")
Back to Journals » Patient Preference and Adherence » Volume 9
Design, construction, and implementation of an online platform for patients with type 1 diabetes: EncoDiab
Authors Alvarado-Martel D , Cañas F, Velasco R, Alcubierre N, López-Ríos L, Rius F, Nóvoa FJ, Carrillo A, Hernández M, Wägner AM , Mauricio D
Received 18 November 2014
Accepted for publication 8 January 2015
Published 15 June 2015 Volume 2015:9 Pages 767—775
DOI https://doi.org/10.2147/PPA.S77730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Dácil Alvarado-Martel,1,2,* Francesca Cañas,3,* Rebeca Velasco,1 Nuria Alcubierre,3 Laura López-Ríos,1,2 Ferran Rius,4 Francisco Javier Nóvoa,1,2 Armando Carrillo,1,2 Marta Hernández,3,4 Ana María Wägner,1,2,* Dídac Mauricio5,6,*
1Department of Endocrinology and Nutrition, Complejo Hospitalario Universitario Insular Materno-Infantil de Gran Canaria, Las Palmas, Spain; 2Instituto Universitario de Investigaciones Biomédicas y Sanitarias, Universidad de Las Palmas de Gran Canaria, Las Palmas, Spain; 3Department of Endocrinology and Nutrition, Institut de Recerca Biomèdica de Lleida (IRBLleida), Lleida, Spain; 4Department of Endocrinology and Nutrition, Hospital Universitari Arnau de Vilanova, Lleida, Spain; 5Hospital Universitari Germans Trias i Pujol, Badalona, Spain; 6Health Sciences Research Institute Germans Trias i Pujol, Badalona, Spain
*These authors contributed equally to this work
Purpose: The purpose of this study was to develop, build, and implement a virtual platform equipped with practical tools, relevant contents, and communication rooms, with the aim of facilitating patients’ self-management of type 1 diabetes mellitus (T1DM).
Materials and methods: The design of the platform was based on the suggestions of T1DM patients who were being managed at two reference hospitals. Patients’ needs and preferences were identified in group discussion sessions. Before having access to the platform, patients underwent a baseline assessment, which included physical examination and the administration of validated questionnaires for evaluation of clinical background, quality of life, treatment satisfaction, and well-being.
Results: A total of 33 patients were included in the study; 54.5% of them were men, their median age was 34 (18–50) years, the median duration of diabetes was 15 (1–38) years, and the median A1C was 7.4% (6%–12.6%). Based on their suggestions and requests, the online platform EncoDiab was built and organized into four domains: a personal domain, two domains shared by the patients and the staff of each of the two participating hospitals, and one domain that was accessible to all participants. The platform included practical tools (a body mass index calculator, a carbohydrate counting tool, and an insulin-dose calculator), a library with relevant information (documents on prevention and treatment of acute complications, nutrition, exercise, etc), and a chat room.
Conclusion: Although the study is still ongoing, our current results demonstrate the feasibility of building and implementing an online platform for helping T1DM patients in the self-management of their disease in the public health setting.
Keywords: eHealth, behavioral health, telehealth, education
Introduction
Tight glycemic control in type 1 diabetes mellitus (T1DM) reduces the risk of developing chronic complications of the disease.1 However, barriers preventing glycemic improvement can be found in the patient, in health care professionals, in the disease itself, and in the organization of health care services.2,3 Indeed, the daily management of the disease usually falls on the patient. Although providing an environment that facilitates diabetes self-management and allows for informed decision making is a challenge, it may contribute to improve the management of T1DM.4
Comanagement of this disease has already proved feasible.5,6 The aim of the present project was to shift the task of disease management and responsibility from health care professionals to patients themselves by providing high-quality resources to support them in self-management and informed decision making.
The incorporation of the Internet into our daily life has transformed the relationship between patients and health care professionals.7 Nowadays, “the web” is the most frequently consulted source of information on diseases. Nevertheless, the reliability of certain content is uncertain, and myths and lies are also spread efficiently.7 In the context of a reliable virtual environment, accurate information can be a powerful tool to support patients’ self-management of this disease, without the time and space limits of other resources.
New technologies can be used by health care professionals to assist patients in the management of diabetes. Actually, randomized controlled trials have shown that web-based support may have a positive impact on the process and quality of diabetes care, quality of life, and treatment satisfaction.8–10 Virtual interaction among patients with the same disease has not been rigorously assessed, but reports on discussion groups, chats, or a combination of these with news groups have been published.11 Most of them are run and promoted by health professionals, who stimulate discussion, propose or answer questions, or post useful pieces of news. A study analyzing patients’ perspectives highlighted the importance given to peer support, their awareness of the need to evaluate external information in each patient’s own context, and the value given to the experiential knowledge of other people with the same disease.12
The goal of this study was to design, build, and implement a virtual management system for patients with T1DM, in the public health care setting. It was conceived as a structure integrating information, education, assistance, and socialization. It followed the principles of the Web 2.0 philosophy, which enhances bidirectional communication and promotes adaptation of technological tools to the needs and skills of potential users. In the present article, we describe the design and implementation processes, as well as the baseline characteristics of the patients included in this study. The outcome of the use of the platform will be reported in the future.
Materials and methods
Study population and design
Participants were recruited among T1DM patients who were being treated at any of the two participating hospitals (Complejo Hospitalari Universitario Insular Materno-Infantil of Gran Canaria, Las Palmas, Spain and Hospital Universitari Arnau de Vilanova in Lleida, Spain). Inclusion criteria were: patients older than 18 years, T1DM diagnosed at least 1 year before, Internet connection at home, basic skills in the use of information and communications technology, and having an email account. Pregnant women and people with psychiatric or other conditions that could potentially interfere with follow-up were excluded. The study was approved by the Ethics Committees of both participating hospitals. Patients were contacted in the outpatient clinic, where they were offered a brief description of the study and invited to participate. Interested patients were appointed for a subsequent specific visit, where they were given detailed oral and written information and those wanting to participate were asked to sign an informed consent form. They were also asked to sign consent for potential promotional use of the pictures taken during the group sessions. Furthermore, the participants committed themselves to honor privacy and to act with mutual respect in the interactions within the platform.
In order to identify the patients’ needs and preferences, group sessions were organized, where participants were asked about the tools and contents they would like to find on an online platform. Indeed, one of the main goals of this project was that the patients themselves settled the basis for the design of the platform.
The 17 participants from the Complejo Hospitalario Universitario Insular Materno-Infantil of Gran Canaria were split into two groups, which took part in two parallel 2-hour group discussion sessions. Brainstorming was used to identify and record all the relevant aspects suggested by the participants,13 which were then ordered by priority (since it was assumed that covering all the recorded items within this project would not be feasible).
Participants from the Hospital Universitario Arnau de Vilanova in Lleida participated in 2-hour discussion sessions in two groups of eight subjects each. They were asked to discuss those aspects that would improve their quality of life and diabetes management. A sociology PhD student, who was in charge of designing the virtual environment, a diabetes nurse specialist (from the Lleida Patients Association), and the engineer in charge of the final platform design were present in the sessions and provided advice when needed.
Patients’ needs and suggestions identified in both hospitals were compiled into a common document, which was used as the basis for the design of the platform. The platform was built by using the content management system Drupal and adapted to the requirements of this type of system, as well as to those established by the patients. It was hosted on an independent dedicated server in compliance with the national regulations (law LO 15/1999 on the protection of personal data [LOPD] and RD 1720/2007, BOE-A-2008-979).
Patients
The initial population of the study included 33 patients (17 from Gran Canaria and 16 from Lleida): 54.5% of them were men; the median age was 34 (18–50) years; they had a median T1DM duration of 15 (1–38) years, a median A1C of 7.4% (6%–12.6%), and a median body mass index (BMI) of 24.6 (16.4–37.7 kg/m2); and 72.7% of them were workers, 24.2% were students, and 3% were homemakers. Table 1 shows their needs and suggestions as recorded during the group sessions.
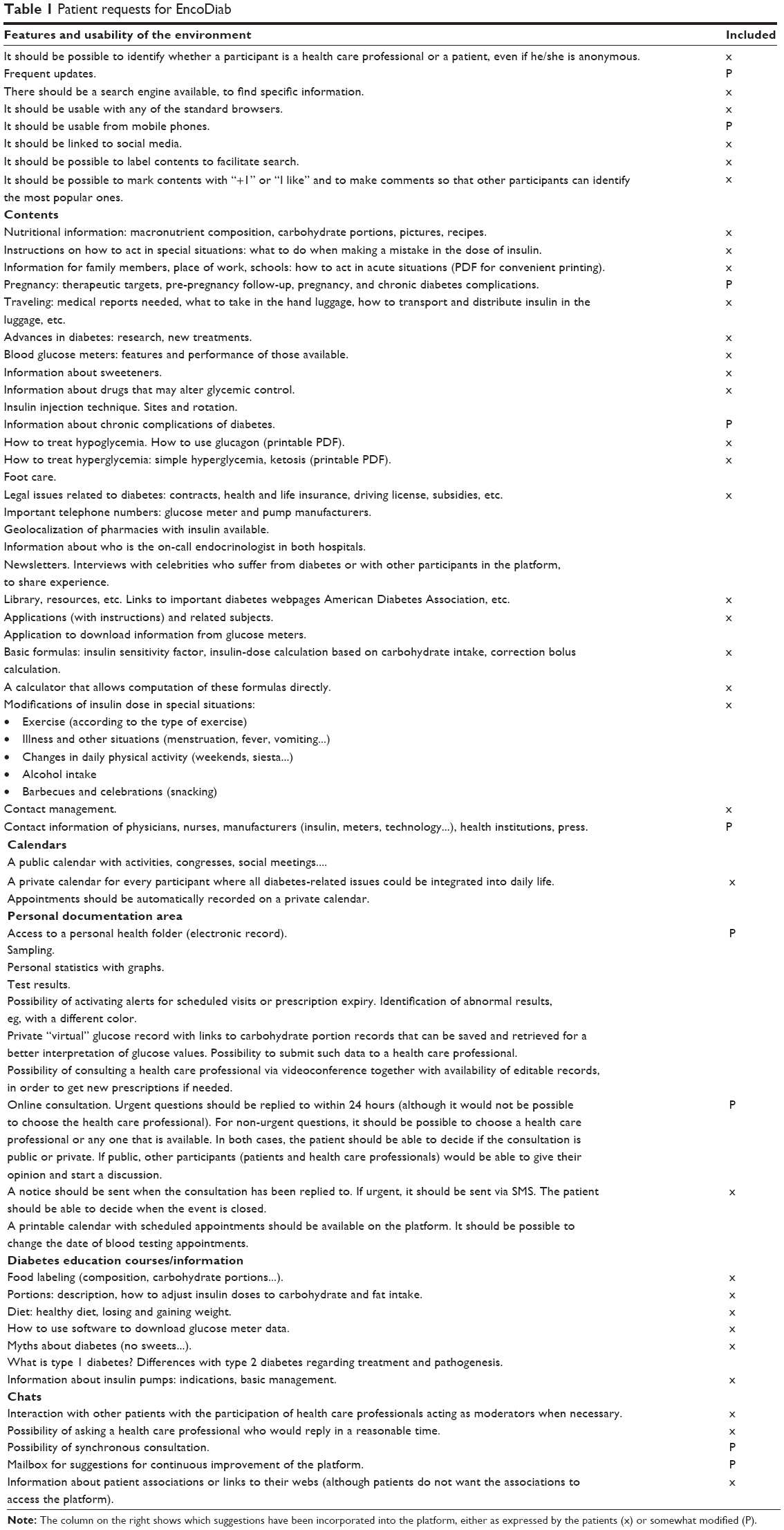 | Table 1 Patient requests for EncoDiab |
Implementation and evaluation
Six months after the initial group sessions, patients were appointed for a baseline evaluation visit, before being given access to the platform. Every participant received an email with their individual username and password to access the platform. There, they would find the contents and tools they had previously suggested and would be able to communicate with other participants and with health care professionals at their hospital.
During the baseline evaluation visit, information was collected on diabetes, possible associated complications, cardiovascular risk factors, and other possible diseases and treatments. Physical examination included blood pressure, anthropometric measurements, and foot examination. Blood samples were collected to measure A1C (high-performance liquid chromatography-National Glycohemoglobin Standardization Program standardized), lipids, kidney and liver assessment (colorimetry), thyroid-stimulating hormone (TSH), and albuminuria.
To evaluate quality of life and treatment satisfaction, the validated, Spanish versions of the following questionnaires were administered: Audit of Diabetes-Dependent Quality of Life,14 Diabetes Treatment Satisfaction Questionnaire,15 and 12-item Well-Being Questionnaire.16 In addition, each patient was asked to define up to three personal goals related to the platform, to be assessed during the follow-up.
All of these parameters were evaluated at baseline and again 12 months later. In addition, participants’ activity, use of resources, and permanence on the platform during the 6 months following their first access were quantified by using tools incorporated into the platform.
The platform EncoDiab was built progressively and did not include all of the patients’ suggestions from the start. At present, it is organized into four domains: a personal domain for every participant, one for interactions between the patients and health care professionals in Lleida, one for interactions between the patients and health care professionals in Gran Canaria, and one for general interactions among all participants.
Personal domains include: a customizable entry panel for profile editing, access to interactive tools (BMI calculator, glucose and insulin-dose register, carbohydrate portion calculator, and insulin-dose calculator), and activation of subscriptions to notifications. Figure 1 shows the BMI calculator, a simple tool in which patients can enter their weight and height and get their BMI as a result. A color code shows whether the BMI is healthy or not (green for normal, yellow for overweight, and red for obesity). Figure 2 shows the carbohydrate portion and insulin-dose calculator and Figure 3 shows the glucose and insulin-dose register, which can be submitted to a health care professional for evaluation. In addition, this domain includes an internal mail system for private one-to-one communication, a personal calendar (Figure 4), and access to other areas the participant is allowed to enter.
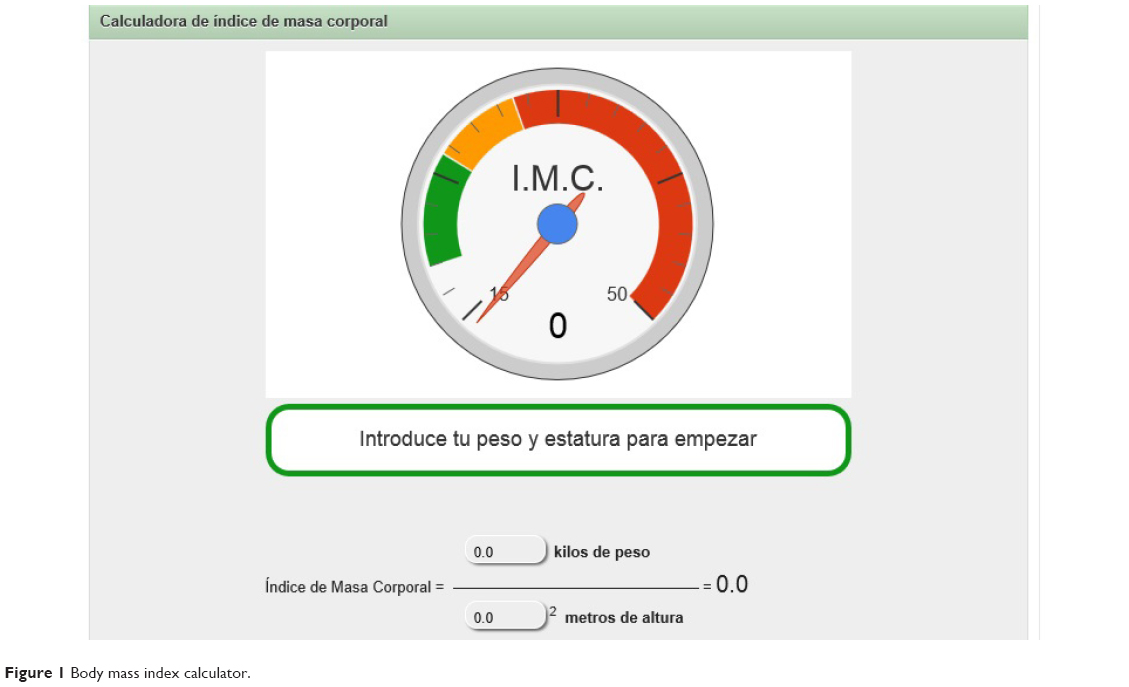 | Figure 1 Body mass index calculator. |
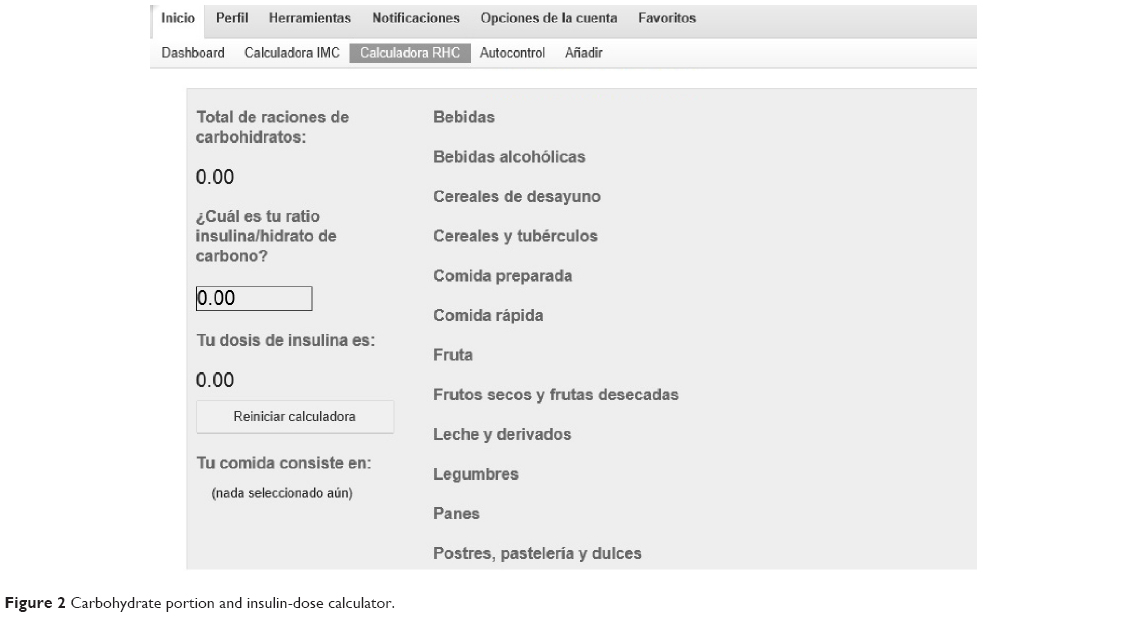 | Figure 2 Carbohydrate portion and insulin-dose calculator. |
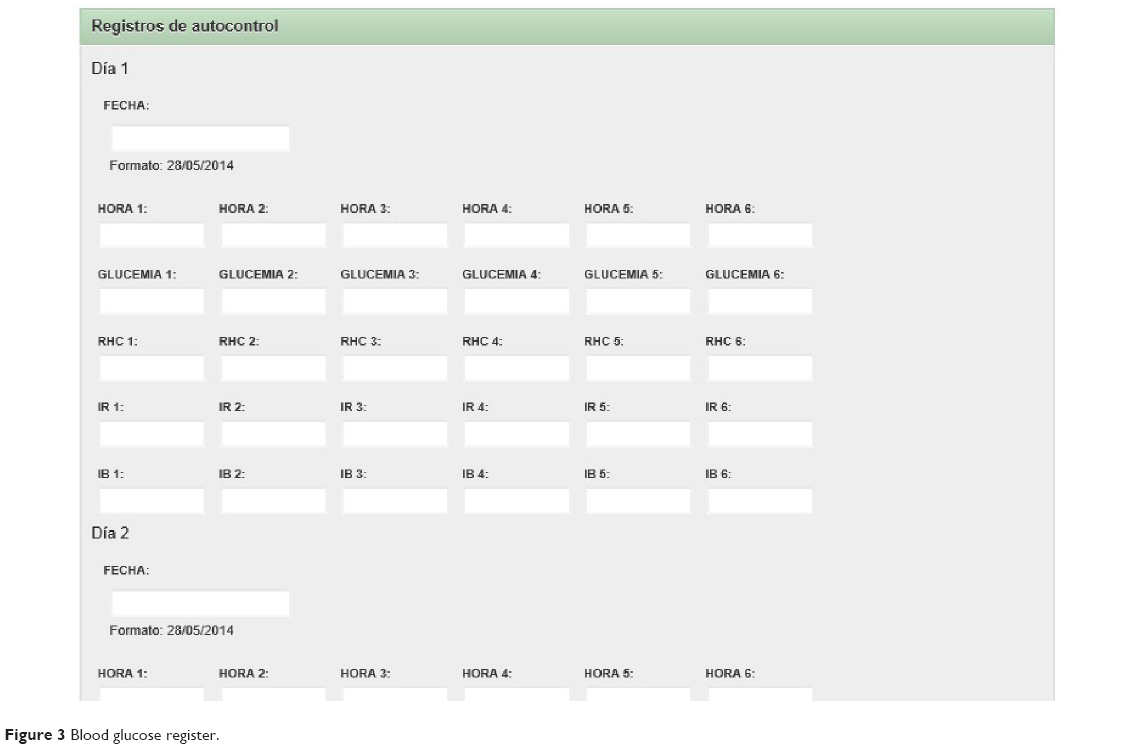 | Figure 3 Blood glucose register. |
 | Figure 4 Private calendar. |
The other domains are structured as follows: a customizable entry panel, a blog, a group calendar, a list of members allowed interaction in the domain, and a chat room. The library (Figure 5) contains a folder with recent commented articles, a section about physical exercise (how to start an exercise program, recommendations for insulin-dose adjustments, etc), a folder with legal information (subsidies), a folder with relevant health information (glucose meters, continuous glucose sensors, management of hypoglycemia and ketosis), a folder with documents on nutrition (general recommendations, links, food groups, healthy eating, frequently asked questions, recipes), selected links, and video tutorials about the use of the platform.
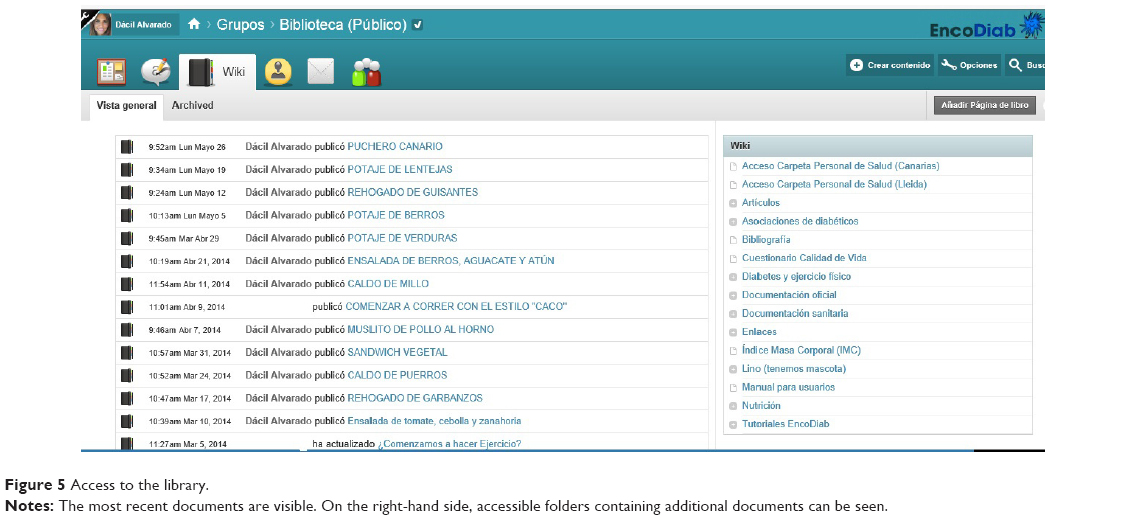 | Figure 5 Access to the library. |
There is also a discussion section, which was created with the aim of facilitating interaction among patients (Figure 6).
 | Figure 6 Patient discussion room. |
Validation group
Upon continuation of the project, 6 months after the start of the use of the platform, a new group of 29 patients (who did not participate in the design) has been given access to it after a baseline evaluation equivalent to that of the first group. This second group will be followed for 1 year. The details and results of this validation process will be published in the future.
Amplification of EncoDiab
A few months after the validation group was given access to the platform, it was also opened to other adults with T1DM who were interested. At the time of the present report, a total of 175 users are members of EncoDiab. An online questionnaire will be used to evaluate their satisfaction with the platform.
Discussion
T1DM has a huge impact on the lives of people who have the disease. Strategies aimed at empowering patients to manage it independently have proved to be effective.4 EncoDiab offers the tools for establishing a virtual community that facilitates communication among patients and with health care professionals. It provides practical tools for daily diabetes management and reliable information to support informed decision making. Above all, it is conceived as a place where patients play the leading role. This type of platform may offer other benefits, such as reducing isolation, promoting a positive psychological state, and acquiring healthy habits.17 Studies have shown that discussion forums and conversation rooms for interaction among patients who suffer from the same disease may have a positive effect on the participants, leading them to a more favorable disposition to control their disease.18 The availability of a reliable setting, with health professionals who offer advice and select and provide appropriate information, may empower patients to take responsibility for the control of their disease, have a positive effect on their level of commitment, and help them establish actions leading to better diabetes care.19 Other authors have reported the benefits of online platforms like EncoDiab, such as helping reduce communication barriers between patients and health care providers,20 which may eventually lead to improved self-care and self-management of disease.21 EncoDiab also facilitates peer support. Indeed, several studies have illustrated the importance of patient–health care provider communication22,23 and peer support in diabetes care.24
Previous studies on the effects of mobile tools, including web pages – which promote self-management and communication with health professionals – on T1DM patients, reported either improved glycemic control25 or no additional benefit when compared with conventional treatment.26,27
The development of EncoDiab was based on the participation of patients from the start, which is, in our opinion, the best way to design a system for such a close collaboration between providers and users. The early involvement of the users, even in the design of the platform, does not guarantee its success, but it should improve the odds. Indeed, the requests made by the participants in both centers (located in different and distant regions) were quite similar. Therefore, it is expected that the design of the platform would also meet the needs of other users. Although the analysis of the results is still in progress, the evaluation of the platform by its current users (more than 150) – only a minority being present from the start – is expected to provide further information about its generalizability.
Conclusion
The use of online resources for the self-management of health conditions is a necessity in communication and technology information society. Actually, self-management is being increasingly demanded by patients, and the public health system is expected to provide solutions. In T1DM in particular, self-care is a pivotal element, which could allow patients to live with high levels of independence from the health care team. To our knowledge, there is no previous evidence in our health care system on the feasibility, efficacy, or impact of a patient-centered, patient-designed online system like EncoDiab, which allows for comprehensive self-management of T1DM.
EncoDiab makes use of technology to complement standard diabetes education. Patients are provided with reliable online resources that can be accessed anytime from anywhere.
Since the study is ongoing, the analysis of the outcomes is still incomplete. The goal of this project was not focused on demonstrating the effectiveness of a telemedicine system, but on building, implementing, and evaluating a T1DM self-management system, based on patients’ requirements, in a real-world, public health care setting. Conclusions would be premature at this point. However, in case the goal of this project is finally achieved, it could lead not only to further optimization of T1DM self-management, but also to its possible application to other populations (pregnant women, children, and adolescents) or types of diabetes, especially the highly prevalent type 2 diabetes.
Acknowledgments
Dácil Alvarado-Martel is funded by a predoctoral fellowship (Agencia Canaria de Investigación, Innovación y Sociedad de la Información TESIS20120050). Nuria Alcubierre holds a predoctoral fellowship from Instituto de Salud Carlos III, FI11/0008. During the study, the authors received grants from the European Foundation for the Study of Diabetes (EFSD/JDRF/Novo Nordisk 2008 Programme for type 1 Diabetes) (AMW, JN) and the Instituto de Salud Carlos III (PI06/1104 [DM]; PI08/01113 [JN, AMW]; PI10/02310 [DAM, RV, AC, MHG, DM, AMW]; and PI11/02441 [AMW]).
Disclosure
The authors report no conflicts of interest in this work.
References
[No authors listed]. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329:977–986. | ||
Valenzuela JM, Seid M, Waitzfelder B, et al; SEARCH for Diabetes in Youth Study Group. Prevalence of and disparities in barriers to care experienced by youth with type 1 diabetes. J Pediatr. 2014;164:1369–1375. | ||
Wilkinson A, Whitehead L, Ritchie L. Factors influencing the ability to self-manage diabetes for adults living with type 1 or 2 diabetes. Int J Nurs Stud. 2014;51:111–122. | ||
Funnell MM, Anderson RM. Working toward the next generation of diabetes self-management education. Am J Prev Med. 2002;22:3–5. | ||
Goldberg HI, Ralston JD, Hirsch IB, Hoath JI, Ahmed KI. Using an Internet comanagement module to improve the quality of chronic disease care. Jt Comm J Qual Saf. 2003;29:443–451. | ||
Jennings A, Powell J, Armstrong N, Sturt J, Dale J. A virtual clinic for diabetes self-management: pilot study. J Med Internet Res. 2009;11:e10. | ||
Hartzband P, Groopman J. Untangling the Web – patients, doctors, and the Internet. N Engl J Med. 2010;362:1063–1066. | ||
Holbrook A, Thabane L, Keshavjee K, et al; COMPETE II Investigators. Individualized electronic decision support and reminders to improve diabetes care in the community: COMPETE II randomized trial. CMAJ. 2009;181:37–44. | ||
McCarrier KP, Ralston JD, Hirsch IB, et al. Web-based collaborative care for type 1 diabetes: a pilot randomized trial. Diabetes Technol Ther. 2009;11:211–217. | ||
Mulvaney SA, Rothman RL, Wallston KA, Lybarger C, Dietrich MS. An internet-based program to improve self-management in adolescents with type 1 diabetes. Diabetes Care. 2010;33:602–604. | ||
Eysenbach G, Powell J, Englesakis M, Rizo C, Stern A. Health related virtual communities and electronic support groups: systematic review of the effects of online peer to peer interactions. BMJ. 2004;328:1166. | ||
Armstrong N, Powell J. Patient perspectives on health advice posted on Internet discussion boards: a qualitative study. Health Expect. 2009;12:313–320. | ||
Osborn AF. Applied Imagination: Principles and Procedures of Creative Thinking. 3rd revised ed. Charles Scribner’s Sons; 1979. | ||
Bradley C, Todd C, Gorton T, Symonds E, Martin A, Plowright R. The development of an individualized questionnaire measure of perceived impact of diabetes on quality of life: the ADDQoL. Qual Life Res. 1998;8:79–91. | ||
Bradley C, editor. Diabetes Treatment Satisfaction Questionnaire (DTSQ). In: Handbook of Psychology and Diabetes: A Guide to Psychological Measurement in Diabetes Research and Practice. Switzerland: Harwood Academic Publishers; 1994:111–132. | ||
McMillan CV, Bradley C, Gibney J, Russell-Jones DL, Sönksen PH. Psychometric properties of two measures of psychological well-being in adult growth hormone deficiency. Health Qual Life Outcomes. 2006;4:16. | ||
Dennis CL. Peer support within a health care context: a concept analysis. Int J Nurs Stud. 2003;40:321–332. | ||
Zrebiec JF, Jacobson AM. What attracts patients with diabetes to an internet support group? A 21-month longitudinal website study. Diabet Med. 2001;18:154–158. | ||
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84:191–215. | ||
Bundesmann R, Kaplowitz SA. Provider communication and patient participation in diabetes self-care. Patient Educ Couns. 2011;85:143–147. | ||
Shaw RJ, Ferranti J. Patient-provider internet portals – patient outcomes and use. Comput Inform Nurs. 2011;29:714–720. | ||
Grey M, Whittemore R, Jeon S, Murphy K, Faulkner MS, Delamater A; TeenCope Study Group. Internet psycho-education programs improve outcomes in youth with type 1 diabetes. Diabetes Care. 2013;36:2475–2482. | ||
Nicholas DB, Gutwin C, Paterson B. Examining preferences for website support to parents of adolescents with diabetes. Soc Work Health Care. 2013;52:862–879. | ||
Donkin L, Christensen H, Naismith SL, Neal B, Hickie IB, Glozier N. A systematic review of the impact of adherence on the effectiveness of e-therapies. J Med Internet Res. 2011;13:e52. | ||
Peterson A. Improving type 1 diabetes management with mobile tools: a systematic review. J Diabetes Sci Technol. 2014;8(4):859–864. | ||
Esmatjes E, Jansà M, Roca D, et al; Telemed-Diabetes Group. The efficiency of telemedicine to optimize metabolic control in patients with type 1 diabetes mellitus: Telemed study. Diabetes Technol Ther. 2014;16:435–441. | ||
Suh S, Jean C, Koo M, et al. A randomized controlled trial of an internet-based mentoring program for type 1 diabetes patients with inadequate glycemic control. Diabetes Metab J. 2014;38:134–142. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.