")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Comparative efficacy of alemtuzumab and established treatment in the management of multiple sclerosis
Received 9 February 2015
Accepted for publication 8 April 2015
Published 18 May 2015 Volume 2015:11 Pages 1221—1229
DOI https://doi.org/10.2147/NDT.S60518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Rachel Babij, Jai S Perumal
Department of Neurology, Weill Cornell Medical College, New York, NY, USA
Abstract: Alemtuzumab is the newest disease-modifying therapy approved for the treatment of relapsing multiple sclerosis. Alemtuzumab is an anti-CD52 targeted antibody that causes lysis of T and B lymphocytes, monocytes, natural killer cells, macrophages, and dendritic cells. Following its administration, a prolonged T-cell lymphopenia results with emergence of a reconstituted immune system that differs in its composition from that pretreatment. In clinical trials, alemtuzumab has shown impressive efficacy with regard to clinical and radiological outcomes in relapsing multiple sclerosis, along with sustained long-term beneficial effects, and it is attractive for its once-yearly administration. Despite this, the occurrence of serious secondary autoimmune disorders, infections, and a potential risk of malignancy necessitates a careful evaluation of risks versus benefits for an individual patient prior to its use. The requirement of patient commitment to the intense mandatory monitoring program is also a factor to be considered when incorporating alemtuzumab into the treatment regimen.
Keywords: alemtuzumab, multiple sclerosis, comparative efficacy
Introduction
Multiple sclerosis (MS) is an autoimmune disorder characterized by inflammation, demyelination, and neurodegeneration.1,2 The first disease-modifying therapy for MS was approved in 1993, and there have since been nine other treatments approved in the USA and Europe, including, most recently, the approval of alemtuzumab by the US Food and Drug Administration (FDA) in November 2014.3–5
Traditionally, first-line agents for the treatment of MS have included interferon b (intramuscular 1a, subcutaneous 1a, and subcutaneous 1b) and glatiramer acetate. Natalizumab and fingolimod have generally been used when patients fail one or more of the above agents; however, with growing experience of their use, albeit less commonly, they are being used as the first agent in patients with highly active disease at onset as well.6 Although the injectable therapies have well established long-term safety data, the inconvenience of injections, the side effects associated with their use, and adherence to the treatment regimen continue to be detriments to their use.4 If increasing experience with the three approved oral medications (fingolimod, teriflunomide, and dimethyl fumarate) establishes their sustained clinical efficacy and long-term safety profiles, their use as first-line agents would be expected to expand in the coming years. The use of alemtuzumab at present will likely be reserved for patients with highly active disease who fail other agents.
Importantly, all medications are approved for the treatment of relapsing MS. Clinical trials have demonstrated efficacy in the relapsing forms of MS, but unfortunately have not shown therapeutic benefit in progressive forms of the disease.7,8 Results of therapeutic trials in primary progressive MS have been disappointing.9,10 With regard to secondary progressive MS, optimal treatment of the relapsing phase early in the disease seems to have the greatest impact in determining the course of the secondary progressive phase rather than escalating therapy in the secondary progressive stage.
There is increasing interest in the concept of a “therapeutic window of opportunity in MS”. Accumulating evidence points to the benefits of early treatment and the presence of a window of opportunity in which to treat patients in order to have a meaningful impact on long-term disability.4,9,10 Disability in the relapsing phase of the disease seems to depend predominantly on focal central nervous system inflammation, while permanent disability in the progressive phase depends on neurodegeneration rather than on ongoing inflammation, and the most important factor determining the rate of progression seems to be the time taken to reach onset of the progressive stage.1 Experience from prior trials and clinical practice, including an early trial with alemtuzumab, demonstrated that even if effective suppression of inflammation is achieved in the progressive phase, this does not necessarily translate to halting or slowing disease progression.11 Thus, the opportunity to treat patients may come early in the disease before the second degenerative phase is reached.10,12,13
The importance of early optimal treatment as discussed in the preceding paragraph necessitates utilization of early prognostic indicators in deciding the best treatment for an individual patient. Although no specific biomarker that might accurately predict long-term outcome has been identified, several studies have looked at early clinical and magnetic resonance imaging (MRI) features that might indicate the subsequent disease course. Among early clinical features that help make an early determination are: frequency of relapses within the first 2–5 years, incomplete recovery from the first attack, and involvement of the motor and brainstem as possible features of patients deserving aggressive treatment.11,14–16 MRI features that might help include the baseline T2 lesion volume, early brain atrophy, number of gadolinium-enhancing lesions, and particularly the change in T2 lesion volume early in the disease course despite being on disease-modifying therapy.15,17
Given this scenario of expanding treatment choices, a better understanding of disease mechanisms in MS, and greater need for early initiation of appropriate and optimal treatment, we aim to review the newest drug, alemtuzumab, try to decipher the role that it can play in the current treatment algorithm, and provide patient-focused perspectives on its use.
Mechanism of action of alemtuzumab and other agents approved for MS
Increasing knowledge and better elucidation of the pathological inflammatory processes that occurs in MS has led to the development of many immunomodulatory therapies in recent years. Table 1 lists the agents currently approved by the FDA and their postulated mechanisms of action. Current therapies target immune cell survival, proliferation or behavior in the periphery, as well as transmigration of the cells across the blood–brain barrier.18 The newest member of the repertoire is alemtuzumab.19 Alemtuzumab is a humanized monoclonal antibody targeting the CD52 molecule, a glycoprotein present in high quantities in the membrane rafts of B-cells and T-cells, as well as other cells of the adaptive immune system. The role of the CD52 molecule is not known, but it may play a role in cell–cell interactions or T-cell migration and costimulation. Alemtuzumab mediates death of immune cells through cellular and complement-mediated induction of apoptosis, and the subsequent reconstitution of the immune system is characterized by changes in the number, proportions, and properties of the lymphocyte subsets. Namely, there is an increase in regulatory T-cells. T-regulatory cells mediate anergy and lessen T-cell responses; this response to alemtuzumab has been demonstrated both in patients and in in vitro studies. Additionally, there is a change in the cytokine environment, a decrease in proinflammatory interferon-gamma and interleukin (IL)-17, and an increase in anti-inflammatory IL-4, IL-10, and transforming growth factor-b. It is thought that this rebalancing of the immune system contributes to the therapeutic benefits, and results in persistent benefits long after clearance of the antibody.20–23
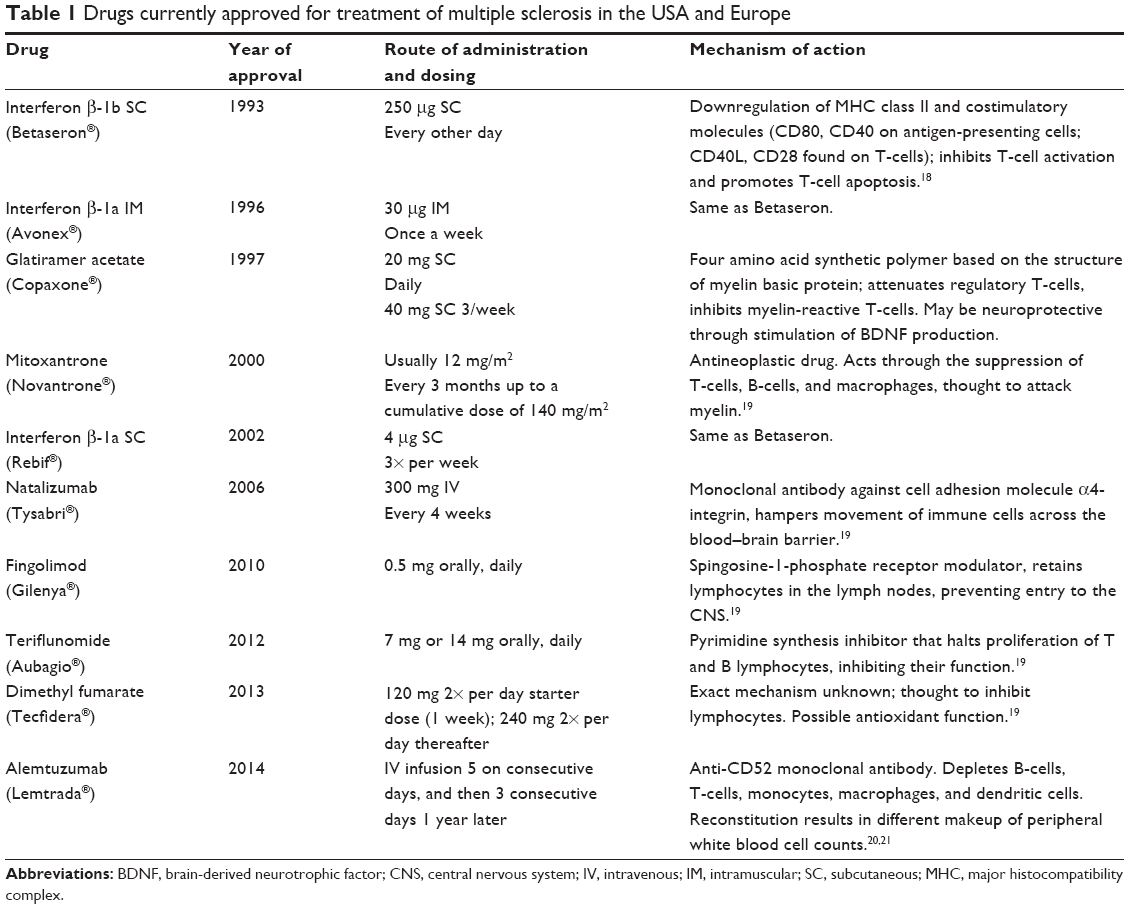 | Table 1 Drugs currently approved for treatment of multiple sclerosis in the USA and Europe |
The decrease in the level of circulating T and B lymphocytes occurs very rapidly, with the lowest values observed within days post-treatment. Lymphocytes repopulate over time, with B-cells returning first, usually with complete recovery within the year, and T-cell populations taking much longer.24
The efficacy of alemtuzumab in MS is likely the result of multiple mechanisms of action. Administration of alemtuzumab results in depletion of circulating T and B lymphocytes within days. The sustained improvement in disability and brain atrophy, even in patients without clinically active disease, would suggest that the benefits seen with alemtuzumab are not entirely anti-inflammatory, but also due to brain repair and neuroprotection promoted by an altered lymphocyte milieu.25,26 This includes the effects of an altered lymphocyte repertoire with a greater proportion of regulatory T-cells and secretion of neurotrophic factors. Studies have shown that when the reconstituted lymphocytes are stimulated with myelin basic protein, they secrete neurotrophins, including brain-derived neurotrophic growth factor, platelet-derived growth factor, and ciliary neurotrophic factor, which enhance neuronal repair, oligodendrocyte survival, and maturation and myelination.27
Another possible mechanism of action of alemtuzumab could come from its effect on the B-cell lymphocyte pool. Although initially postulated to be a T-cell-mediated autoimmune disease, increasing evidence points to involvement of B-cells as well.28 This evidence includes the presence of specific oligoclonal banding patterns in the cerebrospinal fluid of MS patients, demyelination in vitro with antibodies from MS patients,29 reported effectiveness of intravenous immunoglobulin therapy for treating a subset of MS patients,30–33 and the demonstrated efficacy of rituximab and ocrelizumab, which are anti-CD20, B-cell-depleting therapies in MS.29–34 Alemtuzumab produces profound and prolonged alteration in the reconstituted B-cell lymphocyte pool.35
Comparative efficacy, safety, and tolerability with respect to established treatments
There are currently ten treatments approved by the FDA for relapsing MS. The Phase III clinical trial data for newer agents including the oral medications and natalizumab and alemtuzumab are shown in Table 2.36–43
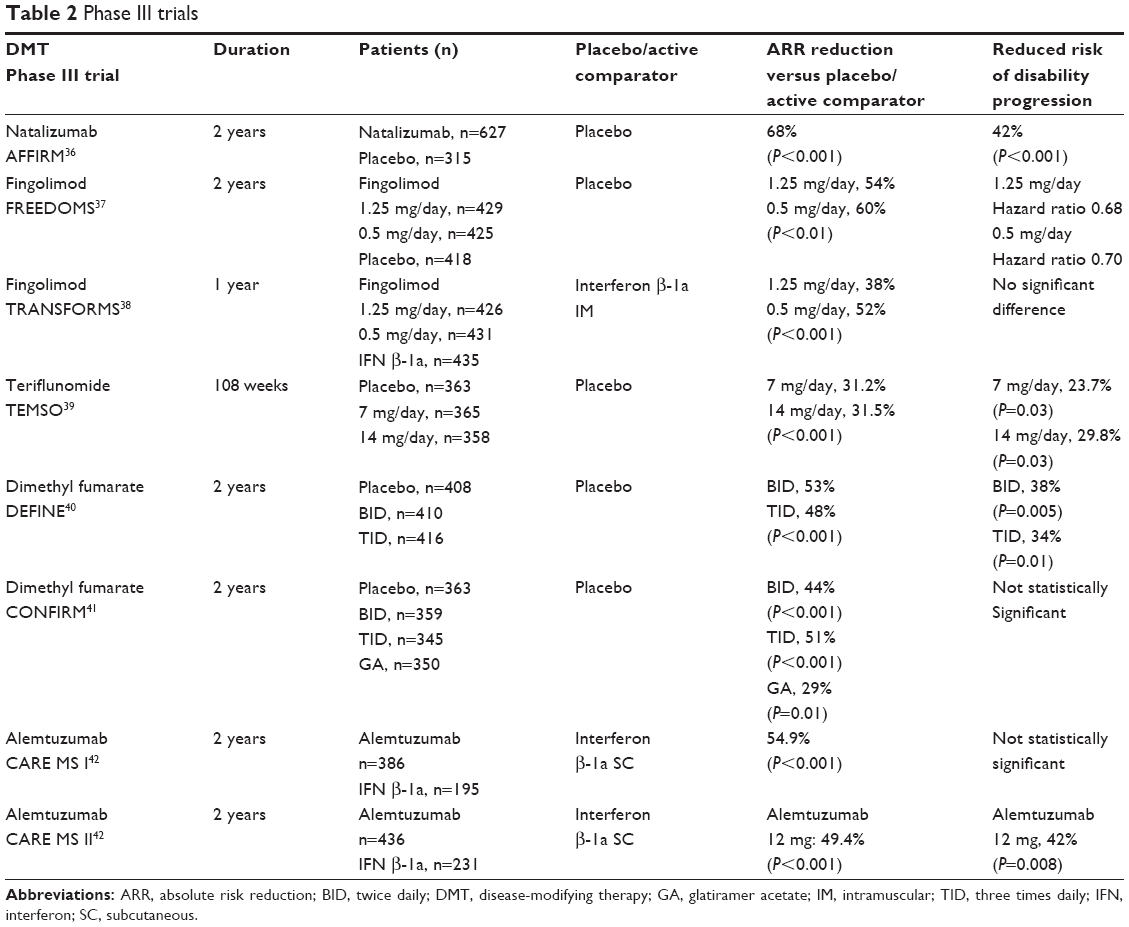 | Table 2 Phase III trials |
Alemtuzumab was initially tested in small open-label studies of MS patients in Cambridge, UK, beginning with 58 patients who had secondary progressive MS, followed by 22 patients who had failed other treatments.44 Results from these trials pointed to greater benefits in treating the early relapsing-remitting phase of the disease.12 After promising results from these early studies, alemtuzumab was tested in a Phase II study (CAMMS223) followed by two Phase III studies (CARE-MSI and CARE-MSII). In all three trials, alemtuzumab was compared with interferon b-1a subcutaneously (Table 3). In the Phase II CAMMS223 trial, 334 patients were randomized to receive subcutaneous interferon b-1a (44 μg three times per week) or annual infusions of alemtuzumab at two doses (12 mg or 24 mg per day). Inclusion criteria for this trial were previously untreated patients with disease duration of less than 3 years, an Expanded Disability Status Scale score of ≤3, a two or more clinical relapses in the preceding 2 years, and at least one gadolinium-enhancing lesion on monthly MRI scans obtained up to 4 months prior. Alemtuzumab treatment was suspended because three patients developed immune thrombocytopenic purpura, one of whom died; however, all but nine patients had received more than one infusion cycle (161 patients received two cycles; 45 patients received three). Treatment continued in the subcutaneous interferon b-1a arm. Alemtuzumab significantly reduced the rate of sustained accumulation of disability (9% versus 26.2%) and the annualized relapse rate (0.1 versus 0.36). The mean disability score improved by 0.39 in the alemtuzumab group and worsened in the interferon b-1a group. On MRI analysis, the lesion burden was reduced, and brain volume was increased from baseline in the alemtuzumab group and reduced in the interferon b-1a group.45
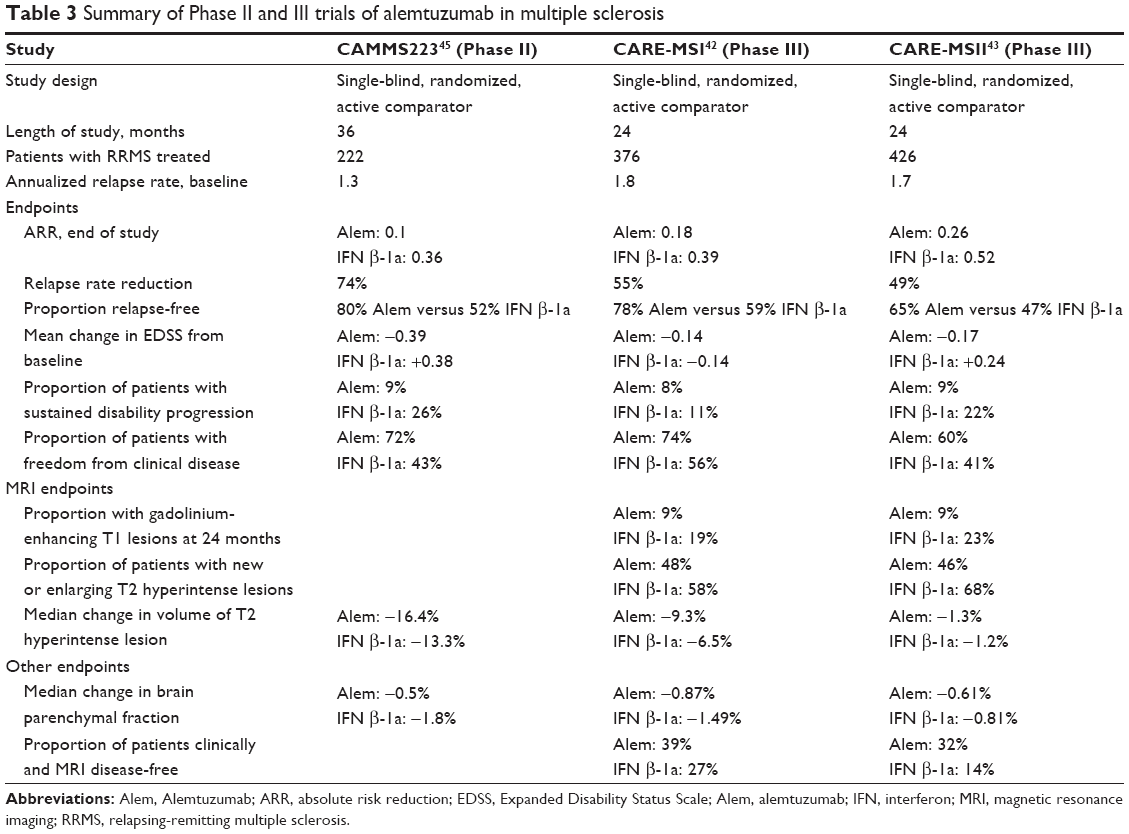 | Table 3 Summary of Phase II and III trials of alemtuzumab in multiple sclerosis |
A 5-year extension study of participants in the Phase II trial of alemtuzumab continued to demonstrate long-term sustained benefits when compared with the interferon group. Over 5 years, alemtuzumab decreased the risk of sustained accumulation of disability by 72% and the relapse rate by 69% compared with interferon b-1a (P<0.0001). The annualized relapse rate from baseline to month 60 was 0.11 for alemtuzumab and 0.35 for interferon b-1a. No new adverse safety events were noted during follow-up.46 The most recent long-term follow-up data published on alemtuzumab-treated patients in its clinical trials assesses efficacy and safety after a median of 7 years. A total of 87 patients participated in this observational study, including patients from CAMM223 and also those from the SM3 trial, where in addition to alemtuzumab, patients were also infused with an inert variant aimed to prevent the development of antibodies to alemtuzumab.47 Fifty-two percent of patients in the 7-year follow-up required just two cycles of alemtuzumab. In the remaining patients, relapses resulted in three (36%), four (8%), or five (1%) cycles. The mean annualized relapse rate after alemtuzumab was 0.16 compared with 1.78 in the 2 years prior to treatment. A greater proportion of patients had a 6-month sustained reduction in disability than a sustained accumulation (43.5% versus 32.2%), and a similar trend was seen when the time period was increased to 12 months (37.7% versus 21.8%). Among the 87 patients, median disability improved following alemtuzumab, with 43 patients having “net improved” disability, 35 having “net worse”, and nine having “net unchanged”. A decrement in positive disability outcome was associated with older age and, to a lesser extent, longer disease duration at the time of treatment.48
Phase III studies compared alemtuzumab with interferon b-1a in treatment-naïve patients (CARE-MSI42) as well as in patients who had failed previous treatment (CARE-MSII43). In CARE-MS I, 581 patients were randomized in a 2:1 manner to receive alemtuzumab or interferon b-1a subcutaneously. Primary endpoints for this study were relapse rate and time to sustained accumulation of disability. Forty percent of interferon-treated patients and 22% of alemtuzumab-treated patients experienced a relapse, which corresponded to a 54.9% risk reduction (P<0.0001) in the alemtuzumab group. Eleven percent of interferon-treated patients and 8% of alemtuzumab-treated patients had disability progression; however, the difference between the groups did not reach statistical significance. On MRI parameters, including proportions of patients with gadolinium-enhancing lesions, new or enlarging T2 lesions, and brain volume loss, alemtuzumab was superior to subcutaneous interferon b-1a. More patients in the alemtuzumab arm remained free from clinical disease activity and combined clinical and radiological disease. The CARE-MS II trial examined 667 patients with at least one relapse on interferon b or glatiramer, who were then randomized to alemtuzumab or subcutaneous interferon b-1a. The primary endpoints were relapse rate and time to sustained accumulation of disability. Fifty percent of the interferon group and 35% of the alemtuzumab group experienced a relapse, which corresponded to a 49.9% risk reduction in the alemtuzumab group and 20% in interferon-treated patients, and 13% of alemtuzumab-treated patients had disability progression, which corresponded to a 42% risk reduction; both of these differences were statistically significant. Alemtuzumab was superior to interferon for MRI parameters, including the proportion of patients with gadolinium-enhancing lesions, new or enlarging T2 lesions, and reduction in brain volume loss.
Safety and tolerability
The most common adverse events were infusion-associated reactions, which were seen in more than 90% of patients who received alemtuzumab. Most of these reactions were characterized by symptoms including fever, chills, myalgia, and rash, which are ameliorated largely by prior administration of antipyretics, antihistamines, and steroids. Serious infusion reactions occurred in 3%, including anaphylaxis in two patients.
Mild to moderate infections were seen more frequently in the alemtuzumab-treated group than in the interferon-treated group. There were more instances of herpes infections in the alemtuzumab group (16% versus 3% in the interferon group). These were predominantly oral infections and herpes zoster. Due to a high incidence of herpes infection in the days following infusion of alemtuzumab, the Phase III CARE MS II trial underwent a protocol amendment with addition of acyclovir prophylaxis during and in the early months following alemtuzumab infusion, with reduction in infection rate during this period. The rate of herpes infections decreased from 2.8% to 0.5% for the first course and from 2.1% to 0.4% for the second course of alemtuzumab. There were no deaths reported as a result of serious or opportunistic infections.
Secondary autoimmune disorders are a significant risk associated with use of alemtuzumab. Based on incidence in the clinical trials, the most common is thyroid disorder, including hyperthyroidism, hypothyroidism, and Graves’ disease, which occurred in 34% of patients.49 Immune thrombocytopenia was seen in 2% of patients treated with alemtuzumab in CAMMS223; the index patient who developed this condition in the clinical trial died from lack of recognition and failure to seek medical attention, ultimately succumbing to intracerebral hemorrhage.45 The subsequent cases were recognized early and appropriate intervention was taken, with favorable outcomes. Additionally, two patients developed anti-glomerular basement membrane disease (Goodpasture’s syndrome) and one patient developed membranous glomerulonephritis following treatment.50 There were rare (<0.2%) instances of neutropenia, hemolytic anemia, and pancytopenia. Forty-eight percent of patients in the 7-year follow-up analysis developed secondary autoimmunity, most of which had been reported in previous studies.48
In the clinical studies, 0.3% of alemtuzumab-treated patients developed thyroid cancer, compared with none in the interferon b-1a-treated group. In addition, two further cases of thyroid cancer were diagnosed in alemtuzumab-treated patients during observational studies. Melanoma was seen in 0.3% of patients treated with alemtuzumab. Rare cases of lymphoproliferative disorders and lymphoma, including mucosa-associated lymphoid tissue lymphoma, Castleman’s disease, and a case of non-Epstein-Barr virus-associated Burkitt’s lymphoma which was fatal following treatment have been reported in MS patients treated with alemtuzumab (http://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM425409.pdf).
Patient-focused perspectives and profiles appropriate for alemtuzumab
There are one of two approaches one could adopt in treating MS, ie, induction versus escalation therapy. Induction or escalation of treatment could be achieved by using one highly efficacious agent or a simultaneous combination of therapies. Combination therapy has not been utilized to any significant extent in MS, likely because of the difficulties associated with administration of multiple injectables at the same time (as all the medications initially approved for MS were parenteral until the advent of fingolimod in 2010) and lack of data supporting increased efficacy from the combination of intramuscular interferon b-1a and glatiramer acetate in a large clinical trial.51
There is increasing knowledge that early optimal intervention provides the best opportunity to favorably influence the long-term outcome of MS. Suboptimal control of the disease early in its course might bring into play a cascade of irreversible events that are not amenable to later treatment and would result in permanent disability. Given the importance of early effective treatment, one could use data from several studies that outline potential early prognostic indicators that might give us insight into an individual patient’s disease course when making appropriate treatment choices. For a patient who has unfavorable prognostic indicators, ie, multiple early relapses, severe relapses with residual deficits, significant brainstem/spinal cord involvement, or a large lesion burden on MRI, it might be prudent to use one of the more aggressive treatments as the patient’s first disease-modifying therapy or have a low threshold to switch to a more aggressive therapy at the earliest indication of a suboptimal response.
Generally, natalizumab appears to be more effective than the injectable treatments. Fingolimod was compared with intramuscular interferon b-1a in one of its Phase III trials and demonstrated greater efficacy. Dimethyl fumarate has not been compared in head-to-head trials with another agent, although one of its clinical trials included a glatiramer acetate arm. Alemtuzumab has demonstrated impressive efficacy when compared with subcutaneous interferon b-1a in three clinical trials. Based on the data we currently have, given its efficacy, it will be used for patients with highly active disease. As to its order of use in the treatment sequence, while in Europe the European Medicines Agency states that “Lemtrada is indicated for adult patients with relapsing remitting multiple sclerosis (RRMS) with active disease defined by clinical or imaging features” (http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003718/WC500150521.pdf), and hence it could be potentially used as first-line therapy, the FDA in its approval states that “Because of its safety profile, the use of Lemtrada should generally be reserved for patients who have had an inadequate response to two or more drugs indicated for the treatment of MS.” Hence, in the USA, alemtuzumab will be used mainly as an escalation therapy rather than as an initial induction agent.
Despite its remarkable efficacy, because of the significant risk of secondary autoimmune disorders, prolonged immune suppression, potential risk of infections, and potential increased risk of certain malignancies, treatment with alemtuzumab should be undertaken only after a thorough risk versus benefit evaluation. The Risk Evaluation and Mitigation Strategy program mandated with use of alemtuzumab will serve to provide close vigilance for emergence of any adverse event and allow immediate remediation measures to lower the likelihood of a poor outcome. Patient adherence to this protocol has to be strictly enforced, and patient commitment to it ensured prior to initiation of treatment, and this will play an important role in patient selection.
Conclusion
Alemtuzumab is the newest medication in the armamentarium to treat MS. It has shown impressive long-term efficacy, and being administered as an infusion cycle once a year would pose no issues with treatment adherence. However, its use is associated with potentially serious adverse events, and the risks versus benefits would need to be carefully weighed for each patient before initiation of treatment. It is vital for patients to adhere to the long-term Risk Evaluation and Mitigation Strategy program and be closely monitored for any adverse event. Ultimately, its growth and expanding use in MS would depend on accumulation of positive patient and physician experience and with continued demonstration of sustained high efficacy over long-term safety concerns.
Acknowledgment
RB is supported by a medical scientist training program grant from the National Institute of General Medical Sciences of the National Institute of Health under award number T32GM007739 to the Weill Cornell/Rockefeller/Sloan-Kettering Tri-Institutional MD-PhD Program.
Disclosure
JSP is a speaker bureau member for Biogen Idec, Teva Pharmaceuticals, Accorda Pharmaceuticals, and Genzyme Corporation. The authors report no other conflict of interest in this work.
References
Vukusic S, Confavreaux C. Natural history of multiple sclerosis: risk factors and prognostic indicators. Curr Opin Neurol. 2007;20(3): 369–374. | ||
Weinshenker BG, Rice GP, Noseworthy JH, Carriere W, Baskerville J, Ebers GC. The natural history of multiple sclerosis: a geographically based study. I. Clinical course and disability. Brain. 1989;112: 133–146. | ||
Jeffrey S. FDA approval for alemtuzumab (Lemtrada) in MS. Medscape Medical News, 2014. Available from: http://www.medscape.com/viewarticle/834994. Accessed April 9, 2015. | ||
Sorensen P. New management algorithms in multiple sclerosis. Curr Opin Neurol. 2014;27(3):246–259. | ||
Weinstock-Guttman B. An update on new and emerging therapies for relapsing-remitting multiple sclerosis. Am J Manag Care. 2013; 19(17 Suppl):343–354. | ||
Perumal J, Khan O. Emerging disease-modifying therapies in multiple sclerosis. Curr Treat Options Neurol. 2012;14(3):256–263. | ||
Cree BA. 2014 Multiple sclerosis therapeutic update. Neurohospitalist. 2014;4(2):63–65. | ||
Noyes K, Weinstock-Guttman B. Impact of diagnosis and early treatment on the course of multiple sclerosis. Am J Manag Care. 2013; 19(17 Suppl):321–333. | ||
Wolinsky JS, Narayana PA, O’Connor P, et al. Glatiramer acetate in primary progressive multiple sclerosis: results of a multinational, multicenter, double-blind, placebo-controlled trial. Ann Neurol. 2007;61(1): 14–24. | ||
Hawker K, O’Connor P, Freedman MS, et al. Rituximab in patients with primary progressive multiple sclerosis: results of a randomized double-blind placebo-controlled multicenter trial. Ann Neurol. 2009; 66(4):460–471. | ||
Freedman MS. Treatment options for patients with multiple sclerosis who have a suboptimal response to interferon beta therapy. Eur J Neurol. 2013;21(3):377–387. | ||
Coles AJ, Cox A, Le Page E, et al. The window of therapeutic opportunity in multiple sclerosis: evidence from monoclonal antibody therapy. J Neurol. 2006;253(1):98–108. | ||
Confavreaux C, Vukusic S. The clinical course of multiple sclerosis. Handb Clin Neurol. 2014;122:343–369. | ||
Wingerchuk D, Carter J. Multiple sclerosis: current and emerging disease-modifying therapies and treatment strategies. Mayo Clin Proc. 2014;89(2):225–240. | ||
Fisniku LK, Brex PA, Altmann DR, et al. Disability and T2 MRI lesions: a 20-year follow-up of patients with relapse onset of multiple sclerosis. Brain. 2008;131 Pt 3:808–817. | ||
Fisher E, Rudick RA, Simon JH, et al. Eight-year follow-up study of brain atrophy in patients with MS. Neurology. 2002;59(9):1412–1420. | ||
Morgen K, Jeffries NO, Stone R, et al. Ring-enhancement in multiple sclerosis: marker of disease severity. Mult Scler. 2001;7(3):167–171. | ||
Ali R, Nicholas RS, Muraro PA. Drugs in development for relapsing multiple sclerosis. Drugs. 2013;73(7):625–650. | ||
National Multiple Sclerosis Society. Medications approved for the treatment of multiple sclerosis. Available from: http://www.nationalmssociety.org/Treating-MS/Medications. Accessed April 9, 2015. | ||
Havari E, Turner MJ, Campos-Rivera J, et al. Impact of alemtuzumab treatment on the survival and function of human regulatory T cells in vitro. Immunology. 2014;141(1):123–131. | ||
Coles A. Alemtuzumab treatment of multiple sclerosis. Semin Neurol. 2013;33(1):66–73. | ||
Bar-Or A, Fawaz L, Fan B, et al. Abnormal B-cell cytokine responses a trigger of T-cell mediated disease in MS? Ann Neurol. 2010;67(4): 452–461. | ||
Lapalombella R, Andritsos L, Baiocchi RA, Lin TS, Byrd JC. Alemtuzumab (Campath-1H) in the treatment of chronic lymphocytic leukemia. Oncogene. 2007;26(25):3644–3653. | ||
Menge T, Stüve O, Kieseier BC, Hartung HP. Alemtuzumab: the advantages and challenges of a novel therapy in MS. Neurology. 2014;83(1): 87–97. | ||
Jones D, Goldman M. Alemtuzumab for the treatment of relapsing-remitting multiple sclerosis: a review of its clinical pharmacology, efficacy and safety. Expert Rev Clin Immunol. 2014;10(10):1281–1291. | ||
Hartung H, Aktas O, Boyko AN. Alemtuzumab: a new therapy for active relapsing-remitting multiple sclerosis. Mult Scler. 2015;21(1):22–34. | ||
Jones JL, Anderson JM, Phuah CL, et al. Improvement in disability after alemtuzumab treatment of multiple sclerosis is associated with neuroprotective autoimmunity. Brain. 2010;133 Pt 8:2232–2247. | ||
Krumbholz M, Derfuss T, Hohlfeld R, Meinl E. B cells and antibodies in multiple sclerosis pathogenesis and therapy. Nat Rev Neurol. 2012;8(11):613–623. | ||
Elliot C, Lindner M, Arthur A, et al. Functional identification of pathogenic autoantibody responses in patients with multiple sclerosis. Brain. 2012;135(6):1819–1833. | ||
Keegan M, König F, McClelland R, et al. Relation between humoral pathological changes in multiple sclerosis and response to therapeutic plasma exchange. Lancet. 2005;366(9485):579–582. | ||
Heigl F, Hettich R, Arendt R, Durner J, Koehler J, Mauch E. Immunoadsorption in steroid-refractory multiple sclerosis: clincial experience in 60 patients. Atheroscler Suppl. 2013;14(1):167–173. | ||
Leussink VI, Lehmann HC, Meyer zu Hörste G, Hartung HP, Stüve O, Kieseier BC. Rituximab induces clinical stabilization in a patient with fulminant multiple sclerosis not responding to natalizumab: evidence for disease heterogeneity. J Neurol. 2008;255(9):1436–1438. | ||
Stüve O, Cepok S, Elias B, et al. Clinical stabilization and effective B-lymphocyte depletion in the cerebrospinal fluid and peripheral blood of a patient with fulminant relapsing-remitting multiple sclerosis. Arch Neurol. 2005;62(10):1620–1623. | ||
Stüve O, Leussink VI, Fröhlich R, et al. Long-term B-lymphocyte depletion with rituximab in patients with relapsing-remitting multiple sclerosis. Arch Neurol. 2009;66(2):259–261. | ||
Thompson S, Jones JL, Cox AL, Compston DA, Coles AJ. B-cell reconstitution and BAFF after alemtuzumab (Campath-1H) treatment of multiple sclerosis. J Clin Immunol. 2010;30(1):99–105. | ||
Polman CH, O’Connor PW, Havrdova E, et al. A randomized placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. 2006;354(9):899–891. | ||
Kappos L, Radue EW, O’Connor P, et al. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med. 2010; 362(5):387–401. | ||
Cohen JA, Barkhof F, Comi G, et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med. 2010; 362(5): 402–415. | ||
O’Connor P, Wolinsky JS, Confavreux C, et al. Randomized trial of oral teriflunomide for relapsing multiple sclerosis. N Engl J Med. 2011; 365(14):1293–1303. | ||
Bar-Or A, Gold R, Kappos L, et al. Clinical efficacy of BG-12 (dimethyl fumarate) in patients with relapsing-remitting multiple sclerosis: subgroup analyses of the DEFINE study. J Neurol. 2013;260(9): 2297–2305. | ||
Fox RJ, Miller DH, Phillips JT, et al. Placebo-controlled Phase 3 study of oral BG-12 or glatiramer in multiple sclerosis. N Engl J Med. 2012;367(12):1087–1097. | ||
Cohen JA, Coles AJ, Arnold DL, et al. Alemtuzumab versus interferon beta-1a as a first-line treatment for patients with relapsing-remitting multiple sclerosis: a randomized controlled phase 3 trial. Lancet. 2012; 380(9856):1819–1828. | ||
Coles AJ, Twyman CL, Arnold DL, et al. Alemtuzumab for patients with relapsing multiple sclerosis after disease-modifying therapy: a randomised controlled phase 3 trial. Lancet. 2012;380(9856): 1829–1839. | ||
Brown JW, Coles AJ. Alemtuzumab: evidence for its potential in relapsing-remitting multiple sclerosis. Drug Des Devel Ther. 2013;7: 131–138. | ||
CAMMS223 Trial Investigators, Coles AJ, Compston DA, Selmaj KW, et al. Alemtuzumab vs interferon beta-1a in early multiple sclerosis: the CAMMS223 trial investigators. N Engl J Med. 2008; 359(17): 1786–1801. | ||
Coles A, Coles AJ, Fox E, Vladic A, et al. Alemtuzumab more effective than interferon b-1a at 5-year follow up of CAMMS223 trial. Neurology. 2012;78(14):1069–1078. | ||
Somerfield J, Hill-Cawthorne GA, Lin A, et al. A novel strategy to reduce the immunogenicity of biological therapies. J Immunol. 2010; 185(1):763–768. | ||
Tuohy O, Costelloe L, Hill-Cawthorne G, et al. Alemtuzumab treatment of multiple sclerosis: long-term safety and efficacy. J Neurol Neurosurg Psychiatry. 2015;86(2):208–215. | ||
Kousin-Ezewu O, Coles A. Alemtuzumab in multiple sclerosis: latest evidence and clinical prospects. Ther Adv Chronic Dis. 2013;4(3): 97–103. | ||
Clatworthy MR, Wallin EF, Jayne DR. Anti-glomerular basement membrane disease after alemtuzumab. N Engl J Med. 2008;359(7): 768–769. | ||
Lublin FD, Cofield SS, Cutter GR, et al. Randomized study combining interferon and glatiramer acetate in multiple sclerosis. Ann Neurol. 2013;73(3):327–340. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.