")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Clinical role of dual bronchodilation with an indacaterol–glycopyrronium combination in the management of COPD: its impact on patient-related outcomes and quality of life
Authors Rossi A, Zanardi E, Poletti V, Cazzola M
Received 24 September 2014
Accepted for publication 22 April 2015
Published 23 July 2015 Volume 2015:10(1) Pages 1383—1392
DOI https://doi.org/10.2147/COPD.S55488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Richard Russell
Andrea Rossi,1 Erika Zanardi,2 Venerino Poletti,3 Mario Cazzola4
1Pulmonary Unit, University of Verona, Verona, 2Department of Respiratory and General Rehabilitation, ULSS 20, Verona, 3Pulmonary Unit, GB Morgani Hospital, AUSL 20, Forli, 4Pulmonary Unit, University of Rome, Tor Vergata, Italy
Abstract: Chronic obstructive pulmonary disease (COPD) is the result of persistent and progressive pathologic abnormalities in the small airways, most often associated with alveolar loss. Smoking cessation is the most effective intervention to slow down the progression of COPD. Long-acting inhaled bronchodilators are prescribed for the symptomatic relief at any stage of disease severity. For patients whose COPD cannot be not sufficiently controlled with long-acting bronchodilator monotherapy, international guidelines suggest the possibility of associating a long-acting beta2 agonist (LABA) with a long-acting muscarinic antagonist (LAMA), ie, dual bronchodilation. This is not a new concept as the combination of short-acting agents has been popular in the past. In recent years, several fixed-dose combinations containing a LAMA and a LABA in a single inhaler have been approved by regulatory authorities in several countries. Among the new LAMA/LABA combinations, the fixed-dose combination of indacaterol 110 µg/glycopyrronium 50 µg (QVA149) has been shown in a series of clinical trials to be as safe as the single components and placebo, and more effective than placebo and the single components with regard to lung function, symptoms, and patient-oriented outcomes. Furthermore, QVA149 achieved better bronchodilation than salmeterol 50 µg/fluticasone 500 µg twice daily. Compared with tiotropium, a well-recognized treatment for COPD, the percentage of patients that exceed the minimal clinical important difference for dyspnea and health-related quality of life measurements was superior with QVA149. Other patient-oriented outcomes, such as daily symptoms, night-time awakening, and use of rescue medication consistently favored QVA149. Finally, QVA149 was significantly superior to LAMAs for reducing all types of exacerbation. In conclusion, several years after introduction of dual bronchodilation, the fixed-dose combination of indacaterol 110 µg/glycopyrronium 50 µg in a single inhaler for once-daily administration via the Breezhaler® device (QVA149) has been demonstrated to be a safe and effective treatment for COPD patients.
Keywords: chronic obstructive pulmonary disease, long-acting bronchodilators, dual bronchodilation, indacaterol, glycopyrronium, patient-oriented outcomes
Introduction
Chronic obstructive pulmonary disease (COPD) continues to be a major health and socioeconomic problem worldwide.1,2 It has been known for many years that COPD is the result of persistent and progressive pathologic abnormalities in the small airways, most often associated with alveolar loss.3–6 Cigarette smoking is the principal and most widespread cause of this disorder, although other etiologic agents have been invoked.7–9 It has been reported that about 11% of patients with COPD are never-smokers.1
Abnormal spirometry, commonly defined by a reduction of the forced expiratory volume in one second/forced vital capacity (FEV1/FVC) ratio below either 0.707 or the age-related lower limit of normal,8–10 is the hallmark of the disease. Progression of COPD is signaled by a faster than normal annual decline in FEV1 and FVC,11–13 as well as by an abnormal increase in static lung volumes.14 The deterioration in lung function is associated with worsening of dyspnea, increased rate and severity of exacerbations,15,16 a progressive inability to cope with daily activity, and eventually premature death.
International and national documents and guidelines7–9 give evidence-based recommendations for the management of COPD. At present, there is no cure for COPD. Smoking cessation is by far the most effective way of slowing down the progression of the disease and improving the chances of survival.11,13 However, some active pharmacologic treatments have been shown to provide substantial benefits for patients suffering from this disabling disorder.7–9 Long-acting bronchodilators, such as long-acting beta2 agonists (LABAs) and long-acting muscarinic antagonists (LAMAs), administered via inhalation, play a major role in the therapeutic management of COPD. In patients with frequent exacerbations, addition of inhaled corticosteroids (ICS) to maintenance treatment with a LABA has been suggested to further improve clinical outcomes.17,18
Recently, the combination of a LAMA and a LABA in a single inhaler has renewed the concept of dual bronchodilation, which was popular in the past with the short-acting agents.19–21 Current guidelines recommend combined LAMA/LABA use if symptoms are not improved by a single agent.7,9
This paper reviews the effects of one of the newly marketed LAMA and LABA combinations, ie, the fixed-dose combination (FDC) of indacaterol 110 μg/glycopyrronium 50 μg in one inhaler (Breezhaler®) administered once daily (ie, QVA149) on patient-related outcomes (PROs), which have gained increasing attention in clinical trials.22
Complex effect of bronchodilators in COPD
Inhaled bronchodilators (short-acting and then long-acting) have been widely used for many years for symptomatic relief in COPD patients at any stage of disease severity.7–9 Although in large-scale population studies, the most effective control of symptoms and exacerbations is associated with spirometric improvements,23 the relationship between individual spirometric data and symptoms is rather poor.24 The acute effect of bronchodilators on FEV1 is variable, being largely dependent on the initial absolute value, and is a poor predictor of the patient’s long-term response to treatment.25 However, several studies that have examined lung function “beyond FEV1” showed that reduction of lung hyperinflation is the main mechanism via which COPD patients derive benefit over the entire span of severity.26–31 Improvement of bronchial patency allows for better lung emptying and resetting of functional residual capacity at a lower lung volume.32 These changes in lung function, which are not seen with the FEV1, improve dynamic lung mechanics and determine better exercise tolerance, decreased dyspnea, and even a lower exacerbation rate.31,33
Why associate/combine bronchodilators?
Airway tone is regulated by the parasympathetic and sympathetic nervous systems. The exact nature of the interactions between the two physiologic systems is not yet fully understood, but there is enough evidence to suggest that combining beta2-agonists and muscarinic antagonists is pharmacologically a good option for several reasons, which have been reviewed in detail recently.34,35 Briefly, we may assume that addition of a muscarinic antagonist can reduce the bronchoconstricting effect of acetylcholine, release of which will have been modified by the beta2-agonist, and thereby amplify the bronchodilation elicited by the same beta2-agonist through direct stimulation of beta2-adrenoceptors in smooth muscle. However, it has been suggested that crosstalk between muscarinic receptors and beta2-adrenoceptors, causing functional antagonism at the level of the airway smooth muscle itself, seems more likely to be of importance.36,37 It seems reasonable to hypothesize that targeting bronchoconstriction through two distinct mechanisms should optimize the bronchodilator response and help to overcome the interpatient and intrapatient variability in bronchomotor tone associated with airway obstruction.38 In addition, some in vitro studies suggest a possible synergistic, and not simply additive, effect when the two active agents reach the cell target together.38
Dual bronchodilation
The initial trials on dual bronchodilation were performed with short-acting bronchodilators.19–21,39 In some studies, administration of one drug was followed by inhalation of the other.40 In other studies, an FDC was more effective in improving lung function that either component on its own.20,21 It was also suggested that there might be a different site of activity.41 Antimuscarinic agents produce their smooth muscle-relaxing action mainly in the central airways where acetylcholine is released from the vagus nerve and activates M3 receptors, which are present on smooth muscle cells. In peripheral airways, there is no cholinergic innervation, but M3 receptors are expressed; these receptors can be activated by acetylcholine released from epithelial cells that may express choline acetyltransferase in response to inflammatory stimuli.42 On the other hand, the effective site of bronchodilation for adrenergic agents includes both the central and peripheral airways, although beta-agonists are relatively more effective in the distal airways.42
The LAMA tiotropium is a well-established treatment for COPD.43,44 Recent clinical trials show that tiotropium is superior to LABAs (both salmeterol45 and indacaterol46) and not inferior to the FDC of salmeterol/fluticasone47 for reducing exacerbations in COPD patients. On the other hand, a short-term clinical study29 suggested that indacaterol can be more effective than tiotropium in improving lung mechanics.48 Therefore, there might be an additional potential mechanism to support the antimuscarinic/adrenergic combination for maintenance pharmacotherapy in stable COPD, ie, the different effect on lung mechanics and exacerbations. However, it remains unclear whether the combination effect is simply additive or synergistic in vivo.
In clinical studies, both formoterol and salmeterol were added to tiotropium, resulting in greater benefits in terms of symptoms and lung function.49,50 Further, administration of indacaterol in addition to tiotropium showed a significant improvement in trough FEV1 and inspiratory capacity.51 It was also shown that administration of indacaterol 300 μg plus glycopyrronium 50 μg achieved more bronchodilation than indacaterol 300 μg, while doubling the dose of indacaterol alone to 600 μg failed to further improve FEV1 when compared with the lower dose.52 In two randomized clinical trials, a new LABA, ie, olodaterol (Respimat®), was associated with tiotropium (HandiHaler®) in COPD patients with moderate-to-severe airflow limitation. This association achieved better bronchodilation that tiotropium alone, without any difference in the safety profile.53
FDC of a LAMA and a LABA
FDCs of different drugs in a single inhaler can maintain the benefits of the separate principles with the same safety profile, and improve the patient’s adherence to treatment at no additional cost.21 There are several FDCs containing LAMAs/LABAs under development with various devices.50,54,55 However, up until now, only two have been approved by regulatory authorities, ie, an FDC of indacaterol/glycopyrronium in the European Union, Japan, and Canada, and an FDC of umeclidinium/vilanterol in the European Union, USA, and Canada. FDCs of aclidinium/formoterol and tiotropium/olodaterol are in Phase III development.
In two randomized controlled trials, including more than 2,000 COPD patients with moderate-to-severe airflow limitation, the FDC of umeclidinium 62.5 μg plus vilanterol 25 μg (equivalent to a delivered dose of 55/22 μg, respectively), administered once daily by means of the Ellipta® multidose dry powder inhaler (DPI), achieved better lung function compared not only with single vilanterol and umeclidinium, but also compared with the tiotropium HandiHaler and with the salmeterol/fluticasone FDC.56 Beneficial effects were found also on lung function and exercise tolerance, and on PROs such as dyspnea and health-related quality of life (HRQoL).57,58
FDC of indacaterol/glycopyrronium
Both indacaterol48 and glycopyrronium59 are indicated for maintenance treatment in symptomatic patients with COPD. In a series of randomized controlled trials including more than 10,000 patients across 52 countries, once-daily coadministration of an FDC containing indacaterol 110 μg and glycopyrronium 50 μg by means of the Breezhaler device (QVA149) provided significant and sustained improvement in bronchodilation and PROs versus placebo, the single components, and other active agents, with a satisfactory safety profile.54,60 Dahl et al have demonstrated that QVA149 has efficacy and a safety similar to the concurrent administration of its separate components, ie, indacaterol (150 μg) and glycopyrronium (50 μg).61 However, it should be noted that whereas the dose of glycopyrronium is the same (50 μg), the dose of indacaterol is lower in QVA149, ie, 110 μg versus 150 μg. The US Food and Drug Administration has only approved the 75 μg dose. In fact, a comprehensive assessment of the dose-response relationship for indacaterol provided robust confirmation that 75 μg is the minimum effective dose.62 This issue has been discussed elsewhere.48 A recent study has documented that glycopyrronium plus indacaterol produced an additive interaction and a significant synergistic relaxant effect at isoeffective concentrations inducing an EC20.63 The effective concentration (EC) is the concentration that leads to a percentage of the maximum effect. The synergistic effect suggests that a lower dose of indacaterol may be used to achieve the same therapeutic effect with fewer side effects.
As previously mentioned, this review focuses on QVA149, and discusses the PRO data.64 In fact, due to the recognized limitation of FEV1, interest in PROs is increasing.22 Of the several PROs available, the three that are most widely measured are dyspnea, HRQoL, and exacerbations.65
Dyspnea
The Medical Research Council questionnaire measures the degree of dyspnea and was introduced a number of years ago. It demonstrated its usefulness in assessing symptom severity in epidemiologic studies and in initial evaluation of patients. However, its broad grades make this instrument rather unresponsive to changes determined by pharmacotherapy.66 Later, in the 1980s, the Basal Dyspnea Index and the Transitional Dyspnea Index (TDI) were developed, and since then these have been used increasingly in clinical trials.67 The 2004 update developed the self-administered computerized version to remove any interviewer bias and to provide direct patient-reported ratings of dyspnea.68
Health-related quality of life
The St George’s Respiratory Questionnaire (SGRQ) was developed, validated, and widely used in clinical trials to assess the HRQoL.69,70 However, the SGRQ failed to penetrate routine clinical practice. Other PROs reported in a number of clinical studies assessed “daily symptoms”, “nocturnal awaking”, ability to cope with daily activities, and use of rescue medications by means of “diary cards” self-administered by patients. However, the SGRQ remains the standard for subjective health status assessment in clinical studies.
Exacerbations
Exacerbation of COPD is defined on the basis of worsening of symptoms for more than 24/48 hours compared with stable conditions, and leading to a change in medication.7 It is classified as mild if self-managed by patients; moderate if assistance from a caregiver is required and antibiotics and/or systemic corticosteroids are prescribed to the patient; and severe if admission to the emergency room or hospitalization is indicated. Any history of previous exacerbations and low FEV1 (<50% predicted) are the best predictors of any future occurrence of exacerbations.15,16
Minimal clinically important difference
The comparison with active treatments in terms of PROs is worthy of some additional comments for the analysis of the minimal clinically important difference (MCID).71 In fact, the concept of MCID has been well established for comparison between active principles and placebo, in which the measured effects of treatment may be large. By contrast, the difference between active treatments may be smaller. Furthermore, MCIDs are average estimates obtained in groups of patients. It cannot be excluded that individual patients may perceive benefits even below the MCID threshold.71 Finally, several factors, such as trial duration, withdrawal rates, and baseline severity of the disorder may influence the benefits perceived either by the patient or the clinician and hence the value of the MCID, which should be interpreted as indicative and not as a cut-off point between benefit and no benefit. It has been suggested that comparison between active treatments should look at the percentage of patients achieving a MCID rather than comparison of means.71
PROs in clinical trials of QVA149
PROs have been investigated in all the clinical trials comparing once-daily QVA149 with both placebo and the active drugs. For subsequent analysis, we examined the published studies, excluding abstracts, and have taken into account some reviews.54,55,72,73 The characteristics of the studies and their major findings are summarized in Table 1.
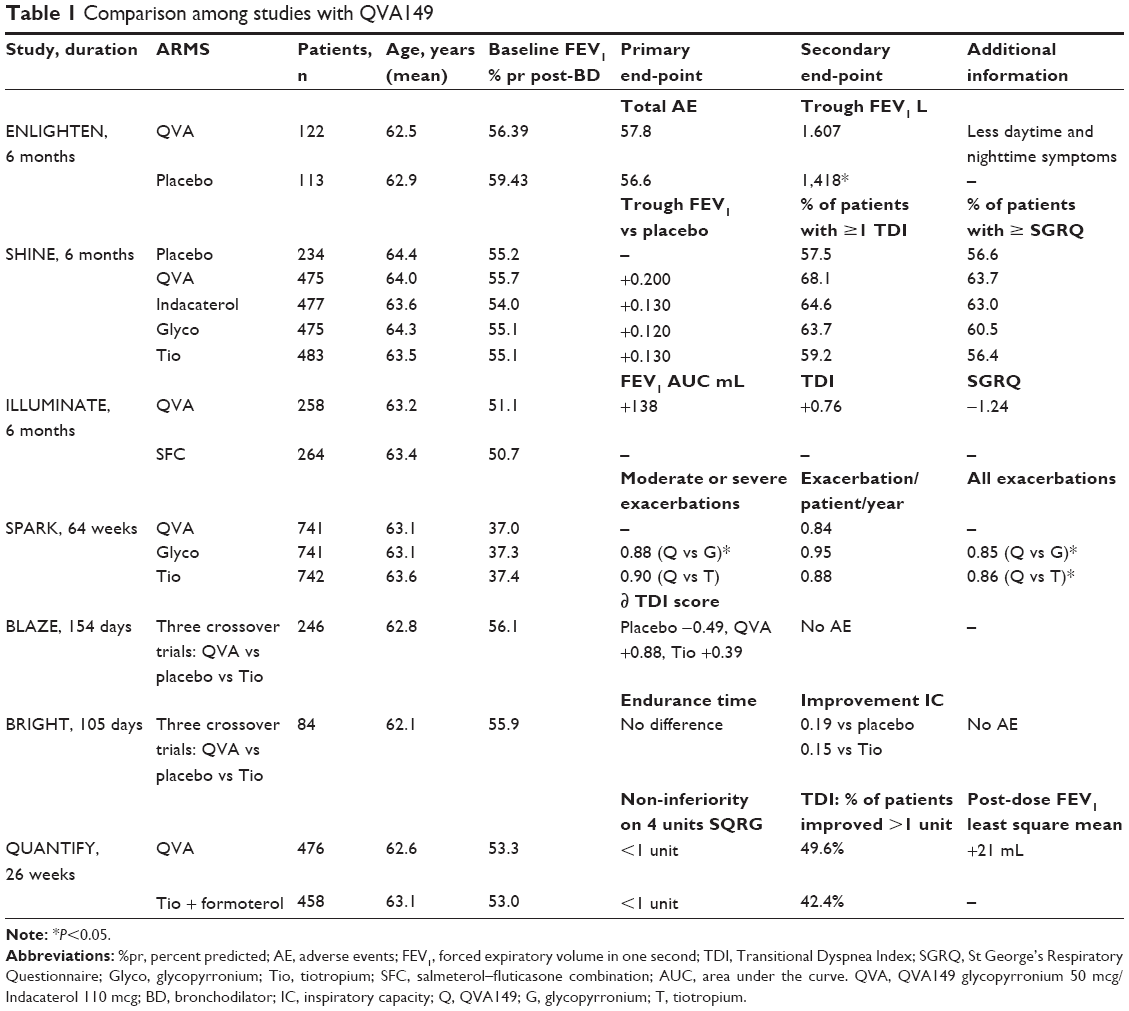 | Table 1 Comparison among studies with QVA149 |
The ENLIGHTEN study74 compared QVA149 with placebo over 52 weeks, showing a sustained improvement of pre-dose FEV1 associated with significantly greater percentages of patients reporting “no daytime symptoms”, “days able to perform usual daily activities”, and “no night-time awakenings”. Overall, the percentage of patients reporting adverse events was similar in the two groups; however, the discontinuation rate in this study was greater in the placebo group and cardiovascular adverse events were more frequent in the QVA149 arm (see below in the Safety section).
The open-label SHINE study compared QVA149 with indacaterol 150 μg, glycopyrronium 50 μg, tiotropium HandiHaler 18 μg, and placebo over 6 months.75 The improvement in trough FEV1 was significantly superior not only to placebo but also to the active comparators, which also performed significantly better than placebo. The TDI focal score was significantly improved by QVA149 versus placebo, glycopyrronium, and tiotropium at week 26. On average, the improvement in both the TDI and SGRQ was lower than the MCID. However, the percentage of patients reaching the MCID was significantly greater for QVA149 versus placebo and tiotropium.
The ILLUMINATE study compared QVA149 with an FDC of salmeterol 50 μg/fluticasone 500 μg (SFC) administered twice daily over a 26-week period.76 Spirometric measurements (both FEV1 and FVC) and TDI improved significantly more in the QVA149 group than in the SFC group. However, the SGRQ failed to find any difference between the two groups. The ILLUMINATE authors explained this discrepancy between lung function, TDI, and SGRQ on the basis of the selection criteria used. In fact, the COPD patients recruited for the ILLUMINATE study needed to have been essentially exacerbation-free in the previous year. As is well known, exacerbations contribute substantially to HRQoL, and the SGRQ may not detect HRQoL changes in non-exacerbating patients.
SPARK was a large-scale study in COPD patients with FEV1 <50% predicted who had suffered at least one exacerbation in the previous year,77 hence were at risk of adverse outcomes in the future.78 However, it should be noted that the majority of patients (75% in all groups) continued their treatment with ICS. Eventually, for the first end-point, ie, comparison with glycopyrronium on moderate and severe exacerbations, QVA149 achieved a statistically significant reduction of 12%, whereas for the secondary endpoint, comparison with open-label tiotropium, QVA149 achieved a nonsignificant 10% reduction. However, when mild exacerbations were also considered, the 15% and 14% reductions in all exacerbations for QVA149 compared with glycopyrronium and tiotropium, respectively, were significant. The SGRQ was lower in the QVA149 group, although the difference was, on average, less than the −4 points considered to be the MCID. However, the percentage of patients with a reduction ≥4 points was greater in the QVA149 group than in both LAMA monotherapy groups at any control visit up to 52 weeks.
BLAZE was the first and only study evaluating an important PRO such as dyspnea as a primary endpoint versus placebo and open-label tiotropium HandiHaler 18 μg.79 COPD patients with stage II or III disease according to the traditional GOLD severity classification were recruited.80 The possible superiority of QVA149 versus placebo and tiotropium was assessed by means of the self-administered computerized version of the Basal Dyspnea Index and TDI after 6 weeks. The mean difference between QVA149 and tiotropium (0.40 TDI score) was statistically significant, but lower than the MCID. Although of short duration, the study had a crossover design, which minimized subjective variability and reinforced the conclusion.
The BRIGHT study investigated the effect of QVA149 on dynamic hyperinflation during exercise and exercise endurance in comparison with placebo (primary objective) and open-label tiotropium (exploratory objective).81 QVA149 was significantly superior to placebo with regard to all the considered variables and to tiotropium for pre-exercise and peak-exercise changes in inspiratory capacity on days 1 and 21. However, the improvement in exercise endurance was significantly superior to placebo for both QVA149 and tiotropium at day 21, but with no difference between the two active compounds. This result may seem rather surprising. In fact, there is abundant literature showing that in patients with COPD, even obese patients82 and patients with mild obstruction,83 exercise tolerance is associated with dynamic hyperinflation during exercise.84,85 However, the authors provide three possible explanations for this unusual result. First, the patients performed their exercise post-dose and not under trough conditions, in such a way that differences in the bronchodilator effect between the two active regimens may have been diluted. Second, the presence of other non-pulmonary factors such as leg fatigue may have contributed to exercise limitation in this group of non-severe patients. In fact, the patient population itself may have reached the “ceiling effect” for endurance time achievable by bronchodilation, in such a way that prevented any distinction between active treatments based on endurance time, despite improved bronchodilation with QVA149 (dual bronchodilation) versus tiotropium (single therapy). Third, the crossover design resulted in a large number of exercise tests (eleven per patient), which may have led to a bias in the results due to a sort of “training effect”.
Recently, the HRQoL non-inferiority QUANTIFY study compared QVA149 with the free combination of once-daily tiotropium and twice-daily formoterol in patients with moderate-to-severe COPD.86 After 26 weeks, the primary endpoint was met, ie, QVA149 and the free combination of tiotropium plus formoterol had a similar effect on HRQoL. However, QVA149 achieved a significant improvement in dyspnea (TDI score) and trough FEV1 and FVC compared with the tiotropium plus formoterol association.86 A brief summary of the major QVA149 studies is given in Table 1.
Discussion
Guidelines recommend that COPD patients not controlled by a single bronchodilator could be upgraded to either an ICS plus LABA combination or two bronchodilators with different mechanisms of action.7,9 The combination of two drugs may lower the dose of the individual agents, decrease adverse effects, simplify medication regimens, and improve compliance.87 The National Institute for Health and Care Excellence guidelines88 recommend treatment with LAMAs plus LABAs in patients with COPD who remain symptomatic on treatment with a LABA alone, but the LABA/LAMA combination is not recommended for those already taking a LAMA as sole maintenance therapy. This recommendation might be reconsidered in view of recent evidence documenting that regular addition of a LABA to a LAMA not only induces better bronchodilation than that obtained with the LAMA on its own,49–52 but also significantly improves PROs.54,58
Compared with the tiotropium HandiHaler 18 μg, QVA149 was associated with greater and more rapid bronchodilation,74 a higher percentage of patients with a significant improvement in dyspnea and HRQoL,74,78 a significant reduction in all exacerbations, and a non-significant decrease in moderate and severe exacerbations, although the reduction was significant compared with the LAMA glycopyrronium.77 Further, QVA149 achieved a greater reduction in exercise-induced dynamic lung hyperinflation, as shown by the improvement in inspiratory capacity, although exercise capacity was not affected by that change and was similar after QVA149 and after tiotropium.80 We may conclude that QVA149 was not inferior to tiotropium overall, and was significantly superior in some lung function measurements and PROs. However, it should be borne in mind that QVA149 was tested only in short-term to medium-term studies, as seen in Table 1, whereas current use of tiotropium in COPD is supported by prolific literature on both lung function and PROs and also involving large long-term population studies.89,90
Upgrade of treatment from LABA or LAMA monotherapy to the ICS/LABA FDC is recommended for COPD patients at high risk of exacerbations7 after valid long-term clinical trials.91,92 However, the salmeterol/fluticasone FDC is also widely used in many patients at low risk of exacerbation.93–95 In this category of patients at low risk, QVA149 achieved superior bronchodilation and symptomatic improvement than the SFC/FDC.75 At present, a clinical trial comparing QVA149 versus SFC/FDC in patients at high risk of exacerbations is ongoing.96
In recent years, “limited reversibility”, ie, an increase in FEV1 <10% of the baseline value, has been eliminated from the inclusion criteria for clinical trials on COPD, such that patients with a significant FEV1 reversibility have been included.89 This may raise the issue of whether COPD patients with large reversibility could be those who obtain the most benefit from dual bronchodilator maintenance therapy. On the other hand, it might be that these patients have an asthmatic component to their COPD that has been missed. In this case, they would benefit more from the ICS/LABA combination than from dual bronchodilation.95
There are not many studies comparing dual bronchodilator strategies. The non-inferiority result from QUANTIFY suggests that treatment with QVA149 can be a simpler alternative with improved patient adherence and compliance compared with the free combination of tiotropium once daily and formoterol twice daily.86 To our knowledge, there is no study comparing the different LAMA/LABA FDCs. However, it should be mentioned that the different combinations are delivered via different devices, which may influence their clinical efficacy. QVA149 is delivered via the Breezhaler DPI, which is a low-resistance (specific airflow resistance 2.2×10−2 kPa1/2L−1 minute) capsule-based device. The Breezhaler requires less inspiratory effort than other DPIs to achieve a given inspiratory flow or, as reflected in the inspiratory flow profiles, permits a higher inspiratory flow for a given effort.97 Consequently, it is suitable for use by patients with a wide range of COPD severity, delivering a consistent dose irrespective of disease severity and age.98 The FDC combination of umeclidinium/vilanterol is inhaled using the Ellipta, which delivers consistent doses within the respirable range over the lifetime of the product. The delivery performance of Ellipta was investigated and showed consistent powder delivery across a wide range of inhalation parameters.99 The Ellipta DPI was preferred over current inhalers by the majority of COPD patients recruited from Phase III studies to participate in post-study interviews.100 Ease of use, simplicity of operation, and design of the mouthpiece were the most frequently encountered response themes underlying preference. The Respimat® Soft Mist™ inhaler, which delivers the FDC of tiotropium/olodaterol, is unique in that it uses mechanical energy, in the form of a spring, to generate a fine, slow-moving cloud (the Soft Mist) for inhalation. The Respimat Soft Mist inhaler also has a number of benefits. Most notably, it is simple to coordinate and the delivered dose is independent of inspiratory effort; it is therefore not affected by the breathing maneuver problems inherent with some other devices, so is suitable for all patients to use.101 The multidose Respimat Soft Mist inhaler provides a high level of satisfaction in COPD patients due to its inhalation and handling characteristics.102 In summary, comparison of LAMA/LABA FDCs should also take into account the characteristics of the inhalation device.
The GOLD document7 suggests dual bronchodilation as a second option for patients at low risk of exacerbations but with significant symptoms, as indicated by the presence of either a modified Medical Research Council dyspnea grade ≥2 or a COPD Assessment Test score >10. However, after the above reported studies on QVA149 and on the umeclidinium/vilanterol FDC, one might consider the option to offer dual bronchodilation to symptomatic naïve patients with GOLD stage II or III COPD without waiting for a step-up approach. The rapid improvement in symptoms could help patients’ adherence to treatment, which may be otherwise discouraged by a “slow” gradual therapeutic strategy. However, this attractive theoretical approach needs to be investigated and proved with adequately powered and designed randomized controlled trials. According to international documents, the LABA/LAMA combination is also recommended for patients at high risk of exacerbations as an alternative choice to the LABA/ICS combination when ICS are refused by the patient or contraindications exist.95
Safety
Both the monocomponents of QVA149, ie, glycopyrronium and indacaterol, have a well characterized safety profile. Both show no evidence of being associated with adverse cardiovascular effects and no difference was found in comparison with placebo.48,5 The safety profile of QVA149 was not different either from placebo or the single components.54,73 However, when combining bronchodilators, not only the efficacy of the combination has to be taken into account, but also the associated safety profile. In the SHINE study,74 the overall incidence of adverse events was similar for QVA149, placebo, and the active comparators. The occurrence of severe adverse cardiovascular events was low across the treatment groups, and none was reported in the QVA149 arm. Also, the 1-year SPARK study showed a similar safety profile among QVA149, the active comparators, and placebo.76 Further, the 1-year ENLIGHTEN study73 showed that the overall incidence of adverse events was comparable between the QVA149 group and the placebo group, ie, 57.8% and 56.6%, respectively. However, severe adverse events occurred in 16.4% and 10.6% of patients in the QVA149 and placebo groups, respectively. The incidence of severe adverse cardiovascular events was low in the QVA149 arm and zero in the placebo arm, although the difference was not statistically significant. There were four deaths in the QVA149 group and one death in the placebo arm, but none was related to the study drug. The imbalance in rates of severe adverse events and deaths was explained by differences in the recruited populations, ie, at baseline, more patients had severe COPD and a history of myocardial infarction, stroke, and diabetes in the QVA149 group. However, in a pooled analysis of 6 months of safety data from SHINE,74 ILLUMINATE,75 and ENLIGHTEN,73 the overall proportion of adverse events in the QVA149 group was lower compared with the indacaterol, glycopyrronium, open-label tiotropium, and SFC groups, while the incidence of severe adverse events was similar across all groups.103 The incidence of severe adverse cardiovascular events was low and similar in the QVA149 and active groups.
In summary, QVA149 was generally well tolerated with a favorable adverse event profile. However, as previously mentioned, the studies of QVA149 are short-term to medium-term. Long-term studies would help to clarify the role of dual bronchodilation in the therapeutic management of COPD. Further, dual bronchodilation should be used with caution in patients with important cardiovascular disease, since this type of patient is generally excluded from clinical trials.
Conclusion
In conclusion, several years after the introduction of the short-acting beta2/muscarinic agonist FDC, dual bronchodilation, which combines a long-acting antimuscarinic agent (glycopyrronium 50 μg) with a beta2-selective, long-acting, adrenergic agonist (indacaterol 110 μg) in a single inhaler for once-daily administration via the Breezhaler device, has been shown to be a safe and effective therapy for COPD patients with moderate-to-severe airflow limitation to improve not only lung function, but also important PROs such as dyspnea, HRQoL, and exacerbations.
Acknowledgments
The authors thank Dr Chris Botterill for copyediting the manuscript and the team at AIPO-Ricerche for technical and editing assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
Buist A, McBurnie M, Vollmer W, et al. International variation in the prevalence of COPD (the BOLD study): a population-based prevalence study. Lancet. 2007;370:741–750. | ||
Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369:448–457. | ||
Hogg JC, Macklem PT, Thurlbeck WM. Site and nature of airway obstruction in chronic obstructive lung disease. N Engl J Med. 1968;278: 1355–1360. | ||
Cosio M, Ghezzo H, Hogg JC, et al. The relations between structural changes in small airways and pulmonary-function tests. N Engl J Med. 1978;298:1277–1281. | ||
Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004; 350:2645–2653. | ||
McDonough JE, Yuan R, Suzuki M, et al. Small-airway obstruction and emphysema in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2011;365:1567–1575. | ||
Vestbo J, Hurd S, Agustì AG, et al. Global Strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease GOLD Executive Summary. Am J Respir Crit Care Med. 2013;187:347–365. | ||
Siafakas NM, Vermeire P, Pride NB, et al. Optimal assessment and management of chronic obstructive pulmonary disease (COPD). Eur Respir J. 1995;8:1398–1420. | ||
Bettoncelli G, Blasi F, Brusasco V, et al. The clinical and integrated management of COPD. An official document of AIMAR, AIPO, SIMeR, SIMG. Sarcoidosis Vasc Diffuse Lung Dis. 2014;31 Suppl 1:3–21. | ||
Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26:948–968. | ||
Fletcher C, Peto R, Tinker C, et al. The Natural History of Chronic Bronchitis and Emphysema. An Eigth-Year Study of Early Chronic Obstructive Lung Disease in Working Men in London. Oxford, UK: Oxford University Press; 1976. | ||
Tantucci C, Modina D. Lung function decline in COPD. Int J COPD. 2012;7:95–99. | ||
Miller A, Raskin JM. The natural history of COPD: confirming and going beyond Fletcher and Peto. Eur Respir J. 2014;44:280–383. | ||
Macklem PT. Therapeutic implications of the pathophysiology of COPD. Eur Respir J. 2010;35:676–680. | ||
Hurst JR, Vestbo J, Anzueto A, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–1138. | ||
Han MK, Kazerooni EA, Lynch DA, et al. Chronic obstructive pulmonary disease exacerbations in the COPD Gene Study: associated radiologic phenotypes. Radiology. 2011;261:274–282. | ||
Cazzola M, Matera M, Santangelo G, et al. Salmeterol and formoterol in partially reversible severe chronic obstructive pulmonary disease: a dose-response study. Respir Med. 1995;89:357–362. | ||
Vestbo J; TORCH Study Group. The TORCH (TOwards a Revolution in COPD Health) survival study protocol. Eur Respir J. 2004;24: 206–210. | ||
Augusti A, Fabbri LM. Inhaled steroids in COPD: when should they be used? Lancet. 2014;2:869–871. | ||
Kaik G. Combined administration of ipratropium bromide (SCH1000) and fenoterol in patients with chronic obstructive airway disease. Med Klin Wochenschr. 1975;87:653–656. | ||
American College of Chest Physicians. In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85-day multicenter trial. COMBIVENT Inhalation Aerosol Study Group. Chest. 1994;105:1411–1419. | ||
Benayoun S, Ernst P, Suissa S. The impact of combined inhaled bronchodilator therapy in the treatment of COPD. Chest. 2001;119:85–92. | ||
Jones PW, Donohue JF, Nedelman J, Pascoe S, Pinault G, Lassen C. Correlating changes in lung function with patient outcomes in chronic obstructive pulmonary disease: a pooled analysis. Respir Res. 2011;12:161. | ||
Cooper CB. The connection between chronic obstructive pulmonary disease symptoms and hyperinflation and its impact on exercise and function. Am J Med. 2006;119 Suppl 1:21–31. | ||
Calverley PMA, Albert P, Walker PP. Bronchodilator reversibility in chronic obstructive pulmonary disease. Lancet Respir Med. 2013;1: 564–573. | ||
Tantucci C, Duguet A, Similowski T, Zelter M, Derenne J-P, Milic-Emili J. Effect of salbutamol on dynamic hyperinflation in chronic obstructive pulmonary disease. Eur Respir J. 1998;12:799–804. | ||
O’Donnell DE, Voduc N, Fitzpatrick M, Webb KA. Effect of salmeterol on the ventilatory response to exercise in chronic obstructive pulmonary disease. Eur Respir J. 2004;24:86–94. | ||
O’Donnell DE, Fluge T, Gerken A, et al. Effects of tiotropium on lung hyperinflation, dyspnoea, and exercise tolerance in COPD. Eur Respir J. 2004;23:832–840. | ||
Rossi A, Centanni S, Cerveri I, et al. Acute effects of indacaterol on lung hyperinflation in moderate COPD: a comparison with tiotropium. Respir Med. 2012;106:84–90. | ||
O’Donnell DE, Laveneziana P, Ora J, Webb KA, Lam YM, Ofir D. Evaluation of acute bronchodilator reversibility in patients with symptoms of GOLD stage I COPD. Thorax. 2009;64:216–223. | ||
O’Donnell DE, Laveneziana P. Lung hyperinflation in COPD: the impact of pharmacotherapy. Eur Respir Rev. 2006;15:85–89. | ||
Beeh KM, Wagner F, Khindri S, Drollmann AF. Effect of indacaterol on dynamic lung hyperinflation and breathlessness in hyperinflated patients with COPD. COPD. 2011;8:340–345. | ||
Wedzicha JA, Decramer M, Seemugal TA. The role of bronchodilator treatment in the prevention of exacerbations of COPD. Eur Respir J. 2012;40:1545–1554. | ||
Cazzola M, Page CP, Calzetta L, Matera MG. Pharmacology and therapeutics of bronchodilators. Pharmacol Rev. 2012;64:450–504. | ||
Cazzola M, Molimard M. The scientific rationale for combining long-acting β2-agonists and muscarinic antagonists in COPD. Pulm Pharmacol Ther. 2010;23:257–267. | ||
Cazzola M, Calzetta L, Matera MG. β2-adrenoceptor agonists: current and future direction. Br J Pharmacol. 2011;163:4–17. | ||
Meurs H, Oenema TA, Kistemaker LE, Gosens R. A new perspective on muscarinic receptor antagonism in obstructive airways diseases. Curr Opin Pharmacol. 2013;13:316–323. | ||
Meurs H, Dekkers BG, Maarsingh H, Halayko AJ, Zaagsma J, Gosens R. Muscarinic receptors on airway mesenchymal cells: novel findings for an ancient target. Pulm Pharmacol Ther. 2013;26:145–155. | ||
Cazzola M, Matera MG. The effective treatment of COPD: anticholinergics and what else? Drug Discov Today Ther Strateg. 2006;3: 277–286. | ||
Easton PA, Jadue C, Dhingra S, Anthonisen NR. A comparison of the bronchodilating effect of a beta-2 adrenergic agent (albuterol) and an anticholinergic agent (ipratropium bromide) given by aerosol alone or in sequence. N Engl J Med. 1985;315:735–739. | ||
Ingram RH, McFadden ER. Predominantly large versus small airways responses in normal subjects. In: Sadoul P, Milic-Emili J, Simonsson BG, Clark TJH, editors. Small Airways in Health and Disease. Amsterdam, The Netherlands: Excerpta Medica; 1979. | ||
Barnes PJ. Distribution of receptors targets in the lung. Proc Am Thorac Soc. 2004;1:345–351. | ||
Keating GM. Tiotropium bromide inhalation powder. A review of its use in the management of chronic obstructive pulmonary disease. Drugs. 2012;72:273–300. | ||
Keating MG. Tiotropium Respimat® Soft Mist™ inhaler: a review of its use in chronic obstructive pulmonary disease. Drugs. 2014;74:1801–1816. | ||
Vogelmeier C, Hedere B, Glaab T, et al; for the POET-COPD investigators. Tiotropium versus salmeterol for prevention of exacerbations of COPD. N Engl J Med. 2011;364:1093–1103. | ||
Decramer M, Chapman KR, Frith P, et al. Once daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): a randomized, blinded, parallel-group study. Lancet Respir Med. 2013;1:524–533. | ||
Wedzicha JA, Calverley PMA, Seemugal TA, et al. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am J Respir Crit Care Med. 2008;177:19–26. | ||
Rossi A, Polese G. Indacaterol: a comprehensive review. Int J COPD. 2013;8:353–363. | ||
Taskin DP, Ferguson GT. Combination bronchodilator therapy in the management of chronic obstructive pulmonary disease. Respir Res. 2013;14:49. | ||
Singh D. New combination bronchodilators for COPD: current evidence and future perspectives. Br J Clin Pharmacol. November 6, 2014. [Epub ahead of print]. | ||
Mahler DA, D’Urzo A, Bateman ED, et al; on behalf of the INTRUST-1 and INTRUST-2 Study Investigators. Concurrent use of indacaterol plus tiotropium in patients with COPD provides superior bronchodilation compared with tiotropium alone: a randomized, double-blind comparison. Thorax. 2012;67:781–788. | ||
van Noord JA, Buhl R, LaForce C, et al. QVA149 demonstrates superior bronchodilation compared with indacaterol or placebo in patients with chronic obstructive pulmonary disease. Thorax. 2010;65:1086–1091. | ||
ZuWallack R, Allen L, Hernandez G, Ting N, Abrahams R. Efficacy and safety of combining olodaterol Respimat(®) and tiotropium HandiHaler(®) in patients with COPD: results of two randomized, double-blind, active-controlled studies. Int J Chron Obstruct Pulmon Dis. 2014;9:1133–1144. | ||
Banerji D, Fogel R, Beeh KM. Dual bronchodilation for the treatment of chronic obstructive pulmonary disease: a review of latest clinical data. Clin Invest. 2014;4:511–533. | ||
Ulrik CS. Clinical benefit of fixed-dose dual bronchodilation with glycopyrronium and indacaterol once daily in patients with chronic obstructive pulmonary disease: a systematic review. Int J COPD. 2014; 9:331–338. | ||
Decramer M, Anzueto A, Kerwin E, et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. Lancet Respir Med. 2014;2:472–486. | ||
Maltais F, Singh S, Donald AC, et al. Effects of a combination of umeclidinium/villanterol on exercise endurance in patients with chronic obstructive pulmonary disease: two randomized, double-blind clinical trials. Ther Adv Respir Dis. 2014;8:169–181. | ||
Blair HA, Deeks ED. Umeclidinium/vilanterol: a review of its use as maintenance therapy in adults with chronic obstructive pulmonary disease. Drugs. 2015;75:61–74. | ||
Vinken W, Aumann J, Chen H, Henley M, McBryan D, Goyal P. Efficacy and safety of coadministration of once-daily indacaterol and glycopyrronium versus indacaterol alone in COPD patients: the GLOW6 study. Int J COPD. 2014;9:215–228. | ||
Buhl R, Banerji D. Profile of glycopyrronium for once-daily treatment of moderate-to-severe COPD. Int J COPD. 2012;7:729–741. | ||
Dahl R, Jadeyel D, Alagappan VKT, Chen H, Banerji D. Efficacy and safety of QVA149 compared to the concurrent administration of its mono components indacaterol and glycopyrronium: the BEACON study. Int J COPD. 2013;8:501–508. | ||
Renard D, Looby M, Kramer B, Lawrence D, Morris D, Stanski DR. Characterization of the bronchodilatory dose response to indacaterol in patients with chronic obstructive pulmonary disease using model-based approaches. Respir Res. 2011;12:54. | ||
Cazzola M, Calzetta L, Segreti A, Facciolo F, Rogliani P, Matera MG. Translational study searching for synergy between glycopyrronium and indacaterol. COPD. September 15, 2014. [Epub ahead of print]. | ||
Glaab T, Vogelmeier C, Buhl R. Outcome measures in chronic obstructive pulmonary disease (COPD): strengths and limitations. Respir Res. 2010;11:79. | ||
Frampton JE. QVA149 (indacaterol/glycopyrronium fixed-dose combination): a review of its use in patients with chronic obstructive pulmonary disease. Drugs. 2014;74:465–488. | ||
Cazzola M, MacNee W, Martinez FJ, et al. Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J. 2008;31:416–468. | ||
Mahaler DA. Measurement of dyspnea: clinical ratings. In: Mahaler DA, editor. Dyspnea: Mechanisms, Measurement, and Management. 2nd ed. New York, NY, USA; Taylor & Francis Inc; 2005. | ||
Mahler DA, Ward J, Watermann LA, et al. Patient-reported dyspnea in COPD reliability and association with stage of disease. Chest. 2009;136: 1473–1479. | ||
Mahaler DA, Ward J, Fierro-Carrion G, et al. Development of self-administered versions of modified baseline and transitional dyspnea indexes in COPD. J COPD. 2004;1:1–8. | ||
Jones PW. Quality of life measurement for patients with diseases of the airways. Thorax. 1991;46:676–682. | ||
Jones PW, Quirk FH, Baveystock CM. The Saint George’s Respiratory Questionnaire. Respir Med. 1991;85 Suppl B:25–31. | ||
Jones PW, Beeh KM, Chapman KR, Decramer M, Mahaler D, Wedzicha JA. Minimal clinically important differences in pharmacological trials. Am J Respir Crit Care Med. 2014;189:250–255. | ||
Rodrigo GJ, Plaza V. Efficacy and safety of a fixed-dose combination of indacaterol and glycopyrronium for the treatment of COPD. A systematic review. Chest. 2014;146:309–317. | ||
Dahl R, Chapman KR, Rudolf M, et al. Safety and efficacy of dual bronchodilation with QVA149 in COPD patients: the ENLIGHTEN study. Respir Med. 2013;107:1558–1567. | ||
Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42:1484–1494. | ||
Vogelmeier CF, Bateman ED, Pallante J, et al. Efficacy and safety of once-daily QVA149 compared with twice-daily salmeterol-fluticasone in patients with chronic obstructive pulmonary disease (ILLUMINATE): a randomized, double-blind, parallel group study. Lancet Respir Med. 2013;1:51–60. | ||
Wedzicha JA, Decramer M, Ficker JH, et al. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomized, double-blind, parallel-group study. Lancet Respir Med. 2013;1:199–209. | ||
Oba Y, Lone NA. Comparative effect of inhaled corticosteroid and long-acting beta agonist combinations in preventing COPD exacerbations: a Bayesian network meta-analysis. Int J COPD. 2014;9:469–479. | ||
Mahaler DA, Decramer M, D’Urzo A, et al. Dual bronchodilation with QVA149 reduces patient-reported dyspnea in COPD: the BLAZE study. Eur Respir J. 2014;43:1599–1609. | ||
Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis management and prevention of chronic obstructive pulmonary disease. GOLD executive summary. Am J Respir Crit Care Med. 2007;176: 532–555. | ||
Beeh KM, Korn S, Beier J, et al. Effect of QVA149 on lung volumes and exercise tolerance in COPD patients; the BRIGHT study. Respir Med. 2014;108:584–592. | ||
Ora J, Laveneziana P, Ofir D, Deesomchok A, Webb K, O’Donnell DE. Combined effects of obesity and chronic obstructive pulmonary disease on dyspnea and exercise tolerance. Am J Respir Crit Care Med. 2009;180:964–971. | ||
Ofir D, Laveneziana P, Webb K, Lam YM, O’Donnell DE. Mechanisms of dyspnea during cycle exercise in symptomatic patients with GOLD I stage chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2008;177:622–629. | ||
Guenette JA, Chin RC, Cheng S, et al. Mechanisms of exercise intolerance in global initiative for chronic obstructive lung disease grade 1 COPD. Eur Respir J. 2014;44:1177–1187. | ||
O’Donnell DE, Laveneziana P. Physiology and consequences of lung hyperinflation in COPD. Eur Respir Rev. 2006;15:61–67. | ||
Buhl R, Gessner C, Schuermann W, et al. Efficacy and safety of once-daily QVA1448 compared with the free combination of one-daily tiotropium plus twice-daily formoterol in patients with moderate-to-severe COPD (QUANTIFY): a randomized, non-inferiority study. Thorax. 2015;70:311–319. | ||
Cazzola M, Matera MG. Bronchodilators: current and future. Clin Chest Med. 2014;35:191–201. | ||
National Clinical Guideline Centre. Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care. London, UK: National Clinical Guideline Centre; 2010. Available from: http://guidance.nice.org.uk/CG101/Guidance/pdf/English. Accessed April 24, 2015. | ||
Tashkin DP, Celli B, Senn S, et al; UPLIFT Study Investigators. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359:1543–1554. | ||
Wise RA, Anzueto A, Calverley P, et al. The Tiotropium Safety and Performance in Respimat Trial (TIOSPIR): a large scale, randomized, controlled, parallel-group trial design and rationale. Respir Res. 2013;14:40. | ||
Calverley P, Pauwels R, Vestbo J, et al; Trial of Inhaled Steroids and Long-Acting Beta2 Agonists Study Group. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 2003;361:449–456. | ||
Calverley PM, Anderson JA, Celli B, et al; TORCH Investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775–789. | ||
Corrado A, Rossi A. How far is real life from COPD therapy guidelines? An Italian observational study. Respir Med. 2012;106:e989–e997. | ||
Rossi A, Guerriero M, Corrado A; OPTIMO/AIPO Study Group. Withdrawal of inhaled corticosteroids can be safe in COPD patients at low risk of exacerbation: a real-life study on the appropriateness of treatment in moderate COPD patients (OPTIMO). Respir Res. 2014;15:77. | ||
Ernst P, Saad N, Suissa S. Inhaled corticosteroids in COPD: the clinical evidence. Eur Respir J. 2015;45:525–537. | ||
Wedzicha JA, Decramer M, Vestbo J, et al. A novel study design for the comparison between once-daily QVA149 and twice-daily salmeterol/fluticasone on the reduction of COPD exacerbations: the FLAME study. Eur Respir J. 2013;42 Suppl 57:P696. | ||
Chapman KR, Fogarty CM, Peckitt C, et al. Delivery characteristics and patients’ handling of two single-dose dry-powder inhalers used in COPD. Int J Chron Obstruct Pulmon Dis. 2011;6:353–363. | ||
Pavkov R, Mueller S, Fiebich K, et al. Characteristics of a capsule based dry powder inhaler for the delivery of indacaterol. Curr Med Res Opin. 2010;26:2527–2533. | ||
Hamilton M, Prime D, Bogalo Huescar M, et al. In vitro delivery performance of umeclidinium and umeclidinium/vilanterol from a dry powder inhaler using the Electronic Lung breathing simulator to replicate inhalation profiles from patients with varying COPD severity. Am J Respir Crit Care Med. 2013;187:A4281. | ||
Svedsater H, Dale P, Garrill K, et al. Qualitative assessment of attributes and ease of use of the Ellipta™ dry powder inhaler for delivery of maintenance therapy for asthma and COPD. BMC Pulm Med. 2013;13:72. | ||
Dalby R, Spallek M, Voshaar T. A review of the development of Respimat Soft Mist inhaler. Int J Pharm. 2004;283:1–9. | ||
Hodder R, Price D. Patient preferences for inhaler devices in chronic obstructive pulmonary disease: experience with Respimat Soft Mist inhaler. Int J Chron Obstruct Pulmon Dis. 2009;4:381–390. | ||
Wedzicha JA, Dahl R, Buhl R, et al. Pooled safety analysis of the fixed-dose combination of indacaterol and glycopyrronium (QVA149), its monocomponents, and tiotropium versus placebo in COPD patients. Respir Med. 2014;108:1498–1507. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.