")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Comparison of outcomes of laparoscopic intracorporeal knotting technique in patients with complicated and noncomplicated acute appendicitis
Authors Ay N, Dinç B, Alp V, Kaya , Sevük U
Received 13 May 2015
Accepted for publication 8 July 2015
Published 12 August 2015 Volume 2015:11 Pages 1213—1216
DOI https://doi.org/10.2147/TCRM.S88479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Nurettin Ay,1 Bulent Dinç,2 Vahhac Alp,1 Şafak Kaya,3 Utkan Sevük4
1Department of General Surgery, Diyarbakir Gazi Yaşargil Training and Research Hospital, Diyarbakir, Turkey; 2Department of General Surgery, Ataturk State Hospital, Antalya, Turkey; 3Department of Infectious Disease, Diyarbakir Gazi Yaşargil Training and Research Hospital, Diyarbakir, Turkey; 4Department of Cardiovascular Surgery, Diyarbakir Gazi Yaşargil Training and Research Hospital, Diyarbakir, Turkey
Background and aim: In our study we aimed to compare laparoscopic intracorporeal knotting technique (base of the appendix was ligated with 20 cm of 2.0 silk) in patients with complicated acute appendicitis (CAA) and noncomplicated acute appendicitis.
Patients and methods: Ninety patients (female/male: 40/50, age ranging from 16 to 60 years, median age and interquartile range [IQR]: 25 [20; 32] years) who underwent laparoscopic appendectomy were included in the study. The patients were evaluated for the type of acute appendicitis, duration of operation, duration of hospital stay, and postoperative complications.
Results: The number of cases diagnosed as CAA was 28 (31.1%), and the number of noncomplicated cases was 62 (68.9%). We found that there was no significant difference in postoperative complication rates between complicated and noncomplicated appendicitis cases. Incision site infection was seen in seven cases (7.8%) and ileus was seen in two cases (2.2%). Bleeding, intra-abdominal abscess, and appendix stump leakage were not observed in any of the cases. Median and IQR duration of operation were 42 (35; 52) minutes and median and IQR duration of hospital stay were detected as 2 (1; 2) (range 1–10) days.
Conclusion: Laparoscopic intracorporeal knotting technique may be a safe, effective, and reliable technique as the materials needed for closing the appendix stumps are easily available for both CAA cases and noncomplicated cases.
Keywords: laparoscopic intracorporeal knotting technique, laparoscopic appendectomy, complicated acute appendicitis
Introduction
Laparoscopic appendectomy (LA) has found an increasingly wide range of applications since its first implementation in 1983. It has been demonstrated that LA is as much effective as open appendectomy in terms of postoperative wound site infection, analgesic requirement, duration of hospital stay, fast recovery, and early return to work.1–8
One of the most important phases of LA operation is the closure of appendix stump. The most commonly used methods for these are endostapler, extracorporeal sliding knots, endoloop, intracorporeal knotting, and endoclip.9–12 Although endostapler is an easy-to-use and reliable method, it is an expensive method.13 Although endoclips are affordable in terms of price, their usage is limited in cases with large appendix base.14
In our study, we aimed to compare laparoscopic intracorporeal knotting technique (LIKT) in patients with complicated acute appendicitis (CAA) and noncomplicated acute appendicitis (NCAA).
Patients and methods
Ninety patients (female/male: 40/50, age range: 16–60 years, median age and interquartile range [IQR]: 25 [20; 32] years) in whom LA was performed in our hospital between May 2012 and March 2015 were included in this study. The patients were evaluated for the type of complicated appendicitis, duration of operation, duration of hospital stay, and for postoperative complications. Informed consent was obtained from all patients who were included in the study. This study adheres to the principles of the Declaration of Helsinki 2008. Local ethics committee approval (Diyarbakir Education and Research Hospital, Diyarbakir, Turkey) was obtained for this retrospective study.
The cases with appendicular abscess, plastron appendicitis, periappendicular abscess, perforated appendicitis, and intra-abdominal abscess were evaluated as CAA.
LA has been performed in all AA cases, unless there is a contraindication. Antibiotic prophylaxis was given half an hour before the surgery. Antibiotic treatment has been continued in the postoperative period in case of the continuation of the infection. The operation was performed with classical 3 trocar technique. A suprapubic 5 mm, a left lower quadrant 10 mm, and one supraumbilical 10 mm trocars were used. Dissection with LigaSure™ is used only in CAA cases. After dissecting the mesoappendix, base of the appendix was ligated with LIKT once with 20 cm of 2.0 silk. Appendectomy was performed approximately 3 mm above the knot. Appendix is pulled out either with endo-bag or directly from the left lower quadrant trocar. Trocars were removed and closed after the abdomen was washed with saline solution. Drainage tube was used only in CAA cases. Statistical analyses were performed using the SPSS software version 16. Descriptive analyses were presented using median and IQR for the nonnormally distributed and ordinal variables. We compared CAA and NCAA using chi-square test (or Fisher’s exact test) and Mann–Whitney U-test. A P-value of less than 0.05 was considered to be statistically significant.
Results
The number of cases diagnosed as CAA was 28 (31.1%), and the number of NCAA cases was 62 (68.9%) (Figure 1). In the postoperative period, incision site infection was observed in seven cases (7.8%) and ileus was observed in two cases (2.2%). Incision site infection was observed at the supraumbilical trocar site and at the left lower quadrant site in one case. Bleeding, intra-abdominal abscess, and appendix stump leakage were not observed in any of the cases. Of the 28 cases diagnosed as CAA, incision site infection developed in three cases (10.7%) and ileus developed in two cases (7.1%). Incision site infection developed in four NCAA cases (6.4%). Incision site infection was treated with regular wound care and antibiotics and ileus was treated with bowel rest and fluid resuscitation. Median duration of operation and IQR were detected as 42 (35; 52) (range 26–100) minutes, and median duration of hospitalization and IQR were detected as 2 (1; 2) (range 1–10) days (Table 1).
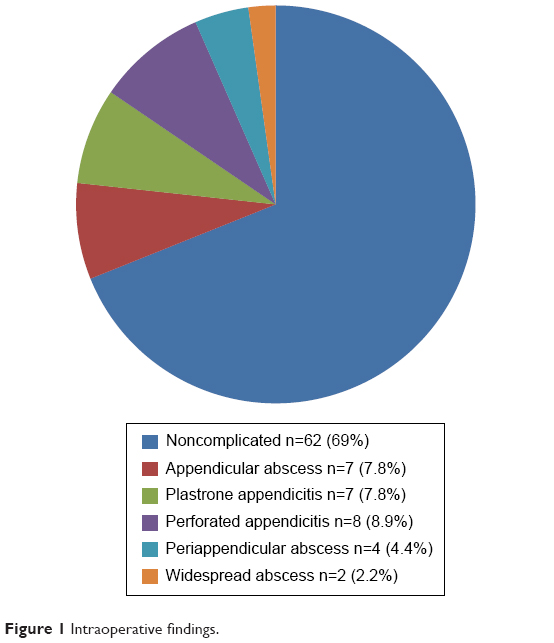 | Figure 1 Intraoperative findings. |
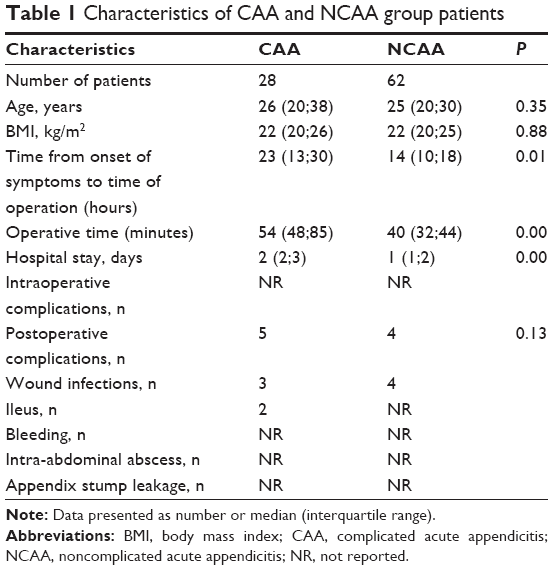 | Table 1 Characteristics of CAA and NCAA group patients |
Discussion
It has been demonstrated in our study that LIKT may be a safe, effective, and reliable technique with easily obtained materials for closing appendix stumps in CAA cases as in NCAA cases.
In LA, appendix stump is closed using methods such as endostapler, extracorporeal sliding knots, endoloop, intracorporeal knotting, and endoclip. In the study by Katsuno et al, they performed LA in 141 CAA cases and closed the appendix stump with 2/0 or 0/0 Polysorb™ suture or laparoscopic stapler. The mean duration of operation was detected as 116.7 minutes, and the mean duration of hospital stay was 8.9 days.15 In our 28 cases diagnosed with CAA and in whom LA was performed, the median duration of operation and IQR were 54 (48; 85) (range 32–100) minutes and median duration of hospital stay and IQR were detected as 2 (2; 3) days. Again, in the study of Katsuno et al, wound infection was detected as 6.4%, intra-abdominal abscess was 4.3%, and small-bowel obstruction was detected as 2.1%.15 In our study, wound site infection rate in CAA cases was found to be 10.7% and ileus rate as 7.1%. Postoperative intra-abdominal abscess was not observed in any of the cases. Ateş et al compared LIKT with titanium endoclip use for the closure of appendix stump in LA cases. The mean duration of operation was found to be 41.27 minutes in the endoclip group and 62.81 minutes in the knot-tying group.16 In our study including CAA and NCAA cases, the median duration of operation and IQR were detected as 42 (35; 52) minutes.
In a study with 100 patients, Rickert et al evaluated the reliability of titanium clips for the closure of appendix stump; intraoperational complication was not observed, mean duration of operation was 54 minutes, and the mean duration of hospital stay was detected as 4 days.17 Again in the same study, postoperative abdominal abscess, ileus, and wound site infections were observed in one patient for each. In our study, intraoperative complication and postoperative abdominal abscess were not observed in any of the cases. Ileus was observed in two cases (2.2%) and wound site infection was observed in seven cases (7.8%). Median duration of hospital stay and IQR were detected as 2 (1;2) days.
Postoperative appendix stump leakage or intra-abdominal abscess were not observed in any of the CAA and NCAA cases whose appendix stumps were closed by 2.0 silk and LIKT. As a result, LIKT may be a safe, effective, and reliable technique with easily obtained materials for closing the appendix stumps in CAA cases as well as in NCAA cases.
Disclosure
The authors report no conflicts of interest in this work.
References
Semm K. Endoscopic appendectomy. Endoscopy. 1983;15(2):59–64. | ||
Frazee RC, Roberts JW, Symonds RE, et al. A prospective randomized trial comparing open versus laparoscopic appendectomy. Ann Surg. 1994;219(6):728–731. | ||
Golub R, Siddiqui F, Pohl D. Laparoscopic versus open appendectomy: a meta-analysis. J Am Coll Surg. 1998;186(5):543–553. | ||
Hansen JB, Smithers BM, Schache D, Wall DR, Miller BJ, Menzies BL. Laparoscopic versus open appendectomy: prospective randomized trial. World J Surg. 1996;20(1):17–20. | ||
Temple LK, Litwin DE, McLeod RS. A meta-analysis of laparoscopic versus open appendectomy in patients suspected of having acute appendicitis. Can J Surg. 1999;42(5):377–383. | ||
Korndorffer JR Jr, Fellinger E, Reed W. SAGES guideline for laparoscopic appendectomy. Surg Endosc. 2010;24(4):757–761. | ||
Heikkinen TJ, Haukipura K, Hulkko A. Cost-effective appendectomy: open or laparoscopic? A prospective, randomized study. Surg Endosc. 1998;12(10):1204–1208. | ||
Reiertsen O, Larsen S, Trondsen E, Edwin B, Faerden AE, Rosseland AR. Randomized controlled trial with sequential design of laparoscopic versus conventional appendectomy. Br J Surg. 1997;84(6): 842–847. | ||
Hanssen A, Plotnikov S, Dubois R. Laparoscopic appendectomy using a polymeric clip to close the appendicular stump. JSLS. 2007;11(1): 59–62. | ||
Beldi G, Vorburger SA, Bruegger LE, Kocher T, Inderbitzin D, Candinas D. Analysis of stapling versus endoloops in appendiceal stump closure. Br J Surg. 2006;93(11):1390–1393. | ||
Moreno M, Magos FJ, Arcovedo R, et al. Comparison of the performance of the Gea extracorporeal knot with the Roeder extracorporeal knot and the classical knot. Surg Endosc. 2004;18(1):157–160. | ||
Delibegović S, Matović E. Hem-o-lok plastic clips in securing of the base of the appendix during laparoscopic appendectomy. Surg Endosc. 2009;23(12):2851–2854. | ||
Kazemier G, in’t Hof KH, Saad S, Bonjer HJ, Sauerland S. Securing the appendiceal stump in laparoscopic appendectomy: evidence for routine stapling? Surg Endosc. 2006;20(9):1473–1476. | ||
Patrecke LI, Kessler W, von BW, Diedrich S, Heidecke CD, Patrzyk M. Laparoscopic appendectomy using a single polymeric clip to close the appendicular stump. Langenbecks Arch Surg. 2010;395(8): 1077–1082. | ||
Katsuno G, Nagakari K, Yoshikawa S, Sugiyama K, Fukunaga M. Laparoscopic appendectomy for complicated appendicitis: a comparison with open appendectomy. World J Surg. 2009;33(2):208–214. | ||
Ateş M, Dirican A, Ince V, Ara C, Isik B, Yilmaz S. Comparison of intracorporeal knot-tying suture (polyglactin) and titanium endoclips in laparoscopic appendiceal stump closure: a prospective randomized study. Surg Laparosc Endosc Percutan Tech. 2012;22(3):226–231. | ||
Rickert A, Bönninghoff R, Post S, Walz M, Runkel N, Kienle P. Appendix stump closure with titanium clips in laparoscopic appendectomy. Langenbecks Arch Surg. 2012;397(2):327–331. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.