")
Back to Journals » Orthopedic Research and Reviews » Volume 6
Current therapeutic approaches for plantar fasciitis
Authors Martinelli N, Bonifacini C, Romeo G
Received 15 November 2013
Accepted for publication 29 January 2014
Published 28 March 2014 Volume 2014:6 Pages 33—40
DOI https://doi.org/10.2147/ORR.S43126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Nicolò Martinelli, Carlo Bonifacini, Giovanni Romeo
Department of Ankle and Foot Surgery, IRCCS Galeazzi Orthopaedic Institute, Milan, Italy
Abstract: Almost 1 million Americans are affected by plantar fasciitis (PF), which is the commonest cause of chronic heel pain. This condition is often managed conservatively, and many rehabilitation protocols, some with the aid of orthoses, have been adopted, with good-to-excellent clinical results. Although most cases of chronic PF can be successfully managed with a conservative approach, alternative treatments, including high-energy shock wave therapy and corticosteroid injections, are commonly accepted as second-line treatment when traditional conservative therapy fails. However, surgery is still an important mode of treatment. Recently, new minimally invasive surgical techniques that offer numerous advantages (faster recovery time, early weight-bearing, lower postoperative pain) over standard surgical approaches have been proposed, with good results and low complication rates. The purpose of this review is to report new conservative and surgical techniques for the treatment of PF. A literature search for articles about plantar fasciitis was conducted on the PubMed database in order to identify publications addressing the treatments of PF. The literature suggests that, initially, traditional conservative treatments consisting of rest, oral nonsteroidal anti-inflammatory drugs, foot orthotics, and stretching exercises can be tried for several weeks. In patients with chronic recalcitrant PF, extracorporeal shock wave therapy or corticosteroid injection can be considered. Surgery (minimally invasive techniques) should be considered only after failure of the conservative treatments.
Keywords: heel pain, surgery, plantar fasciosis
Introduction
Plantar fasciitis (PF) is a common cause of heel pain seen by foot and ankle surgeons. Approximately 10%–16% of the US population suffers from PF, and approximately 75% of these patients turn to their family physician.1,2 The term “plantar fasciitis” has been used for years, but this term is misleading since inflammatory cells are rarely present in biopsies from involved fascias.3 Therefore, Lemont et al advocate the term “plantar fasciosis” to describe the syndrome characterized by pain along the proximal plantar fascia and its attachment in the area of the calcaneal tuberosity with impaired physical function, implying a more chronic degenerative process in comparison with acute heel pain.3 In literature, the term “plantar heel pain syndrome” has been used for patients with PF. We believe this term is too generic and should be used only for plantar heel pain. In this review, we will use the term “plantar fasciitis” to refer to the presentation of patients with plantar fasciopathy and facilitate the comparison between studies reported.
The plantar fascia is formed from collagen fibers that originate from the medial tuberosity of the calcaneus and insert into the dorsal aspect of the proximal phalanges and the flexor tendon sheaths.4 A number of studies have shown that the plantar fascia is involved in both the dynamic and static supports of the arch of the foot.5–8 During weight-bearing, stretching of the longitudinal arch is prevented by tension of the plantar fascia, muscles, and ligaments, with compression of the bones forming the arch itself.8 Continuity of the plantar fascia into the paratenon of the Achilles tendon has been shown in cadaver specimens, providing a positive correlation between Achilles tendon loading and plantar fascia tension.6 In cadaver studies, complete release of the plantar fascia decreased the height of the medial longitudinal arch during terminal stance as well as changed the distribution of plantar foot pressure, resulting in increased pressure on the central metatarsal heads.9–11
The etiology of PF is likely multifactorial. Numerous factors, including flatfoot, advancing age, obesity, inappropriate footwear, and decrease in ankle dorsiflexion, have been associated with plantar fascia disorders.12,13 While advancing age, which may induce plantar fascia degeneration and increased mechanical overload, is considered a risk factor for PF, the true pathogenesis remains unknown. A literature search for “articles about plantar fasciitis” was conducted on the PubMed database in order to identify publications addressing the current treatments of PF. Randomized clinical trials, case series, surveys, and narrative reviews written in English and published in peer-reviewed journals were included in this study. Although a more valid approach requires systematic search strategies, the intention of this review is to describe the current therapeutic approaches and the context in which future studies should be situated.
Clinical presentation
Patients with PF will complain of plantar heel pain, which is exacerbated with the first step after a period of non-weight-bearing, typically in the morning. In the early stages, patients will report that their symptoms improve after a few steps or minutes, but, in the chronic stages, pain becomes blunt and constant.14
The condition is generally self-limiting, and most of the cases spontaneously resolve regardless of the type of intervention received (including placebo). The painful symptoms usually spontaneously resolve within 10 months.14 However, in approximately 10% of patients, the disease progresses to chronic pain.14 Physical examination commonly reveals pain at palpation of the plantar fascia at the plantar aspect of the calcaneal tuberosity. Physical examination should, however, include the assessment of range of motion of the foot and ankle, focusing on limitation of ankle dorsiflexion, presence of hypesthesia or dysesthesia, and assessment of the forefoot/midfoot/hindfoot alignment. Passive ankle/first-toe dorsiflexion can cause discomfort or pain in the proximal plantar fascia and it can also cause painful tightness of the Achilles tendon. A fall from a height onto the heel may cause bone fractures involving the subtalar joint, the sustentaculum tali, the plantar calcaneal tubercles, or the inferior calcaneal spur. In most cases, diffuse pain in the hindfoot is poorly localized in the heel itself.15 A fracture is usually suspected with a history of trauma and focal pain at palpation. Acute plantar fascia rupture should be suspected in patients with a history of trauma and with negative radiographic and bone scan findings. Plantar swelling and ecchymosis of the heel are often present.16–18
Differential diagnosis
The differential diagnosis of plantar heel pain includes significant disorders, such as calcaneal stress fracture, systemic arthritides, entrapment neuropathies (eg, tarsal tunnel syndrome and medial plantar nerve entrapment), calcaneal infection, plantar calcaneal bursitis, or hindfoot osteoarthritis.19 Taking patient history, performing a physical examination of the foot and ankle, and ordering appropriate imaging studies, if indicated, are the first steps to making the correct diagnosis. A calcaneal stress fracture often develops from repetitive overload to the heel, and most commonly occurs when muscles become fatigued and are unable to absorb added shock. Patients experience heel pain after an increase in weight-bearing activity or change to a harder walking surface. The pain initially occurs only with activity, but often progresses to include pain at rest. Clinically, first examination may reveal swelling and stiffness associated with point tenderness at the fracture site immediately inferior and posterior to the posterior facet of the subtalar joint.19,20 Magnetic resonance imaging (MRI) allows evaluation of the extent of a stress fracture, as well as assessment of the ligamentous structures and plantar surface.20,21
Paresthesia presenting as burning, tingling, or numbness with chronic unilateral pain is indicative of neurologic heel pain due to nerve entrapment. These symptoms most commonly indicate a neuropathic etiology caused by overuse, trauma, obesity, venous insufficiency, or iatrogenic injury from previous surgery.22,23 Tarsal tunnel syndrome is the most commonly reported nerve entrapment due to compression of branches of the posterior tibial nerve, including the medial plantar nerve, the lateral plantar nerve, or the nerve to the abductor digiti minimi.22–25 Decreased heel pad elasticity with aging and increasing body weight may cause heel pad syndrome, which is often mistaken for PF. The syndrome is usually caused by inflammation, but damage to or atrophy of the heel pad can also elicit deep pain in the middle of the heel, which can be reproduced with firm palpation.26
Imaging
Plain weight-bearing radiographs of the foot represent the initial imaging study. Radiologic studies generally do not add additional diagnostic information, but they can exclude alternative causes of plantar heel pain or can be used in assessment of a failed treatment. A heel spur is often detected in radiographs of the foot; however, its presence may not necessarily correlate with the patient’s symptoms, since people without any symptoms can have this radiographic finding.27–30 Although ultrasonography and MRI are not the current imaging modalities of choice in patients with PF, they can provide useful information.31,32 Ultrasonography is an inexpensive diagnostic tool, which can be used to assess soft tissue pathology of the heel. Normal plantar fascia is hyperechoic and isoechoic with adjacent fat, with a thickness ranging from 2–4 mm.33 A thickening of the fascia greater than 4 mm and areas of hypoechogenicity can be observed in patients with plantar fasciopathy, which directly correlates with heel pain.13,34,35 Other signs of plantar fasciopathy include loss of definition and disorganization of the plantar fascia structure and peri-insertion edema.36 Ultrasound should also be used to identify the precise localization of corticosteroid injection within the plantar fascia and may be used as an objective measure of response to treatment in PF.37–39 Recently, Ieong at al reported the results of ultrasound evaluation in 125 consecutive feet with symptoms of chronic PF and concluded that distal involvement of the plantar fascia with atypical pattern (fusiform thickening of the plantar fascia distal to the insertion with normal appearance at the insertion site) is frequently observed.40 Therefore, the authors suggested the use of ultrasonographic examination in cases of recalcitrant plantar heel pain that have residual pain after conservative first-line management, in order to confirm the clinical diagnosis and to classify the disease as either insertional or noninsertional plantar fasciopathy (or mixed disease).40 MRI has been shown to differentiate between the various causes of heel pain, due to its ability to identify soft tissue and bony anatomy of the plantar aspect of the foot.41 In patients with PF, the commonest findings are perifascial and calcaneal bone edema with high signal intensity within the plantar fascia on T2 and short-tau inversion recovery images and thickening of the plantar fascia greater than 5 mm on T1 sequences.42 However, in patients with atypical chronic heel pain, osteoarthritic changes of hindfoot/midfoot joints, regional migratory osteoporosis, plantar arteriovenous malformation, and calcaneal stress fracture can be detected with MRI.43 The high cost of this exam should be taken into account, hence MRI is indicated only in patients with recalcitrant atypical heel pain. Other examinations, such as computerized tomography scanning, technetium-99m bone scan, nerve conduction velocity, and electromyography test, are indicated for those patients with a high index of suspicion for the other causes of heel pain.
Therapy
Nonoperative treatment
Conservative therapies remain the preferred approach to treating PF, successfully managing 85%–90% of cases (Table 1).44,45 A 2010 clinical practice guideline from the American College of Foot and Ankle Surgeons recommends conservative treatments, such as nonsteroidal anti-inflammatory drugs (NSAIDs), specific plantar fascia stretching, and orthotics for the initial management of plantar heel pain.46 Patients should be informed that it may take 6–12 months for symptoms to resolve. Patient-directed treatments to improve heel pain consist of rest, activity modification, ice, and acetaminophen or NSAIDs. A randomized placebo-controlled prospective study of NSAIDs to treat chronic PF showed short-term improvement in pain relief and disability when combined with other conservative treatments.47 However, there are few studies to support the benefits of these treatments used alone.
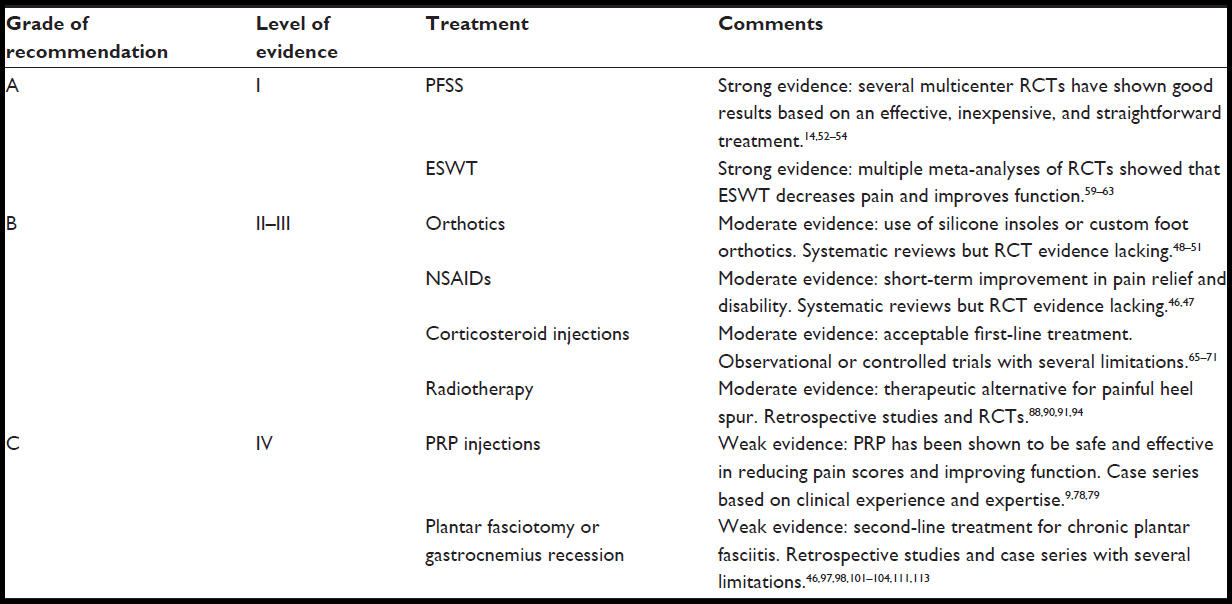 | Table 1 Evidence for management of plantar fasciitis |
The use of foot orthoses (prefabricated or custom-made) is considered the commonest approach in patients with PF.48 Orthoses theoretically unload the plantar fascia, reducing foot pronation. Because of the moderate expense, it is suggested that they should not be prescribed routinely to all patients but should be used instead in cases of abnormal foot posture (eg, flat feet). Lee et al performed a meta-analysis examining the effects of foot orthoses on self-reported pain and function in patients with PF and found that foot orthoses can decrease rear foot pain and improve foot function.49 A Cochrane Review found that custom foot orthotics may not help to reduce foot pain any more than prefabricated foot orthotics, but, when custom foot orthotics are used with an anterior night splint, patients may show higher pain relief.50 It is a generally held consensus that one or more of these options should be started prior to initiating any invasive treatments (level II evidence; Table 1). A recent paper reported good results with either full-length silicone insoles for patients with PF or an ultrasound-guided corticosteroid injection.51 Plantar fascia-specific stretching exercise has shown good results in the treatment of chronic PF.14,52–54 This approach for treatment of PF is simple and inexpensive; however, recommendations for the optimal duration and frequency of stretching exercises have not been unanimously established (Figure 1). The results, obtained from good experimental studies,14,52–54 suggest this treatment protocol for the treatment of chronic proximal PF. In a 2011 study, adding myofascial trigger-point manual therapy to a plantar fascia-specific stretching exercise routine improved self-reported pain and function when compared to stretching alone.55 However, due to the absence of a true control/sham/placebo group and long-term follow-up, the trigger-point release techniques cannot be considered effective in the treatment of heel pain.
Patients with severe pain when arising from bed in the morning can achieve benefits from the use of a night splint, which can provide a stretch lasting for many hours. Poor compliance should be taken into account, especially for patients with a low quality of nighttime bed rest.
Extracorporeal shock wave therapy (ESWT) has been used to treat different orthopedic disorders, including PF, shoulder calcific tendinitis, lateral epicondylitis, and Achilles tendinopathy.56–60 Shock waves used to treat PF are hypothesized to improve pain relief by promoting extracellular responses that cause neovascularization and angiogenesis leading to tissue repair and regeneration.61 Theoretically, patients with plantar fasciopathy with degeneration and calcific change (ie, calcaneal spur) may be successfully treated with a “stimulating” approach, such as ESWT. Rompe et al have previously reviewed the results of using focused shock wave therapy to treat chronic PF in a meta-analysis.62 Despite the heterogeneity between the studies included in their work (method of shock wave generation, amount of shock wave energy delivered, use of anesthesia, and outcome measure), the authors concluded that ESWT should be considered for the treatment of plantar fasciopathy when more common, accepted, and proven noninvasive treatments have failed. A 2012 review article concluded that most research shows that ESWT decreases pain and improves function in 34%–88% of patients with chronic PF.60 Dizon et al, in a more recent meta-analysis, combined the results of eleven studies on the effects of ESWT on PF and reported a decrease of pain and improved function in patients with chronic PF.63 Therefore, ESWT should be recommended as a remedial measure after failure of traditional conservative treatment and before surgical intervention. Recently, one study reported comparable results between high-energy ESWT and endoscopic plantar fasciotomy at short-term follow-up (1 year).64 However, larger randomized controlled studies are still needed to compare the curative effect of ESWT with surgery in the treatment of recalcitrant PF.
Corticosteroid injections have been used to treat multiple orthopedic diseases, including acute and chronic tendon pathologies.65,66 A single dexamethasone injection has been proven to reduce pain and improve function in patients with plantar fasciopathy.66–68 Additionally, the American College of Foot and Ankle Surgeons considers corticosteroid injections an acceptable first-line treatment for PF.46 Complications such as plantar fascia calcification, post-injection pain, fat pad atrophy, and plantar fascia ruptures should be taken into account.69–71
Steroid injection immediately after endoscopic surgery has been suggested to decrease postoperative fibrosis.71,72 Recently, promising clinical results have been reported with the use of platelet-rich plasma (PRP) injections for treating chronic muscle and tendon injuries.73–76 The rationale for using PRP is to promote cellular chemotaxis, matrix synthesis, and proliferation through higher than physiologic doses of reparative growth factors.77 PRP has been shown to be safe and effective in reducing pain scores and improving function in chronic PF.9,78 It can be argued that steroid injections, which decrease the inflammatory state of the tissue, are more successful in PF than in plantar fasciopathy. In a recent paper, Aks¸ahin et al compared the use of PRP injection with methylprednisolone injection, and both treatments were effective and successful in treating recalcitrant PF with no complications.79 Therefore, future randomized controlled trials are warranted to confirm or refute these findings. New conservative treatments have been proposed in recent years, including a micronized dehydrated human amniotic/chorionic membrane injection or botulinum toxin type A injection, with satisfactory results, but more studies are needed to include such protocols in the first-line approach for recalcitrant PF.80–85
Cast immobilization for 4–6 weeks or use of a short-leg walking boot to immobilize or offload the foot during activity has been proposed for recalcitrant PF, but the lack of prospective randomized studies precludes specific recommendations.86,87
A further modality for the treatment of painful PF is radiotherapy.88–92 Radiotherapy in nonmalignant disease is effective because the anti-inflammatory activity is mediated by a mechanism of downregulation of leukocyte adhesion and nitric oxide synthase activity in stimulated macrophages.93 In a retrospective study, Miszczyk et al reported lack of pain in 157 of 327 (48%) patients without a dose–response relationship.88 In a more recent multicenter randomized controlled trial on the effect of radiation therapy on PF, Niewald et al demonstrated that radiation therapy with 6.0 Gy doses applied in six fractions of 1.0 Gy twice weekly (standard dose) was highly significantly superior to low-dose radiation therapy (0.6 Gy applied in six fractions of 0.1 Gy twice weekly).94 Considering the lack of adverse effects, the simplicity of treatment, and the safe modality, radiotherapy seems to be an effective treatment for PF.
 | Figure 1 Plantar fascia specific stretching. |
Surgical treatment
Surgery should be considered only for patients who have not responded adequately after 6–12 months of conservative therapy.95 Surgery typically includes open plantar fasciotomy, resection of the heel spur (when present), and release of the abductor hallucis fascia.96,97 Complications of open surgery include residual pain (approximately 25% of patients will still experience heel pain); flatfoot deformity due to over-release of the plantar fascia; medial calcaneal nerve damage; and plantar tender scar.95 Several studies have investigated open plantar fasciotomy through a variety of approaches.98–100 Endoscopic plantar fascia fasciotomy, performed through a small skin incision, has been proven to achieve better results in comparison to traditional open surgery, and current practice suggests a minimally invasive approach to plantar fasciotomy versus extensive open surgical exposures.46,101–103 The use of endoscopic approaches in performing these procedures allows more rapid recovery and return to activity after surgery, with a low rate of complications (wound infection, residual pain). Patients undergoing surgery should expect a return to normal activity in approximately 2–3 months; however, patients should be informed about the possibility of complications such as residual pain.12,104 Further surgical approaches to relieving heel pain, which include radiofrequency ablation of the plantar fascia, radiofrequency nerve ablation, and cryosurgery, have shown good clinical results.105–109 Further studies to compare these new minimally invasive techniques with more traditional surgical approaches are warranted. Some authors suggest assessing the tightness of the Achilles tendon, since increased tension on the Achilles tendon is coupled with increased strain on the plantar fascia.110–112
Monteagudo et al, in a retrospective study, compared the results of open plantar fasciotomy with open gastrocnemius recession in the treatment of chronic PF.113 The authors concluded that proximal medial gastrocnemius release provides better clinical results than open fasciotomy with less incidence of complications and a higher satisfaction rate of the patients.113
Summary
PF is a common cause of chronic heel pain. In subjects at risk for PF, stretching exercises, weight loss, and changes in footwear may be effective preventive measures. Usually, first-line conservative treatment (including rest, NSAIDs, plantar fascia-specific stretching exercises, and orthoses) can successfully manage most cases of PF. Surgery (minimally invasive techniques) should be considered only after failure of the conservative treatments.
Disclosure
The authors report no conflicts of interest in this work.
References
Riddle DL, Schappert SM. Volume of ambulatory care visits and patterns of care for patients diagnosed with plantar fasciitis: a national study of medical doctors. Foot Ankle Int. 2004;25(5):303–310. | |
Riddle DL, Pulisic M, Pidcoe P, Johnson RE. Risk factors for plantar fasciitis: a matched case-control study. J Bone Joint Surg Am. 2003; 85-A(5):872–877. | |
Lemont H, Ammirati KM, Usen N. Plantar fasciitis: a degenerative process (fasciosis) without inflammation. J Am Podiatr Med Assoc. 2003;93(3):234–237. | |
Keener BJ, Sizensky JA. The anatomy of the calcaneus and surrounding structures. Foot Ankle Clin. 2005;10(3):413–424. | |
Arangio GA, Chen C, Salathé EP. Effect of varying arch height with and without the plantar fascia on the mechanical properties of the foot. Foot Ankle Int. 1998;19(10):705–709. | |
Stecco C, Corradin M, Macchi V, et al. Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. J Anat. 2013;223(6)665–676. | |
Hicks JH. The foot as a support. Acta Anat (Basel). 1955;25(1):34–45. | |
Salathé EP Jr, Arangio GA, Salathé EP. A biomechanical model of the foot. J Biomech. 1986;19(12):989–1001. | |
Martinelli N, Marinozzi A, Carnì S, Trovato U, Bianchi A, Denaro V. Platelet-rich plasma injections for chronic plantar fasciitis. Int Orthop. 2013;37(5):839–842. | |
Sharkey NA, Ferris L, Donahue SW. Biomechanical consequences of plantar fascial release or rupture during gait: part I – disruptions in longitudinal arch conformation. Foot Ankle Int. 1998;19(12)812–820. | |
Sharkey NA, Donahue SW, Ferris L. Biomechanical consequences of plantar fascial release or rupture during gait. Part II: alterations in forefoot loading. Foot Ankle Int. 1999;20(2):86–96. | |
Glazer JL. An approach to the diagnosis and treatment of plantar fasciitis. Phys Sportsmed. 2009;37(2):74–79. | |
Wearing SC, Smeathers JE, Sullivan PM, Yates B, Urry SR, Dubois P. Plantar fasciitis: are pain and fascial thickness associated with arch shape and loading? Phys Ther. 2007;87(8):1002–1008. | |
DiGiovanni BF, Nawoczenski DA, Lintal ME, et al. Tissue-specific plantar fascia-stretching exercise enhances outcomes in patients with chronic heel pain. A prospective, randomized study. J Bone Joint Surg Am. 2003;85-A(7):1270–1277. | |
Silver DA, Kerr PS, Atkins RM, Andrews HS. Fractures of the calcaneum. J Bone Joint Surg Br. 1993;75(5):838. | |
Pai VS. Rupture of the plantar fascia. J Foot Ankle Surg. 1996;35(1)39–40. | |
Theodorou DJ, Theodorou SJ, Kakitsubata Y, et al. Plantar fasciitis and fascial rupture: MR imaging findings in 26 patients supplemented with anatomic data in cadavers. Radiographics. 2000;20 Spec NoS181–S197. | |
Ahstrom JP Jr. Spontaneous rupture of the plantar fascia. Am J Sports Med. 1988;16(3):306–307. | |
Tu P, Bytomski JR. Diagnosis of heel pain. Am Fam Physician. 2011;84(8):909–916. | |
Aldridge T. Diagnosing heel pain in adults. Am Fam Physician. 2004;70(2):332–338. | |
Cassas KJ, Cassettari-Wayhs A. Childhood and adolescent sports-related overuse injuries. Am Fam Physician. 2006;73(6):1014–1022. | |
Schon LC, Glennon TP, Baxter DE. Heel pain syndrome: electrodiagnostic support for nerve entrapment. Foot Ankle. 1993;14(3):129–135. | |
Alshami AM, Souvlis T, Coppieters MW. A review of plantar heel pain of neural origin: differential diagnosis and management. Man Ther. 2008;13(2):103–111. | |
Peck E, Finnoff JT, Smith J. Neuropathies in runners. Clin Sports Med. 2010;29(3):437–457. | |
Labib SA, Gould JS, Rodriguez-del-Rio FA, Lyman S. Heel pain triad (HPT): the combination of plantar fasciitis, posterior tibial tendon dysfunction and tarsal tunnel syndrome. Foot Ankle Int. 2002;23(3):212–220. | |
Prichasuk S. The heel pad in plantar heel pain. J Bone Joint Surg Br. 1994;76(1):140–142. | |
Shama SS, Kominsky SJ, Lemont H. Prevalence of non-painful heel spur and its relation to postural foot position. J Am Podiatry Assoc. 1983;73(3):122–123. | |
Osborne HR, Breidahl WH, Allison GT. Critical differences in lateral X-rays with and without a diagnosis of plantar fasciitis. J Sci Med Sport. 2006;9(3):231–237. | |
Yozsa S, Lehnert B, Resnick D. Imaging of the rearfoot. J Am Podiatr Med Assoc. 1999;89(6):292–301. | |
DiMarcangelo MT, Yu TC. Diagnostic imaging of heel pain and plantar fasciitis. Clin Podiatr Med Surg. 1997;14(2):281–301. | |
Sabir N, Demirlenk S, Yagci B, Karabulut N, Cubukcu S. Clinical utility of sonography in diagnosing plantar fasciitis. J Ultrasound Med. 2005;24(8):1041–1048. | |
Timins ME. MR imaging of the foot and ankle. Foot Ankle Clin. 2000;5(1):83–101, vi. | |
Akfirat M, Sen C, Günes T. Ultrasonographic appearance of the plantar fasciitis. Clin Imaging. 2003;27(5):353–357. | |
Karabay N, Toros T, Hurel C. Ultrasonographic evaluation in plantar fasciitis. J Foot Ankle Surg. 2007;46(6):442–446. | |
McMillan AM, Landorf KB, Barrett JT, Menz HB, Bird AR. Diagnostic imaging for chronic plantar heel pain: a systematic review and meta-analysis. J Foot Ankle Res. 2009;2:32. | |
Gibbon WW, Long G. Ultrasound of the plantar aponeurosis (fascia). Skeletal Radiol. 1999;28(1):21–26. | |
Tsai WC, Wang CL, Tang FT, Hsu TC, Hsu KH, Wong MK. Treatment of proximal plantar fasciitis with ultrasound-guided steroid injection. Arch Phys Med Rehabil. 2000;81(10):1416–1421. | |
Tsai WC, Hsu CC, Chen CP, Chen MJ, Yu TY, Chen YJ. Plantar fasciitis treated with local steroid injection: comparison between sonographic and palpation guidance. J Clin Ultrasound. 2006;34(1):12–16. | |
Kane D, Greaney T, Shanahan M, et al. The role of ultrasonography in the diagnosis and management of idiopathic plantar fasciitis. Rheumatology (Oxford). 2001;40(9):1002–1008. | |
Ieong E, Afolayan J, Carne A, Solan M. Ultrasound scanning for recalcitrant plantar fasciopathy. Basis of a new classification. Skeletal Radiol. 2013;42(3):393–398. | |
Roger B, Grenier P. MRI of plantar fasciitis. Eur Radiol. 1997;7(9)1430–1435. | |
Grasel RP, Schweitzer ME, Kovalovich AM, et al. MR imaging of plantar fasciitis: edema, tears, and occult marrow abnormalities correlated with outcome. AJR Am J Roentgenol. 1999;173(3)699–701. | |
Chimutengwende-Gordon M, O’Donnell P, Singh D. Magnetic resonance imaging in plantar heel pain. Foot Ankle Int. 2010;31(10)865–870. | |
Gill LH. Plantar fasciitis: diagnosis and conservative management. J Am Acad Orthop Surg. 1997;5(2):109–117. | |
Martin RL, Irrgang JJ, Conti SF. Outcome study of subjects with insertional plantar fasciitis. Foot Ankle Int. 1998;19(12):803–811. | |
Thomas JL, Christensen JC, Kravitz SR, et al; American College of Foot and Ankle Surgeons heel pain committee. The diagnosis and treatment of heel pain: a clinical practice guideline-revision 2010. J Foot Ankle Surg. 2010;49(Suppl 3):S1–S19. | |
Donley BG, Moore T, Sferra J, Gozdanovic J, Smith R. The efficacy of oral nonsteroidal anti-inflammatory medication (NSAID) in the treatment of plantar fasciitis: a randomized, prospective, placebo-controlled study. Foot Ankle Int. 2007;28(1):20–23. | |
Roos E, Engström M, Söderberg B. Foot orthoses for the treatment of plantar fasciitis. Foot Ankle Int. 2006;27(8):606–611. | |
Lee SY, McKeon P, Hertel J. Does the use of orthoses improve self-reported pain and function measures in patients with plantar fasciitis? A meta-analysis. Phys Ther Sport. 2009;10(1):12–18. | |
Hawke F, Burns J, Radford JA, du Toit V. Custom-made foot orthoses for the treatment of foot pain. Cochrane Database Syst Rev. 2008;(3):CD006801. | |
Yucel U, Kucuksen S, Cingoz HT, et al. Full-length silicone insoles versus ultrasound-guided corticosteroid injection in the management of plantar fasciitis: a randomized clinical trial. Prosthet Orthot Int. 2013;37(6):471–476. | |
Digiovanni BF, Nawoczenski DA, Malay DP, et al. Plantar fascia-specific stretching exercise improves outcomes in patients with chronic plantar fasciitis. A prospective clinical trial with two-year follow-up. J Bone Joint Surg Am. 2006;88(8):1775–1781. | |
Hyland MR, Webber-Gaffney A, Cohen L, Lichtman PT. Randomized controlled trial of calcaneal taping, sham taping, and plantar fascia stretching for the short-term management of plantar heel pain. J Orthop Sports Phys Ther. 2006;36(6):364–371. | |
Cleland JA, Abbott JH, Kidd MO, et al. Manual physical therapy and exercise versus electrophysical agents and exercise in the management of plantar heel pain: a multicenter randomized clinical trial. J Orthop Sports Phys Ther. 2009;39(8):573–585. | |
Renan-Ordine R, Alburquerque-Sendín F, de Souza DP, Cleland JA, Fernández-de-Las-Peñas C. Effectiveness of myofascial trigger point manual therapy combined with a self-stretching protocol for the management of plantar heel pain: a randomized controlled trial. J Orthop Sports Phys Ther. 2011;41(2):43–50. | |
Furia JP. Safety and efficacy of extracorporeal shock wave therapy for chronic lateral epicondylitis. Am J Orthop (Belle Mead N J). 2005;34(1):13–19. | |
Furia JP. High-energy extracorporeal shock wave therapy as a treatment for insertional Achilles tendinopathy. Am J Sports Med. 2006;34(5):733–740. | |
Gerdesmeyer L, Wagenpfeil S, Haake M, et al. Extracorporeal shock wave therapy for the treatment of chronic calcifying tendonitis of the rotator cuff: a randomized controlled trial. JAMA. 2003;290(19)2573–2580. | |
Wang CJ, Wang FS, Yang KD, Weng LH, Ko JY. Long-term results of extracorporeal shockwave treatment for plantar fasciitis. Am J Sports Med. 2006;34(4):592–596. | |
Wang CJ. Extracorporeal shockwave therapy in musculoskeletal disorders. J Orthop Surg Res. 2012;7:11. | |
Buchbinder R, Ptasznik R, Gordon J, Buchanan J, Prabaharan V, Forbes A. Ultrasound-guided extracorporeal shock wave therapy for plantar fasciitis: a randomized controlled trial. JAMA. 2002;288(11)1364–1372. | |
Rompe JD, Furia J, Weil L, Maffulli N. Shock wave therapy for chronic plantar fasciopathy. Br Med Bull. 2007;81–82:183–208. | |
Dizon JN, Gonzalez-Suarez C, Zamora MT, Gambito ED. Effectiveness of extracorporeal shock wave therapy in chronic plantar fasciitis: a meta-analysis. Am J Phys Med Rehabil. 2013;92(7):606–620. | |
Radwan YA, Mansour AM, Badawy WS. Resistant plantar fasciopathy: shock wave versus endoscopic plantar fascial release. Int Orthop. 2012;36(10):2147–2156. | |
Paavola M, Kannus P, Järvinen TA, Järvinen TL, Józsa L, Järvinen M. Treatment of tendon disorders. Is there a role for corticosteroid injection? Foot Ankle Clin. 2002;7(3):501–513. | |
Landorf KB, Menz HB. Plantar heel pain and fasciitis. Clin Evid (Online). 2008;2008. | |
Schulhofer SD. Short-term benefits of ultrasound-guided corticosteroid injection in plantar fasciitis. Clin J Sport Med. 2013;23(1):83–84. | |
McMillan AM, Landorf KB, Gilheany MF, Bird AR, Morrow AD, Menz HB. Ultrasound guided corticosteroid injection for plantar fasciitis: randomised controlled trial. BMJ. 2012;344:e3260. | |
Fox TP, Oliver G, Wek C, Hester T. Plantar fascia calcification a sequelae of corticosteroid injection in the treatment of recalcitrant plantar fasciitis. BMJ Case Rep. 2013;2013. | |
Uden H, Boesch E, Kumar S. Plantar fasciitis – to jab or to support? A systematic review of the current best evidence. J Multidiscip Healthc. 2011;4:155–164. | |
Acevedo JI, Beskin JL. Complications of plantar fascia rupture associated with corticosteroid injection. Foot Ankle Int. 1998;19(2):91–97. | |
Kinley S, Frascone S, Calderone D, Wertheimer SJ, Squire MA, Wiseman FA. Endoscopic plantar fasciotomy versus traditional heel spur surgery: a prospective study. J Foot Ankle Surg. 1993;32(6):595–603. | |
Filardo G, Kon E, Della Villa S, Vincentelli F, Fornasari PM, Marcacci M. Use of platelet-rich plasma for the treatment of refractory jumper’s knee. Int Orthop. 2010;34(6):909–915. | |
Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, Rodeo SA. Platelet-rich plasma: from basic science to clinical applications. Am J Sports Med. 2009;37(11):2259–2272. | |
Monto RR. Platelet-rich plasma and plantar fasciitis. Sports Med Arthrosc. 2013;21(4):220–224. | |
Chew KT, Leong D, Lin CY, Lim KK, Tan B. Comparison of autologous conditioned plasma injection, extracorporeal shockwave therapy, and conventional treatment for plantar fasciitis: a randomized trial. PM R. 2013;5(12):1035–1043. | |
Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62(4):489–496. | |
Ragab EM, Othman AM. Platelets rich plasma for treatment of chronic plantar fasciitis. Arch Orthop Trauma Surg. 2012;132(8):1065–1070. | |
Aks¸ahin E, Doğruyol D, Yüksel HY, et al. The comparison of the effect of corticosteroids and platelet-rich plasma (PRP) for the treatment of plantar fasciitis. Arch Orthop Trauma Surg. 2012;132(6):781–785. | |
Díaz-Llopis IV, Gómez-Gallego D, Mondéjar-Gómez FJ, López-García A, Climent-Barberá JM, Rodríguez-Ruiz CM. Botulinum toxin type A in chronic plantar fasciitis: clinical effects one year after injection. Clin Rehabil. 2013;27(8):681–685. | |
Huang YC, Wei SH, Wang HK, Lieu FK. Ultrasonographic guided botulinum toxin type A treatment for plantar fasciitis: an outcome-based investigation for treating pain and gait changes. J Rehabil Med. 2010;42(2):136–140. | |
Babcock MS, Foster L, Pasquina P, Jabbari B. Treatment of pain attributed to plantar fasciitis with botulinum toxin a: a short-term, randomized, placebo-controlled, double-blind study. Am J Phys Med Rehabil. 2005;84(9):649–654. | |
Peterlein CD, Funk JF, Hölscher A, Schuh A, Placzek R. Is botulinum toxin A effective for the treatment of plantar fasciitis? Clin J Pain. 2012;28(6):527–533. | |
Zelen CM, Poka A, Andrews J. Prospective, randomized, blinded, comparative study of injectable micronized dehydrated amniotic/chorionic membrane allograft for plantar fasciitis – a feasibility study. Foot Ankle Int. 2013;34(10):1332–1339. | |
Elizondo-Rodriguez J, Araujo-Lopez Y, Moreno-Gonzalez JA, Cardenas-Estrada E, Mendoza-Lemus O, Acosta-Olivo C. A comparison of botulinum toxin a and intralesional steroids for the treatment of plantar fasciitis: a randomized, double-blinded study. Foot Ankle Int. 2013;34(1):8–14. | |
Tisdel CL, Harper MC. Chronic plantar heel pain: treatment with a short leg walking cast. Foot Ankle Int. 1996;17(1):41–42. | |
Pribut SM. Current approaches to the management of plantar heel pain syndrome, including the role of injectable corticosteroids. J Am Podiatr Med Assoc. 2007;97(1):68–74. | |
Miszczyk L, Jochymek B, Wozniak G. Retrospective evaluation of radiotherapy in plantar fasciitis. Br J Radiol. 2007;80(958):829–834. | |
Mücke R, Schönekaes K, Micke O, Seegenschmiedt MH, Berning D, Heyder R. Low-dose radiotherapy for painful heel spur. Retrospective study of 117 patients. Strahlenther Onkol. 2003;179(11):774–778. | |
Micke O, Seegenschmiedt MH; German Cooperative Group on Radiotherapy for Benign Diseases. Radiotherapy in painful heel spurs (plantar fasciitis) – results of a national patterns of care study. Int J Radiat Oncol Biol Phys. 2004;58(3):828–843. | |
Niewald M, Seegenschmiedt MH, Micke O, Gräber S; German Cooperative Group on the Radiotherapy for Benign Diseases of the DEGRO German Society for Radiation Oncology. Randomized multicenter trial on the effect of radiotherapy for plantar fasciitis (painful heel spur) using very low doses – a study protocol. Radiat Oncol. 2008;3:27. | |
Ott OJ, Jeremias C, Gaipl US, Frey B, Schmidt M, Fietkau R. Radiotherapy for calcaneodynia. Results of a single center prospective randomized dose optimization trial. Strahlenther Onkol. 2013;189(4):329–334. | |
Hildebrandt G, Seed MP, Freemantle CN, Alam CA, Colville-Nash PR, Trott KR. Mechanisms of the anti-inflammatory activity of low-dose radiation therapy. Int J Radiat Biol. 1998;74(3):367–378. | |
Niewald M, Seegenschmiedt MH, Micke O, et al; German Cooperative Group on Radiotherapy for Benign Diseases (GCGBD) of the German Society for Radiation Oncology (DEGRO). Randomized, multicenter trial on the effect of radiation therapy on plantar fasciitis (painful heel spur) comparing a standard dose with a very low dose: mature results after 12 months’ follow-up. Int J Radiat Oncol Biol Phys. 2012;84(4)e455–e462. | |
Neufeld SK, Cerrato R. Plantar fasciitis: evaluation and treatment. J Am Acad Orthop Surg. 2008;16(6):338–346. | |
Healey K, Chen K. Plantar fasciitis: current diagnostic modalities and treatments. Clin Podiatr Med Surg. 2010;27(3):369–380. | |
Morton TN, Zimmerman JP, Lee M, Schaber JD. A review of 105 consecutive uniport endoscopic plantar fascial release procedures for the treatment of chronic plantar fasciitis. J Foot Ankle Surg. 2013;52(1)48–52. | |
O’Malley MJ, Page A, Cook R. Endoscopic plantar fasciotomy for chronic heel pain. Foot Ankle Int. 2000;21(6):505–510. | |
Brekke MK, Green DR. Retrospective analysis of minimal-incision, endoscopic, and open procedures for heel spur syndrome. J Am Podiatr Med Assoc. 1998;88(2):64–72. | |
Hormozi J, Lee S, Hong DK. Minimal invasive percutaneous bipolar radiofrequency for plantar fasciotomy: a retrospective study. J Foot Ankle Surg. 2011;50(3):283–286. | |
Bader L, Park K, Gu Y, O’Malley MJ. Functional outcome of endoscopic plantar fasciotomy. Foot Ankle Int. 2012;33(1):37–43. | |
Urovitz EP, Birk-Urovitz A, Birk-Urovitz E. Endoscopic plantar fasciotomy in the treatment of chronic heel pain. Can J Surg. 2008;51(4):281–283. | |
Lundeen RO, Aziz S, Burks JB, Rose JM. Endoscopic plantar fasciotomy: a retrospective analysis of results in 53 patients. J Foot Ankle Surg. 2000;39(4):208–217. | |
Saxena A. Uniportal endoscopic plantar fasciotomy: a prospective study on athletic patients. Foot Ankle Int. 2004;25(12):882–889. | |
Liden B, Simmons M, Landsman AS. A retrospective analysis of 22 patients treated with percutaneous radiofrequency nerve ablation for prolonged moderate to severe heel pain associated with plantar fasciitis. J Foot Ankle Surg. 2009;48(6):642–647. | |
Cione JA, Cozzarelli J, Mullin CJ. A retrospective study of radiofrequency thermal lesioning for the treatment of neuritis of the medial calcaneal nerve and its terminal branches in chronic heel pain. J Foot Ankle Surg. 2009;48(2):142–147. | |
Weil L, Glover JP, Weil LS Sr. A new minimally invasive technique for treating plantar fasciosis using bipolar radiofrequency: a prospective analysis. Foot Ankle Spec. 2008;1(1):13–18. | |
Cavazos GJ, Khan KH, D’Antoni AV, Harkless LB, Lopez D. Cryosurgery for the treatment of heel pain. Foot Ankle Int. 2009;30(6)500–505. | |
Allen BH, Fallat LM, Schwartz SM. Cryosurgery: an innovative technique for the treatment of plantar fasciitis. J Foot Ankle Surg. 2007;46(2):75–79. | |
Cheung JT, Zhang M, An KN. Effect of Achilles tendon loading on plantar fascia tension in the standing foot. Clin Biomech (Bristol, Avon). 2006;21(2):194–203. | |
Abbassian A, Kohls-Gatzoulis J, Solan MC. Proximal medial gastrocnemius release in the treatment of recalcitrant plantar fasciitis. Foot Ankle Int. 2012;33(1):14–19. | |
Patel A, DiGiovanni B. Association between plantar fasciitis and isolated contracture of the gastrocnemius. Foot Ankle Int. 2011;32(1)5–8. | |
Monteagudo M, Maceira E, Garcia-Virto V, Canosa R. Chronic plantar fasciitis: plantar fasciotomy versus gastrocnemius recession. Int Orthop. 2013;37(9):1845–1850. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.