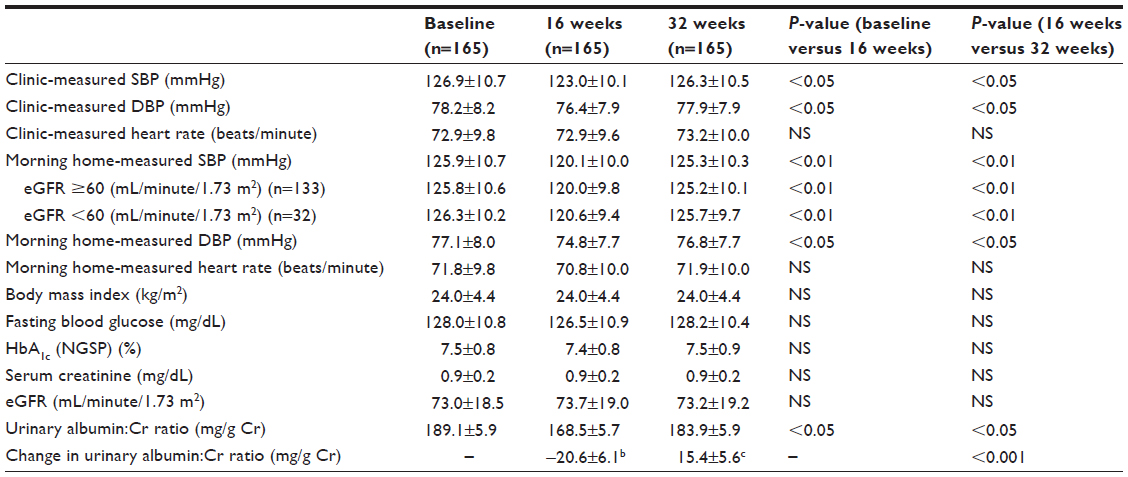 | Table 2 Change in parameters of the candesartan–olmesartan groupa |
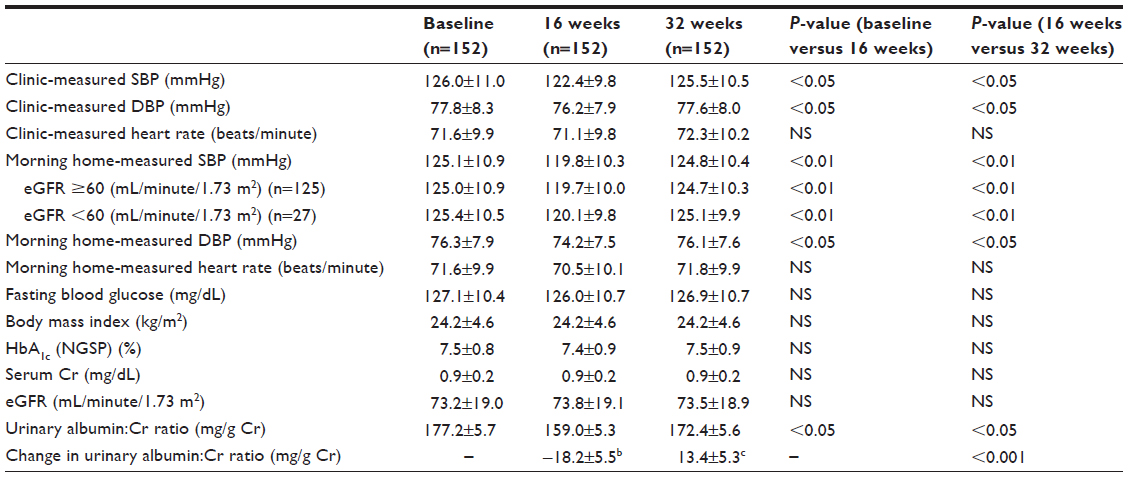 | Table 3 Change in parameters of the telmisartan–olmesartan groupa |
In study 1 (Table 2), in the CO group’s clinic BP showed a significant decrease after 16 weeks of treatment with olmesartan in comparison with the baseline clinic BP measured at the end of the initial candesartan treatment during the 16-week run-in period. After switching back to the candesartan treatment for another 16 weeks, the patients’ clinic BP was significantly elevated again. Morning home BP was also significantly decreased by 16 weeks of treatment with olmesartan in comparison with the baseline morning home BP at the end of the run-in period. At 16 weeks after switching back to candesartan treatment, the morning home BP was also significantly elevated again.
Glucose metabolism was assessed from the fasting blood glucose and HbA1c values. There were no significant changes at any of the times of assessment, including at the time of switching to olmesartan, after 16 weeks of olmesartan treatment, and after switching back to candesartan for another 16 weeks (week 32).
In study 2 (Table 3), in the TO group, the clinic BP was significantly decreased as a result of treatment with olmesartan for 16 weeks when compared with the baseline clinic BP measured at the end of the initial telmisartan treatment time during the 16-week run-in period. After switching back to telmisartan for another 16 weeks (week 32), the clinic BP was significantly elevated again. Morning home BP was also significantly decreased after 16 weeks of treatment with olmesartan in comparison with the baseline morning home BP at the end of the run-in period. After switching back to telmisartan treatment for another 16 weeks, the morning home BP was also significantly elevated again.
Glucose metabolism (fasting blood glucose and HbA1c) showed no significant changes at any of the times of assessment, including at the time of switching to olmesartan, after 16 weeks of olmesartan treatment, and after switching back to telmisartan for 16 weeks (week 32).
Therefore, treatment with olmesartan achieved similar outcomes in both the CO group and the TO group in terms of clinic BP, morning home BP, and the parameters of glucose metabolism.
In the CO group, treatment with olmesartan resulted in a decrease in the urinary albumin level by 20.6±6.1 mg/g Cr from baseline, whereas it increased by 15.4±5.6 mg/g Cr after switching back to treatment with candesartan for another 16 weeks. There was a significant difference between olmesartan and candesartan with regard to the change in urinary albumin excretion (P<0.001). In the TO group, treatment with olmesartan resulted in a decrease in urinary albumin by 18.2±5.5 mg/g Cr from baseline, whereas it increased by 13.4±5.3 mg/g Cr after switching back to treatment with telmisartan for another 16 weeks. There was a significant difference between olmesartan and telmisartan in terms of the change in urinary albumin excretion (P<0.001).
In the CO group, the achievement rate for the target clinic BP (<130/80 mmHg) was 63.6% at week 0 after the initial candesartan treatment (during the run-in period), and 64.8% at week 32 (upon completion of another 16-week treatment period) with candesartan after switching back from olmesartan, whereas this level showed a significant increase to 74.5% at week 16 of olmesartan treatment. In the TO group, the achievement rate for the target clinic BP was 65.1% at week 0 after the initial telmisartan treatment during the run-in period, and 65.8% at week 32 upon completion of another 16-week treatment period with telmisartan after switching back from olmesartan; conversely, there was a significant increase to 77.0% at week 16 of olmesartan treatment.
Figure 2 shows the achievement rates for the target morning home BP (<125/75 mmHg). Regarding the home BP, the target achievement rate of the home BP in the CO group was 44.2% at week 0 after the initial candesartan treatment during the run-in period, and 45.5% at week 32 upon completion of another 16-week period of candesartan treatment. There was a significant increase in the rate to 60.6% at week 16 of olmesartan treatment. In the TO group, the achievement rate for the target home BP was 46.1% at week 0 after the initial telmisartan treatment during the run-in period, and 47.4% at week 32 upon completion of another 16-week period of telmisartan treatment; conversely, it increased significantly to 61.2% at week 16 of olmesartan treatment. Overall, the achievement rate for the target home BP was lower than that for the clinic BP.
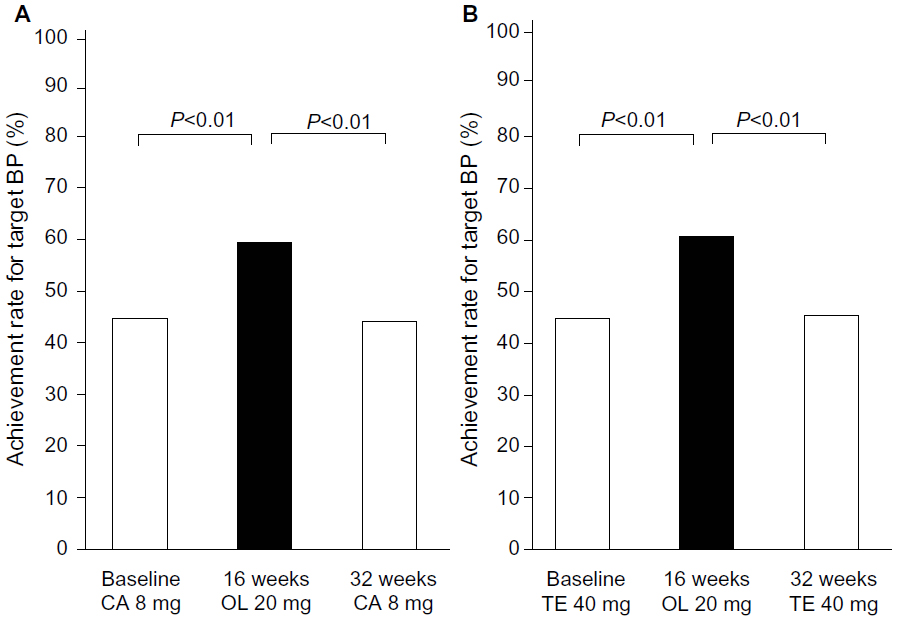 | Figure 2 Achievement rates for target home BP. |
In both groups, none of the subjects experienced any symptoms or adverse reactions that required withdrawal during the study. Similarly, we noted no adverse reactions caused by administration of the study drugs.
Discussion
This study compared three ARBs in terms of their ability to achieve the target BP level recommended by JSH 2009 for patients with type 2 diabetes, because this antihypertensive drug class is most widely used for the treatment of hypertensive patients with type 2 diabetes. Briefly, treatment with olmesartan for 16 weeks after switching from candesartan or telmisartan achieved a significant reduction in the clinic BP, morning home BP, and urinary albumin excretion from baseline levels. In the present study of hypertensive type 2 diabetics, the target achievement rates for both clinic BP and morning home BP were significantly higher after the completion of 16 weeks of olmesartan therapy than after the completion of 16 weeks of treatment with candesartan or telmisartan. This result suggests that the hypotensive effect of olmesartan is stronger and more sustained than that of the other two ARBs.
Regarding the strength and durability of the antihypertensive effect of olmesartan in patients with essential hypertension, Brunner et al5 conducted a double-blind controlled study that compared olmesartan and candesartan on the basis of ambulatory BP, whereas Sezai et al9 assessed the antihypertensive effect of olmesartan on early morning BP, and Furukawa et al10 investigated the efficacy of olmesartan therapy on ambulatory BP monitoring. These studies have revealed the superiority of olmesartan over candesartan with regard to the strength and duration of its antihypertensive effects. Nakayama et al11 compared olmesartan and telmisartan in type 2 diabetics with hypertension and reported that olmesartan achieved superior control of the 24-hour BP and nocturnal BP on the basis of ambulatory BP monitoring; it also had a stronger inflammatory effect than telmisartan. It has also been reported that switching from telmisartan to olmesartan resulted in a further reduction in BP and a decrease in urinary cystatin C, a marker of renal function.12 When olmesartan was administered to hypertensive patients with chronic kidney disease, the circadian rhythm of BP was altered from a nondipper pattern to a dipper pattern by its natriuretic activity;13 this effect has not been reported for other ARBs. Similarly, olmesartan has been found to improve circadian rhythm of BP in patients with essential hypertension and diabetics.14 In the Japan Morning Surge–Target Organ Protection (J-TOP) study of candesartan,15 microalbuminuria was more effectively decreased by bedtime dosing compared with morning dosing. In that study, the dosage of candesartan was increased on the basis of home BP, so there were no significant between-group differences in morning BP, evening BP, or bedtime BP. However, there was a difference in BP between the morning and evening, which suggests that morning dosing and bedtime dosing of candesartan have different effects on urinary albumin excretion. Also, the intensified inhibitory effect on urinary albumin excretion was suggested to be independent of the circadian variation in BP. Nevertheless, in the recent study16 of olmesartan that similarly compared evening dosing with morning dosing, olmesartan was suggested to show a well-sustained antihypertensive effect independent of dosing time when given once daily. That is, olmesartan significantly reduced the urinary albumin:Cr ratio when given in the morning or in the evening, but there was no significant difference in the reduction of this ratio between the morning and evening dosing groups. The inhibitory effect of olmesartan on albuminuria was not affected by the dosing time, because olmesartan exhibits a strong antihypertensive effect that is sustained for 24 hours, irrespective of whether the drug is administered in the morning or in the evening.
In the present study, the change in urinary albumin from baseline showed a significant difference between olmesartan treatment and candesartan treatment or telmisartan treatment. This difference in the change in urinary albumin excretion is considered to reflect the sustained antihypertensive effect of olmesartan. Furthermore, we previously reported that olmesartan plus azelnidipine was more effective at lowering morning home BP and reducing urinary albumin than candesartan plus amlodipine in the combination of OLmesartan and a CAlcium channel blocker (OLCA) study.17 We had thought that the improvement in microalbuminuria seemed to be partially attributed to the difference between calcium channel blockers. However, we found in the present study that reducing urinary albumin might be explained by the difference between ARBs. Reducing urinary albumin may be associated with lowering home morning BP. While it has been reported that telmisartan activates PPARγ and, thus, can directly improve insulin sensitivity without involving angiotensin II type 1 receptor signaling, olmesartan was comparable to telmisartan in terms of its effect on the clinical parameters of glucose metabolism in the present study. This result also suggests that telmisartan does not have any action on PPARγ at the standard clinical dose used in the present study, although such an action has been detected in nonclinical studies using higher doses.18 The recently published 2013 European Society of Hypertension/European Society of Cardiology Guidelines state that the study ONTARGET has disproved the hypothesis that the PPARγ activity of telmisartan may render this compound more effective in preventing or delaying the onset of diabetes;19 the incidence of new diabetes was not significantly different between the telmisartan-alone and telmisartan-plus-ramipril groups in ONTARGET.20 Olmesartan was also similar to candesartan in terms of its effect on glucose metabolism. Therefore, all three ARBs were suggested to have a similar effect on HbA1c, although some differences in the effect on glucose metabolism may have been masked because of the strict glycemic control maintained by the subjects in this study.
This was not a randomized study, so we could not directly compare olmesartan with candesartan, or with telmisartan. Nonetheless, this study is thought to be clinically useful, because olmesartan and candesartan were assessed in the same patient cohort by switching between the two drugs, while olmesartan and telmisartan were similarly assessed, so that intercohort variation was avoided. Therefore, the study is important in view of the findings that further highlight that antihypertensive effects on morning home BP can be expected by switching treatment to olmesartan from other ARBs in hypertensive patients with type 2 diabetes.
Conclusion
In hypertensive patients with type 2 diabetes who had already been treated with candesartan or telmisartan, switching to olmesartan, which has the strongest BP-lowering effect in the ARB class, led to a further reduction in BP and a decrease in urinary albumin excretion. Therefore, olmesartan is suggested to be more effective than other ARBs for morning BP control in type 2 diabetics with hypertension.
Acknowledgments
Medical editorial assistance was provided by Nature Japan K.K. (Macmillan Medical Communications, Tokyo, Japan) and funded by Daiichi Sankyo Co, Ltd (Tokyo, Japan).
The sponsor had no control over the study design; the collection, analysis, and interpretation of data; or the decision to submit the paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
Ogihara T, Kikuchi K, Matsuoka H, et al; Japanese Society of Hypertension Committee. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Hypertens Res. 2009;32(1):3–107. | |
Katayama S, Inaba M, Morita T, Awata T, Shimamoto K, Kikkawa R. Blood pressure control in Japanese hypertensives with or without type 2 diabetes mellitus. Hypertens Res. 2000;23(6):601–605. | |
Kiya Y, Miura S, Fujino M, Imaizumi S, Karnik SS, Saku K. Clinical and pharmacotherapeutic relevance of the double-chain domain of the angiotensin II type 1 receptor blocker olmesartan. Clin Exp Hypertens. 2010;32(2):129–136. | |
Oparil S, Williams D, Chrysant SG, Marbury TC, Neutel J. Comparative efficacy of olmesartan, losartan, valsartan, and irbesartan in the control of essential hypertension. J Clin Hypertens (Greenwich). 2001;3(5):283–291. | |
Brunner HR, Stumpe KO, Januszewicz A. Antihypertensive efficacy of olmesartan medoxomil and candesartan cilexetil assessed by 24-hour ambulatory blood pressure monitoring in patients with essential hypertension. Clin Drug Investig. 2003;23(7):419–430. | |
Saito I, Kario K, Kushiro T, et al. Rationale, study design, baseline characteristics and blood pressure at 16 weeks in the HONEST Study. Hypertens Res. 2013;36(2):177–182. | |
Li P, Koike T, Jiang HY, Wang ZH, Kawata Y, Oshida Y. Acute treatment with candesartan cilexetil, an angiotensin II type 1 receptor blocker, improves insulin sensitivity in high-fructose-diet-fed rats. Horm Metab Res. 2012;44(4):286–290. | |
Benson SC, Pershadsingh HA, Ho CI, et al. Identification of telmisartan as a unique angiotensin II receptor antagonist with selective PPARgamma-modulating activity. Hypertension. 2004;43(5):993–1002. | |
Sezai A, Soma M, Hata M, et al. Effects of olmesartan on the renin-angiotensin-aldosterone system for patients with essential hypertension after cardiac surgery – investigation using a candesartan change-over study. Ann Thorac Cardiovasc Surg. 2011;17(5):487–493. | |
Furukawa T, Hatsuno T, Ueno Y, et al. Relationship between decrease in ambulatory blood pressure and heart rate variability due to the effects of taking olmesartan medoxomil. Clin Drug Investig. 2009;29(4):257–264. | |
Nakayama S, Watada H, Mita T, et al. Comparison of effects of olmesartan and telmisartan on blood pressure and metabolic parameters in Japanese early-stage type-2 diabetics with hypertension. Hypertens Res. 2008;31(1):7–13. | |
Ikeda H, Hamamoto Y, Honjo S, Nabe K, Wada Y, Koshiyama H. Olmesartan reduced microalbuminuria in Japanese subjects with type 2 diabetes. Diabetes Res Clin Pract. 2009;83(1):117–118. | |
Fukuda M, Yamanaka T, Mizuno M, et al. Angiotensin II type 1 receptor blocker, olmesartan, restores nocturnal blood pressure decline by enhancing daytime natriuresis. J Hypertens. 2008;26(3):583–588. | |
Shimada K, Ogihara T, Saruta T, Kuramoto K; REZALT Study Group. Effects of combination olmesartan medoxomil plus azelnidipine versus monotherapy with either agent on 24-hour ambulatory blood pressure and pulse rate in Japanese patients with essential hypertension: additional results from the REZALT study. Clin Ther. 2010;32(5):861–881. | |
Kario K, Hoshide S, Shimizu M, et al. Effect of dosing time of angiotensin II receptor blockade titrated by self-measured blood pressure recordings on cardiorenal protection in hypertensives: the Japan Morning Surge-Target Organ Protection (J-TOP) study. J Hypertens. 2010;28(7):1574–1583. | |
Mori H, Yamamoto H, Ukai H, et al; COMPATIBLE Study Group. Comparison of effects of angiotensin II receptor blocker on morning home blood pressure and cardiorenal protection between morning administration and evening administration in hypertensive patients: the COMPATIBLE study. Hypertens Res. 2013;36(3):202–207. | |
Daikuhara H, Kikuchi F, Ishida T. The combination of OLmesartan and a CAlcium channel blocker (azelnidipine) or candesartan and a calcium channel blocker (amlodipine) in type 2 diabetic hypertensive patients: the OLCA study. Diab Vasc Dis Res. 2012;9(4):280–286. | |
Nakanishi K, Nagai Y, Piao H, et al. Changes in renal vessels following the long-term administration of an angiotensin II receptor blocker in Zucker fatty rats. J Renin Angiotensin Aldosterone Syst. 2011;12(2):65–74. | |
Mancia G, Fagard R, Narkiewicz K, et al; Task Force Members. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7):1281–1357. | |
Yusuf S, Teo KK, Pogue J, et al; ONTARGET Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358(15):1547–1559. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.