")
Back to Journals » International Journal of Women's Health » Volume 6
Comparison of domestic violence against women in urban versus rural areas of southeast Nigeria
Authors Ajah L , Iyoke CA , Nkwo PO, Nwakoby B, Ezeonu P
Received 7 July 2014
Accepted for publication 13 August 2014
Published 8 October 2014 Volume 2014:6 Pages 865—872
DOI https://doi.org/10.2147/IJWH.S70706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
Leonard Ogbonna Ajah,1,2 Chukwuemeka Anthony Iyoke,1 Peter Onubiwe Nkwo,1 Boniface Nwakoby,3 Paul Ezeonu2
1Department of Obstetrics and Gynaecology, University of Nigeria Teaching Hospital, Enugu, Nigeria; 2Department of Obstetrics and Gynaecology, Federal Teaching Hospital, Abakaliki, Ebonyi State, Nigeria; 3Department of Community Medicine, University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu, Nigeria
Background: The perception and prevalence of domestic violence (DV) in rural areas is poorly understood; the result is that most efforts at eradicating this harmful practice are concentrated in urban areas. The objective of the study was to compare the burden and perception of DV among women living in rural and urban Igbo communities of southeast Nigeria.
Methods: This was a comparative, cross-sectional study of women residing in rural and urban communities in Enugu, Nigeria, who had gathered for an annual religious meeting from August 1–7, 2011. Data analysis involved descriptive and inferential statistics and was conducted with the Statistical Package for Social Sciences, software version 17.0, at a 95% level of confidence.
Results: A total of 836 women who met the eligibility criteria participated in the survey. Of these, 376 were from Okpanku, a rural community, while 460 were from Ogui Nike, an urban community. The prevalence of DV among rural women was significantly higher than that among urban women (97% versus 81%, P<0.001). In particular, the prevalence of physical violence was significantly higher among rural women than among urban women (37.2% versus 23.5%; P=0.05). In contrast, rural and urban women did not differ significantly in the proportions that had experienced psychological or sexual violence. The proportion of women who believed that DV was excusable was significantly higher among rural dwellers than among urban dwellers (58.5% versus 29.6%; P=0.03).
Conclusion: The burden of DV against women may be higher in rural communities than in urban communities in southeast Nigeria. More rural women perceived DV as excusable; this finding suggests that factors that sustain DV could be strong in rural areas. A comprehensive program to curb DV in this area may need to significantly involve the rural areas.
Keywords: prevalence, perception, domestic violence, rural, urban
Introduction
Domestic violence (DV) against women refers to any type of harmful behavior directed at either a woman or a girl by her significant other, such as her spouse.1,2 It is the most common form of violence against women.3 DV can take various forms. It can be in the form of physical, verbal, or sexual violence, or it can be the threat of such an act.4,5 DV can also be in the form of coercion or of arbitrary deprivation of liberty, and it can occur in public or private life.5,6 An emerging dimension to the problem of DV against women in South East Nigeria is the use of acid baths by men to punish women or girls for various perceived offences.7
DV cuts across ages, ethnicity, religion, and educational barriers.1 The lifetime risk of physical violence, sexual violence, or both varied from 15%–71% in many countries.8 DV has been associated with psychiatric illnesses such as depression, anxiety, posttraumatic stress disorder, and suicide.9,10 Low socioeconomic and educational status, early marriage, alcohol and substance abuse by the partner, and unemployment have been suggested as risk factors for DV.4,11 Most countries and religions frown at DV, but because some cultures seem to condone it, the problem has persisted.5,12 In addition, DV is still underreported partly because of the culture of concealment in some societies.13,14
DV against women could be associated with significant morbidity, which could occasionally result in mortality. The World Health Organization (WHO), International Federation of Gynaecoloy and Obstetrics, and the Nigeria National Reproductive Health Policy recognize the scourge of violence against women, and these organizations have various declarations on the elimination of violence against women.5,15,16
DV is a prevalent public health problem in Nigeria.17–20 Its prevalence in Nigeria ranges between 17% and 78.8%, with considerable regional variation.12–14,17–22 Most of the previous studies on DV in Nigeria were based in urban hospitals or urban communities. Little is known about the prevalence of DV in rural communities in Nigeria and how it is perceived there, and there are few studies that have made a direct comparison between urban and rural women. The aim of this study was to compare the burden and perception of DV against women between women in a rural Igbo community in southeast Nigeria and women in an urban community in the same area.
Methods
Study area
Enugu State is one of the states in the southeast geopolitical zone of Nigeria. The state shares borders with Abia and Imo States to the south, Ebonyi State to the east, Benue State to the northeast, Kogi State to the northwest, and Anambra State to the west. The state is predominantly rural and agrarian, with a substantial proportion of its working population engaged in subsistence farming. Enugu has a population of 3.3 million people, and it has 17 local government areas (LGAs).
The study communities were Okpanku in the Aninri LGA and Ogui Nike in the Enugu East LGA.23,24 Aninri is a rural LGA, and all of the component communities are inhabited mostly by subsistence farmers. Some women in these communities are farmers, and many are housewives. In contrast, Enugu East is an urban LGA at the heart of the city of Enugu. The residents of Ogui Nike come from different parts of the state and country and include civil servants, teachers, traders, artisans, as well as people in other professions. Women living in this area are substantially involved in these occupations.
August meeting
The August meeting refers to an annual gathering of women belonging to the Christian religion in each community in southeast Nigeria in the month of August. The purpose of the gathering is to promote prayer, Christian virtues, and enlightenment across a broad range of issues among women. For these purposes, activities during August meetings usually include talks and discussions about such areas as female education, women’s health, women’s rights, as well as the participation of women in the development of the church. It has become an important event in the calendars of the churches in southeast Nigeria, where over 90% of the people are Christians.24 The August meeting is very popular and is considered mandatory among some residents. Anecdotal evidence suggests that over 80% of Christian women attend. However, it is possible that a small proportion of men prohibit their wives from attending the August meeting. Activities during the August meeting are entirely organized and conducted by women themselves under the guidance of the clergy. Men can be invited to give talks in any area chosen by the women. August meetings in many communities have witnessed events like health advocacy, free medical consultations, and screening for various medical conditions.
Study design
This was a cross-sectional, comparative study.
Study population
The study population included all women attending the annual August meeting in one rural community, Okpanku, and in one urban community, Ogui Nike, Enugu.
Study period
The study took place in Okpanku from August 1–7, 2011 and in Ogui Nike from August 8–14, 2011.
Sampling
The sampling technique used was multistage sampling. During the first stage, a random Aninri local government was selected from a bag containing all the names of the eleven rural LGAs in the state of Enugu, and a random Enugu North LGA was selected from a bag containing all the names of the six urban LGAs. The second stage involved the random selection of Okpanku from a bag containing the names of all of the communities in the Aninri LGA; the second stage also involved the random selection of Ogui Nike from a bag containing the names of all of the communities in the Enugu North LGA. During the third stage, the list of all of the participants in the August meeting in Okpanku was used as a sampling frame to systematically draw a random sample of women from that region. Similarly, the list of participants in the Ogui Nike August meeting was used to draw a random sample from that community. For each list of participants, a random start was made, and subsequent samples were selected by selecting every third name on the list.
Data collection
The WHO Violence Against Women Instrument, developed for use in the WHO Multi-country Study on Women’s Health and Domestic Violence against Women, was used for this study. The questions used in this study, questions 703–706 from section 7 of the WHO study questionnaire, were incorporated with modifications to adapt the questions to our environment.25 In this respect, we inserted the words “or relations of your partner” into the questions. This is to reflect the high influence of the husband’s relatives in marriage arrangements in the Igbo land.18 We also included “refusal to eat food prepared by partner” and “not coming home to partner” under question 704. This is to reflect a common way that men punish women in the Igbo culture.18 Finally, we left off the determination of the severity of violence by excluding the number of times violence occurred. This was done to reduce recall bias in the study. The questionnaires assessed the experiences of DV over the period of 3 years preceding the study. Administration of the questionnaires was carried out by trained female research assistants. The research assistants were people from the study institution; they did not know and were unknown to the respondents. Women were called aside and interviewed separately, either during or at the end of each day’s activities. The questionnaire was self-administered among women who were literate enough to understand the questions. For women who were not sufficiently literate, the questionnaire was interviewer-administered. For semiliterate or illiterate women, research assistants translated the questions into the Igbo language and transcribed answers that were given in the Igbo language into English. The operational definitions of violence were based on the WHO study and have been outlined in Table S1.
Inclusion criteria
Women were included in the study if they had lived in either the urban or rural community for up to 3 years preceding the study. Such women were to be within the age range of 15–49 years and they must have provided their written consent to participate in the study.
Exclusion criteria
Women were excluded from the study if they were younger than 15 years of age or older than 49 years of age, had resided in either the urban or the rural community for less than 3 years, or had refused consent to participate in the study.
Data analysis
The results were analyzed with the Statistical Package for the Social Sciences version 17.0 for Windows. Comparisons were done between the proportions of rural women and those of urban women in the following types of categories: sociodemographic groups; groups that experienced DV; groups based on the perception of DV; and groups based on the reaction to DV. The chi-square test was used to assess differences between the proportions of rural women and of urban women in groups based on either their experience of DV or their perception of it. Values of P≤0.05 were considered statistically significant.
Ethical clearance
The study was approved by the research ethics committee of the University of Nigeria Teaching Hospital, Enugu, Nigeria.
Results
A total of 836 women who met the eligibility criteria participated in the study. Of these, 376 were from Okpanku (a rural community), while 460 were from Ogui Nike (an urban community). The mean ages of rural and urban women were 33.3 years and 30.9 years, respectively. Table 1 shows the comparisons of the sociodemographic characteristics of the study participants. It shows that the proportions of urban and rural women in the age groups between 15 years and 44 years did not differ significantly. Similarly, there were no significant differences in the proportions of rural and urban women in the marital status groups. Rural women were significantly less educated, were less likely to be employed, had higher parity, had higher numbers of living children, and had more polygamous marital relationships.
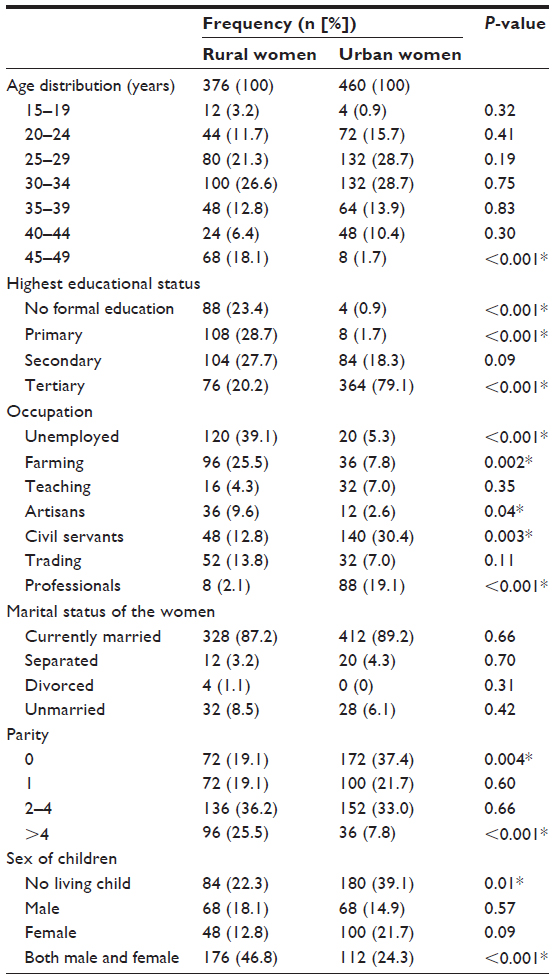 | Table 1 Comparison of the sociodemographic characteristics of respondents |
Of the rural women, 364 out of a total of 376 who participated in the study had experienced DV; of the urban women, 372 out of a total of 460 experienced DV. The difference in the proportions of rural and urban women who had experienced DV was statistically significant (96.8% versus 80.9%, respectively; P<0.001). Among those who experienced physical violence, 140 were rural women, while 108 were urban women. The proportion of rural women who had experienced physical violence was significantly higher than that of the urban women (37.2% versus 23.5%, respectively; P=0.05). In contrast, there was no statistically significant difference between the proportions of rural and urban women who had experienced psychological violence (58.0% versus 53.0%, respectively; P=0.50) or sexual violence (6.4% versus 4.3%, respectively; P=0.21). Table 2 shows a comparison of the types and periods of occurrence of DV between the two study communities.
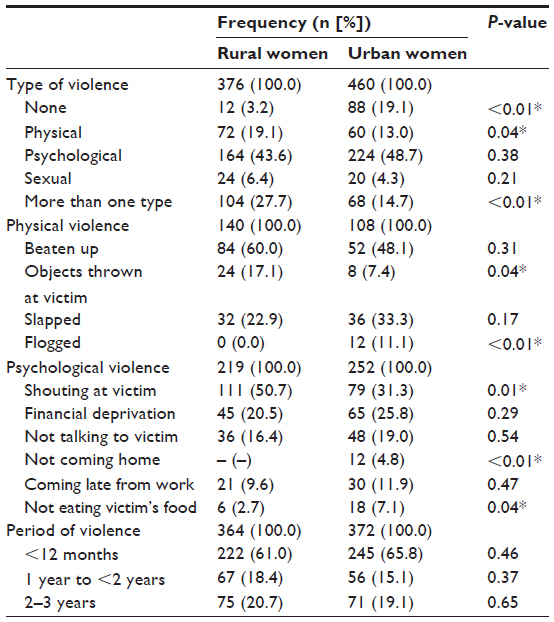 | Table 2 Comparison of types and periods of domestic violence |
Table 3 shows a comparison of the sociodemographic characteristics of the reported perpetrators of DV. The proportion of perpetrators of DV who were farmers was significantly higher in the rural community when compared to that of the urban community. Perpetrators of DV in the rural community tended to be less educated compared to perpetrators in the urban community; the proportion of perpetrators who completed tertiary education was significantly lower in the rural sample than in the urban sample.
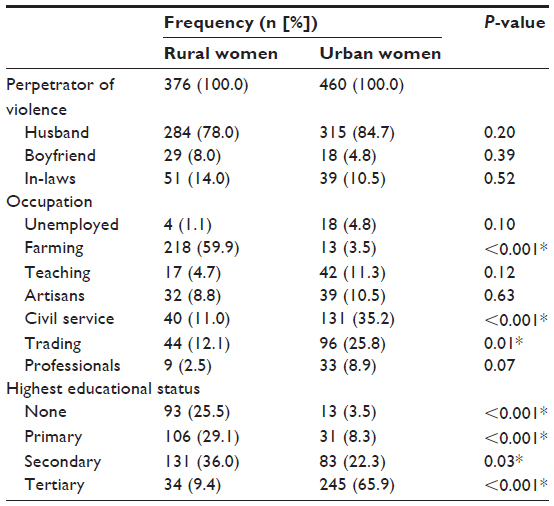 | Table 3 Comparison of the sociodemographic characteristics of reported perpetrators of domestic violence |
Table 4 shows a comparison of the perception of DV by respondents. The proportion of women who believed that DV was sometimes excusable was significantly higher in the rural community than in the urban community (58.5% versus 29.6%, respectively; P=0.03). A significantly higher proportion of rural women believed that going out without telling their partners or neglecting to care for their children could justify DV, while a significantly higher proportion of urban women believed that refusing sex could justify DV. Whereas a higher proportion of rural women would report DV to their families compared to urban women (50.5% versus 18.3%, respectively; P<0.01), a higher proportion of urban women would report DV to law enforcement authorities (27.2% versus 2.9%, respectively; P<0.01).
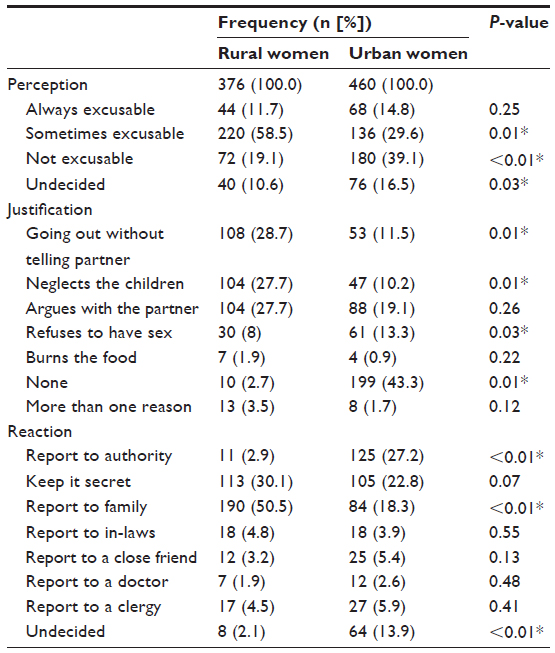 | Table 4 Comparison of the perception of domestic violence between rural and urban women |
Discussion
Prevalence of domestic violence
This study showed high prevalence rates of DV in both the rural and urban communities studied. These high prevalence rates are similar to the findings of a community-based study in Ibadan, Nigeria, but higher than the findings of hospital-based studies in Enugu and Abuja, Nigeria.15,17,18 The prevalence rates of DV in the 12 months preceding this study were also higher than in the findings for a rural community in the state of Anambra in Nigeria and in an urban community in Ibadan.11,17 The high prevalence rates of DV against women that are found among both rural and urban families in this study suggest that a high occurrence of DV against women has festered despite all of the media campaigns against it in Nigeria.
This study showed that significantly more rural Christian women experienced violence during the period of study than did urban Christian women. This study also showed that compared to urban women, significantly more rural women experienced more than one type of DV. These findings are in agreement with previous reports that suggested that women who were less educated and less likely to be employed were more likely to experience DV.4,11
The prevalence of physical violence among rural women in this study was much higher than the rates in the report from Anambra and in the 2008 Nigerian Demographic and Health Survey.20,26 In comparison, physical violence was reported significantly more often by rural women than by their urban counterparts. Physical beating of the women accounted for the most frequent form of physical violence in both communities. This finding agrees with the one in a previous report from Rwanda.27 However, there was no statistically significant difference in the rates of the beating of the respondents between the two communities. Beating the respondents was followed by slapping the victims, and this contrasts with the findings from previous reports from Enugu and Abakaliki in which slapping was the most common form of physical violence.13 The higher prevalence rates of physical violence found among rural women may be due to the cultural perception of the traditional Igbo society, which permits beating as a way to discipline erring members of the society. This perception is sustained by illiteracy and ignorance, both of which were more common among rural women in this study.
The prevalence rates of sexual violence reported in this study for both rural and urban communities were lower than those listed in previous reports from Abuja and South Africa.28,29 Although sexual violence was more common among rural women than among urban women, the difference between prevalence rates was not statistically significant. The lower prevalence rates of sexual violence among the women in both communities compared to the rates in the hospital-based studies may be due to concealment bias. It would be expected that women attending a religious event would be less likely to divulge information related to their sexual experiences than those attending hospitals.
Types of domestic violence
In this study, psychological violence was the most common type of DV in both rural and urban communities. This finding is similar to the findings of hospital-based studies in Enugu, Abakaliki, Anambra, Abuja, and Benin.12,13,17,18,20–22 Overall, psychological violence was slightly more common among rural woman than among urban women, but the difference was not statistically significant. The most common form of psychological violence was shouting at the victim, and this finding agrees with the previous findings in Enugu, Abakaliki, and Anambra.12,17,20 Shouting at the victim was reported significantly more often by rural than urban women. In contrast, not eating food prepared by the victim and not coming home to the victim were significantly more common among urban women than among rural women.
Perception of domestic violence
A high proportion of respondents felt that DV could be justified, and this would be unexpected in Christian families. More rural women than urban women were likely to excuse DV. This could be due to the fact that urban women were more likely to be educated and economically empowered than their rural counterparts. This justification rate of DV among the rural respondents was higher than the rate in the report from previous work among rural Nigerian women.30 However, the justification rate of DV among urban women in this study was similar to rates found in previous studies in Enugu and Abakaliki.13
Rural and urban women differed significantly in the reasons for justifying DV. Significantly more rural than urban women justified DV against women who went out without telling their partners, neglected their children, or did both. In contrast, significantly more urban than rural respondents justified DV against women who refused to have sex with their partners.
Compared to rural women, more urban women reported DV to authorities such as law enforcement agents, they sued the culprits in court, or they did both. This could be because the urban women were more educated, were more empowered economically, and understood their fundamental human rights better than their rural counterparts.
Strengths and limitations of the study
The major strength of this study includes its community-based nature, which enhances the external validity of the findings. The weaknesses include the use of women attending a religious event which, for both communities, allowed only women who had strong religious inclinations to be selected and which, in both cases, may render the results unrepresentative of the entire community. In addition, the use of women of reproductive age excludes women above 50 years, despite the possibility that women older than 50 years also experienced DV. Recall bias could also be a limitation of the study. The exclusion of focus group discussions meant that the details of the perception of DV could not be explored.
Conclusion
We conclude that the burden of DV among this sample of women was high and that rural women experienced higher levels of DV when compared to urban women. The high levels of DV in the Christian communities suggest that cultural factors could supersede Christian ethics in influencing DV against women in Nigeria. Given that the rural women in this study were less educated and less likely to be employed than the urban women, this finding of higher levels of DV among rural women supports the view that better education and the economic empowerment of women may help to curtail DV in our society.
Acknowledgments
The authors acknowledge the cooperation of the Christian Women’s Associations of the Okpanku Community and the Ogui Nike Community, both of which gave permission for the survey to be conducted.
Disclosure
The authors report no conflicts of interest in this work.
References
Little KJ. Screening for domestic violence. Identifying, assisting, and empowering adult victims of abuse. Postgrad Med. 2000;108(2):135–141; quiz 11. | |
Worku A, Addisie M. Sexual violence among female high school students in Debark, north west Ethiopia. East Afr Med J. 2002;79(2):96–99. | |
Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R. World Report on Violence and Health. Geneva, Switzerland: World Health Organization; 2002. | |
Fisher M, Yassour-Borochowitz D, Neter E. Domestic abuse in pregnancy: results from a phone survey in northern Israel. Isr Med Assoc J. 2003;5(1):35–39. | |
Ending violence against women. Population Reports (Series L). 1999;11:1–43. | |
Coker AL, Richter DL. Violence against women in Sierra Leone: frequency and correlates of intimate partner violence and forced sexual intercourse. Afr J Reprod Health. 1998;2(1):61–72. | |
Saror F. Spouse abuse: a study in Samaru, Zaria, Kaduna State, Nigeria. In: 10th Anniversary Women in Nigeria Conference. Breaking the Silence: Women against Violence. Kano, Nigeria: El-rafiu Prints and Company; 1993:70–84. | |
Sarkar NN. The impact of intimate partner violence on women’s reproductive health and pregnancy outcome. J Obstet Gynaecol. 2008;28(3):266–271. | |
Bacchus L, Bewley S, Gillian M. Domestic violence and pregnancy. Obstet Gynecol. 2001;3:56–59. | |
Achor J, Ibekwe P. Challenges of recognition of the psychiatric aspects of intimate partner violence. Ann Med Health Sci Res. 2012;2(1):78–86. | |
Deveci SE, Acik Y, Gulbayrak C, Tokdemir M, Ayar A. Prevalence of domestic violence during pregnancy in a Turkish community. Southeast Asian J Trop Med Public Health. 2007;38(4):754–760. | |
Ezegwui HU, Ikeme AC, Onwasigwe CN. Domestic violence against pregnant Nigerian women. Trop J Obstet Gynaecol. 2003;20(2):116–118. | |
Obi SN, Ozumba BC. Factors associated with domestic violence in south-east Nigeria. J Obstet Gynaecol. 2007;27(1):75–78. | |
Owoaje ET, Olaolorun FM. Intimate partner violence among women in a migrant community in southwest Nigeria. Int Q Community Health Educ. 2005–2006;25(4):337–349. | |
Schenker JG. FIGO committee for the study of ethical aspects of human reproduction. Violence against women. International Federation of Gynecology and Obstetrics. Ginekol Pol. 1996;67(11):583–584. | |
Federal Ministry of Health. National Reproductive Health Policy and Strategy to Achieve Quality Reproductive and Sexual Health for All Nigerians. Abuja, Nigeria: Federal Ministry of Health; 2001. Available from: http://www.youth-policy.com/Policies/Nigeria%20National%20Reproductive%20Health%20Policy%20and%20Strategy.pdf. Accessed June 15, 2014. | |
Odimegwu CO, Okemgbo CN. Women against women; women’s perception of girl-child status in Abakaliki area of Nigeria. Inter J Soc Policy Stud. 2001;4(2):73–84. | |
Okemgbo CN, Omideyi AK, Odimegwu CO. Prevalence, patterns and correlates of domestic violence in selected Igbo communities of Imo State, Nigeria. Afr J Reprod Health. 2002;6(2):101–114. | |
Odujinrin O. Wife battering in Nigeria. Int J Gynaecol Obstet. 1993; 41(2):159–164. | |
Ilika AL, Okonkwo PI, Adogu P. Intimate partner violence among women of childbearing age in a primary health care centre in Nigeria. Afr J Reprod Health. 2002;6(3):53–58. | |
Olagbuji B, Ezeanochie M, Ande A, Ekaete E. Trends and determinants of pregnancy-related domestic violence in a referral center in southern Nigeria. Int J Gynaecol Obstet. 2010;108(2):101–103. | |
Ebeigbe PN, Igberase GO. Screening for intimate partner physical violence against women in outpatient clinics of a Nigerian tertiary hospital. Niger Med J. 2008;49(1):1–4. | |
Williams L. Nigeria: The Bradt Travel Guide. 2nd ed. Chalfont, UK: Bradt Travel Guides; 2008. | |
National Population Commission of Nigeria. 2006 Population and Housing Census. | |
García-Moreno C, Jansen HAFM, Ellsberg M, Watts C, Heise L. WHO Multi-country Study on Women’s Health and Domestic Violence against Women. Geneva, Switzerland: World Health Organization; 2005. Available from: http://www.who.int/gender/violence/who_multicountry_study/Annex3-Annex4.pdf?ua=1. Accessed January 5, 2014. | |
National Population Commission (NPC) and ICF Macro. Nigeria: 2008 Demographic and Health Survey Key Findings. Calverton, MD: NPC and ICF Macro; 2009. Available from: http://dhsprogram.com/pubs/pdf/SR173/SR173.pdf. Accessed June 15, 2014. | |
Ntaganira J, Muula AS, Masaisa F, Dusabeyezu F, Siziya S, Rudatsikira E. Intimate partner violence among pregnant women in Rwanda. BMC Womens Health. 2008;8:17. | |
Modiba LM, Baliki O, Mmalasa R, Reineke P, Nsiki C. Pilot survey of domestic abuse amongst pregnant women attending an antenatal clinic in a public hospital in Gauteng Province in South Africa. Midwifery. 2011;27(6):872–879. | |
Efetie ER, Salami HA. Domestic violence on pregnant women in Abuja, Nigeria. J Obstet Gynaecol. 2007;27(4):379–382. | |
Antai DE, Antai JB. Attitudes of women toward intimate partner violence: a study of rural women in Nigeria. Rural Remote Health. 2008;8(3):996. |
Supplementary materials
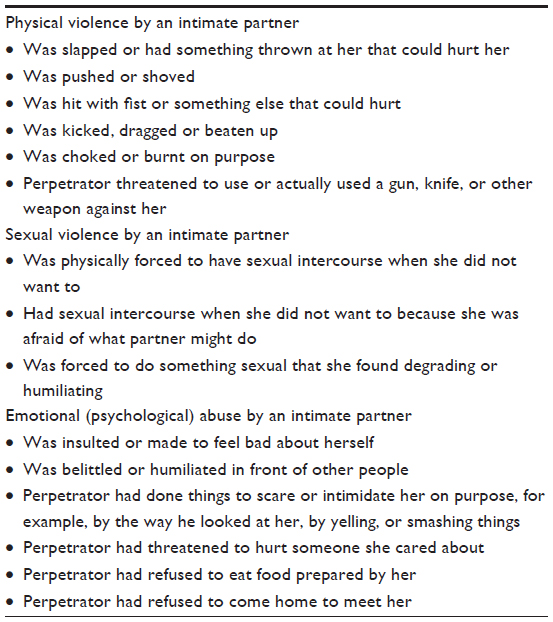 | Table S1 Operational definitions of violence used in this study based on the World Health Organization’s Multi-country Study on Women’s Health and Domestic Violence against Women |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.