")
Back to Journals » Drug Design, Development and Therapy » Volume 9
Clinical pharmacokinetics of AZD3199, an inhaled ultra-long-acting β2-adrenoreceptor agonist (uLABA)
Authors Bjermer L , Kuna P, Jorup C, Bengtsson T, Rosenborg J
Received 12 April 2014
Accepted for publication 13 May 2014
Published 5 February 2015 Volume 2015:9 Pages 753—762
DOI https://doi.org/10.2147/DDDT.S66049
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Leif Bjermer,1 Piotr Kuna,2 Carin Jorup,3 Thomas Bengtsson,4 Johan Rosenborg4
1Department of Respiratory Medicine and Allergology, University Hospital, Lund, Sweden; 2Department of Internal Medicine, Asthma and Allergy, Barlicki University Hospital, Medical University of Lodz, Lodz, Poland; 3AstraZeneca R&D, Mölndal, Sweden; 4StatMind, Lund, Sweden
Objective: The clinical pharmacokinetics of AZD3199, an ultra-long-acting β2-agonist, were investigated in healthy volunteers and patients with asthma or chronic obstructive pulmonary disease (COPD).
Materials and methods: Five studies are presented: one single ascending dose study in healthy Caucasian males; two multiple ascending dose studies in healthy males, one in Caucasians and one in Japanese; a Phase IIA asthma study; and a Phase IIB COPD study. Subjects received AZD3199 via a Spira nebulizer (Turbuhaler; equivalent delivered doses 5–3200 µg) or Turbuhaler (single delivered doses of 120–1920 µg or repeated delivered once-daily doses 240–1,680 µg). AZD3199 pharmacokinetics were assessed using total plasma concentration and urinary excretion, and tolerability using adverse events, clinical laboratory tests, and physical examinations.
Results: AZD3199 appeared rapidly in the systemic circulation following single and multiple dosing in healthy volunteers and patients (maximum plasma concentration within 30 minutes), with dose-proportional time-independent pharmacokinetics. Plasma exposure to unmetabolized drug was similar in healthy volunteers and patients with asthma, but relatively lower in patients with COPD. Estimated terminal half-life was up to 142 hours in healthy Caucasian males. AZD3199 was well tolerated and showed no or at most mild systemic effects.
Conclusion: AZD3199 plasma exposure in healthy volunteers and patients suggested linear pharmacokinetics and a long half-life. Systemic availability was similar in healthy subjects and patients with asthma, but was lower in patients with COPD. These clinical trials suggest that AZD3199 is well-tolerated in healthy male volunteers and patients, with no safety concerns identified to preclude further evaluation.
Keywords: AZD3199, uLABA, COPD, asthma, pharmacokinetics, tolerability
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are characterized by airway obstruction and airflow limitation. Pharmacologically mediated bronchodilation is an important element in the management of these conditions. In asthma, guidelines recommend that this effect is primarily obtained with β2-adrenoceptor agonists, while in COPD guidelines both β2-agonist and muscarinic antagonist bronchodilators are recommended, alone or in combination. Bronchodilators are usually administered via inhalation, due to the more rapid onset of effect and improved therapeutic index in comparison with oral formulations, although available muscarinic antagonists still have a relatively slow onset.1,2 The maintenance of a positive difference between the pulmonary and extrapulmonary effects of an inhaled drug intended to exert an effect in the lungs depends on how long a therapeutically relevant difference in drug concentration can be maintained at the sites of action within and outside the lungs.3,4 The long-acting β2-agonists (LABAs) formoterol (Oxis® [AstraZeneca], Foradil® [Novartis]) and salmeterol (Serevent® [GlaxoSmithKline]) are lipophilic drugs, a quality likely to promote a high affinity for the airways, and thereby a long residence time in the lungs after inhalation. More lipophilic properties (thereby promoting tissue retention of these drugs) in combination with administration via inhalation allow for a more sustained bronchodilatory effect, typically over 12 hours’ duration, with a lower magnitude of systemically mediated adverse effects compared with more hydrophilic short-acting alternatives.5–7 Similarly, AZD3199 was designed for extended residency in the lung, resulting in a long duration of effect after inhalation. The bronchodilating effects of formoterol and salmeterol are further sustained when administered concomitantly with budesonide and fluticasone, respectively.8,9 New approaches to the management of asthma and COPD have focused on the development of once-daily, well-tolerated treatments. Therefore, indacaterol (Onbrez® [Novartis]), a more recently developed ultra-LABA (uLABA) for the treatment of COPD, maintains a clinically relevant effect over 24 hours with once-daily dosing.10
In addition to a prolonged duration of action, novel bronchodilator compounds should demonstrate a systemic side-effect profile at least as good as existing LABAs with a comparable peak bronchodilator effect, ie, a favorable therapeutic index. AZD3199 was investigated as an inhaled, once-daily uLABA in patients with asthma and COPD. Preclinical studies have demonstrated AZD3199 to exhibit high selectivity and high potency as a β2-agonist in vitro, with a prolonged duration of action in vivo. This uLABA may have the potential to significantly improve the pharmacological treatment of these obstructive airway diseases. This paper presents the clinical pharmacokinetics and tolerability of AZD3199 in healthy volunteers and patients with asthma or COPD.
Materials and methods
Ethics
All studies were performed in accordance with the Declaration of Helsinki and the International Conference on Harmonisation/Good Clinical Practice and the AstraZeneca bioethics policy. All patients provided written informed consent prior to initiation of any study-specific procedures.
Healthy subjects and patients
Healthy volunteers were men aged 18–45 years, with a body mass index between 18 and 30 kg/m2. Volunteers were nonsmokers or ex-smokers who had stopped smoking >6 months prior to the study. In the Phase IIA study, asthmatic men or postmenopausal/surgically sterile females aged ≥18 years with a history of asthma for ≥6 months were recruited. Patients had a prebronchodilator forced expiratory volume in 1 second (FEV1) ≥60% of predicted normal and ≥1.5 L, and presented stepwise reversibility after inhalation of salbutamol. Systemic glucocorticoids within 30 days prior to the study constituted an exclusion criterion for the asthmatics.
COPD patients were men aged ≥40 years or women aged ≥40 years (effective contraceptive method or no childbearing potential for the last 3 months), with a clinical diagnosis of COPD and symptoms for ≥1 year. Patients were current or ex-smokers with a smoking history of ≥10 pack-years, a postbronchodilator FEV1 ≥40% and <80%, and FEV1/forced vital capacity <70%. History of asthma or atopic disease, a respiratory tract disorder other than COPD, or an exacerbation within 30 days constituted exclusion criteria for the COPD patients. Demographic details and number of eligible subjects given active drug or placebo are outlined in Table 1.
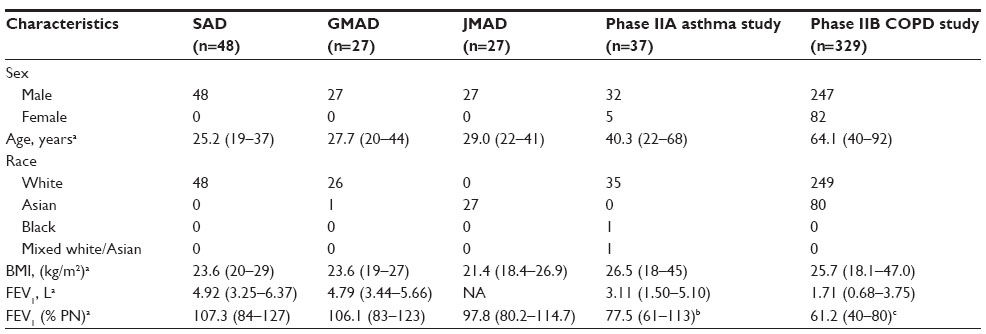 | Table 1 Patient demographic characteristics |
Administration modes and doses of AZD3199 by inhalation
The outcome of an adequately large range of doses is presented in order to assess basic clinical pharmacokinetic elements of inhaled AZD3199, particularly the extrapulmonary fate of AZD3199, and make possible exploration of the relation between systemic exposure and adverse class effects. The range of doses covered presumed clinically relevant regimens: single doses of AZD3199 480 μg have been shown effective in asthmatic patients, and repeat dosing of 200 μg once daily in COPD patients. A Spira nebulizer was used to administer single ascending doses (SADs) of AZD3199 in the SAD study, and a multidose dry-powder inhaler, Turbuhaler®, was used in the other four studies. The use of different inhalation devices had implications for the amount of drug reaching the lungs and ultimately the systemic circulation. The entire delivered dose of AZD3199 was assumed to reach the lungs after inhalation via nebulizer. The delivered dose via Turbuhaler was defined as the amount of AZD3199 leaving the orifice of the inhaler, of which approximately 40% has been estimated to reach the lungs, based on the analysis of fine particles generated in vitro using a computational model for extrathoracic deposition from dry powder inhalers.11 In order to harmonize the presentation of pharmacokinetic data in this paper, nebulized lung-deposited doses have been converted into Turbuhaler equivalents (nominal dose divided by 0.4). Treatments and study designs are summarized in Table 2.
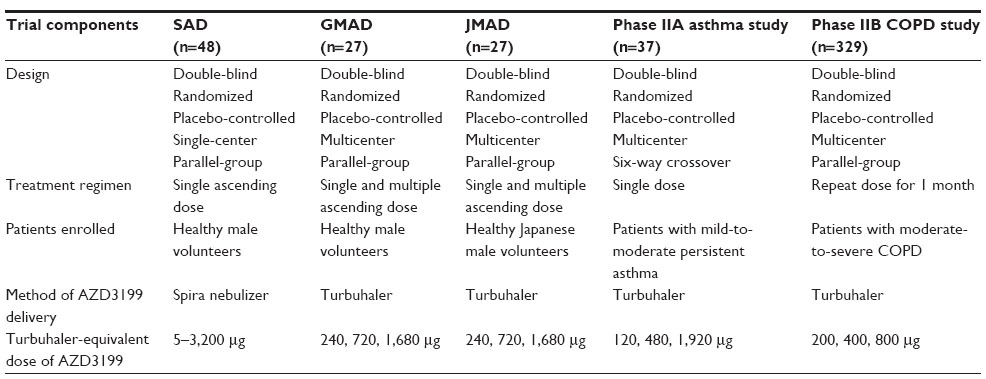 | Table 2 Treatments and study design |
Protocols for healthy subjects
Three Phase I studies were performed using a double-blind, randomized, and placebo-controlled design. SADs were studied on the basis of the outcome in six cohorts, each comprising six subjects on active treatment and two on placebo; Turbuhaler-equivalent delivered doses were 5, 25, 100, 400, 1,600, and 3,200 μg. Multiple ascending dosing (MAD) was studied separately in healthy Caucasian (global MAD [GMAD], NCT00713271) and Japanese (Japanese MAD [JMAD], NCT00772759) men. Both studies were subdivided into three cohorts, each comprising six subjects on active treatment and three on placebo; delivered doses via Turbuhaler were 240, 720, and 1,680 μg. Pharmacokinetics of AZD3199 were assessed using total plasma concentration and urinary excretion. Safety and tolerability were assessed by the incidence and nature of adverse events and clinically relevant abnormalities in laboratory variables after a single dose (SAD, GMAD, and JMAD) and after 12 days of once-daily dosing (GMAD and JMAD).
Protocols for patients
The primary objectives of the Phase IIA and Phase IIB studies were to investigate the pharmacodynamics and clinical efficacy of AZD3199, respectively, in comparison with formoterol and placebo. This paper reports the outcomes of pharmacokinetics, similarly assessed as in the healthy subjects.
The crossover Phase IIA study (NCT00736489) of asthmatic patients comprised six single-dose treatments: 120, 480 and 1,920 μg of AZD3199, 9 and 36 μg of formoterol (delivered doses via Turbuhaler), and placebo.11 The parallel-group Phase IIB study (NCT00929708) of COPD patients comprised five 4-week treatments: 200, 400, and 800 μg of AZD3199 delivered once daily via Turbuhaler, 9 μg of formoterol delivered twice daily via Turbuhaler, and placebo.12
Laboratory assessments
Serial measurements of plasma concentrations in healthy subjects were performed predose and at 5, 15, 30, and 60 minutes and 2, 4, 8, 12, 24, and 48 hours, and thereafter at 24-hour intervals up to 96 hours [4 days] after single dose in the SAD study and up to 384 hours [16 days] after the last [15th] dose in the GMAD; reduced schemes truncated at 24 hours postdose were applied in asthmatic and COPD patients. Urinary excretion of AZD3199 (sampled at 0–6, 6–12, 12–24, and 24–48 hours postdose) was determined in healthy subjects. Briefly, plasma and urine samples including AZD3199 plus (13C, 2H2, 15N)-AZD3199 as an internal standard were prepared using solid-phase ion exchange techniques. AZD3199 and the internal standard were separated from endogenous constituents using liquid chromatography and detected using mass spectrometry. The limit of quantification was 0.010 nmol/L in plasma and 0.250 nmol/L in urine. The bias (systematic error) and precision (between-assay variability) of the bioanalytical methods was <20% at the limit of quantification.
Tolerability was assessed overall on the basis of recorded adverse events and topically on the basis of FEV1. Additionally, serial measurements of serum potassium, plasma lactate, blood pressure, pulse, heart rate, QT interval corrected by Bazett’s formula (QTcB), tremor, and palpitations were used to assess systemic β2-adrenoceptor-mediated responses to inhaled AZD3199 in the asthmatic patients and healthy subjects. The magnitude of these potentially adverse effects was assessed only at trough concentration in COPD patients.
Data analysis
Pharmacokinetic parameters of AZD3199, terminal elimination half-life, apparent clearance (CL/F; only after administration via Turbuhaler), and mean residence time (MRT), were calculated using non-compartmental analysis techniques. Observed maximum plasma concentration (Cmax), time to reach Cmax (tmax), and area under the plasma–concentration time curve (AUC) are described by study, dose, and dosing (single or repeat) condition. Common values of terminal rate of elimination were used within studies to extrapolate AUC and AUMC (area under the first moment of the plasma concentration–time curve, calculated after single doses using the linear trapezoidal rule with extrapolation to infinite time, the latter portion being estimated as the last measurable concentration, multiplied by 1/λ ×[1/λ + tlast]) after Turbuhaler-equivalent doses of 100 μg and above (lack of measurable concentrations precluded extrapolation of data after lower doses). This approach was rationalized by visual comparison of plasma concentration–time curves across doses and pursued by analyzing slopes after the two top doses in the SAD study, the last repeat doses in the GMAD and JMAD studies, and by post hoc analysis of the asthma study using patients with data covering at least 5 days after dosing. The terminal rate of elimination could not be calculated in the study of COPD patients.
To assess the dose-dependency of Cmax and AUCs collected after single- and repeat-dose administration, power models (parameter = A x (dose)b, with A denoting a constant scale factor and b the exponent; b=1 indicates dose-proportionality) were fitted to individual parameter estimates using linear regression on log-log scales.
Representative mean plasma concentrations of AZD3199 from the GMAD study are presented by dose. When constructing plasma profiles across studies, data within each study were normalized to a 400 μg dose once linear pharmacokinetics were established and subsequently pooled across doses.
Average systemically β2-adrenoreceptor-mediated effect (Eav) was calculated as the AUC0–4h divided by the 4-hour time interval, and the observed peak effect as the minimum value, Emin (plasma potassium and diastolic blood pressure), or maximum value, Emax.
Data were summarized using descriptive statistics. Hypotheses were tested using two-sided alternative hypotheses as appropriate, with P-values less than 5% considered to be statistically significant.
Results
Pharmacokinetics
Inhaled AZD3199 was rapidly absorbed, showing maximum systemic concentration in the mean curve approximately 30 minutes following the SAD and MADs in healthy volunteers and asthma patients (Figure 1). The half-life of AZD3199 was long: the global geometric mean was estimated at 108 hours in the SAD study, 142 hours in the GMAD study, 140 hours in the asthma study, and 123 hours in the JMAD study. MRT was about 20% shorter than the half-life. The mean accumulation ratio after 12 days of once-daily dosing (days 3–14) – steady-state AUC (AUCss)/single-dose AUC (AUCsd)0–24h – was 2.28 in the GMAD and 1.83 in the JMAD study; the increase in plasma concentration was negligible at Cmax, but approximately eightfold at trough concentration because of the long terminal half-life. The geometric mean CL/F of AZD3199 after administration via Turbuhaler to healthy Caucasian subjects was estimated at 40.6 L/h after a single dose and 42.2 L/h during repeat dosing (less than 2% of renal origin).
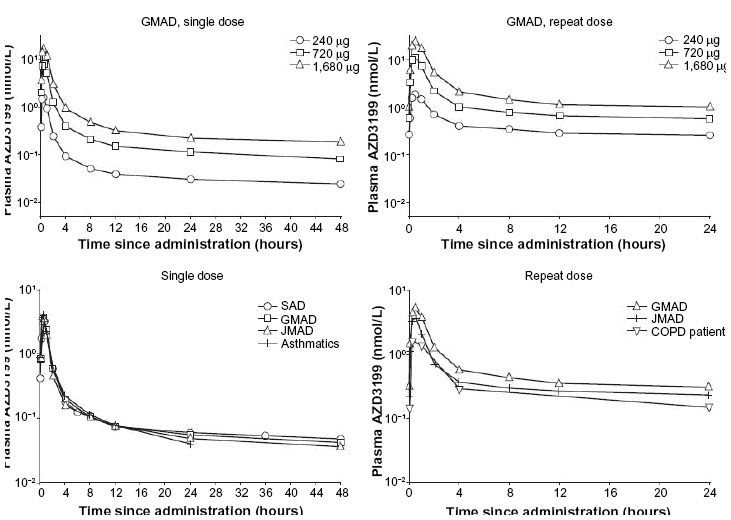 | Figure 1 Mean plasma concentration curves after single and repeat dose. Top row by dose in GMAD study. Bottom row shows average plasma profile from each study (scaled to represent a dose of 400 μg via Turbuhaler). |
Drug exposure, Cmax, and AUC of AZD3199, and tmax for subjects administered AZD3199 in each of the five studies are described in Table 3. The power-model index for the correlation between exposure and dose in the healthy Caucasian subjects was estimated at close to 1 (Figure 2), both with respect to Cmax (geometric mean 1.17 after single and 1.18 after repeat dose) and AUC (geometric mean 0.98 after single and 1.28 after repeat dose), suggesting dose-proportional pharmacokinetics of AZD3199. The time-linearity index – AUCss/AUCsd – was also estimated at about 1, both in Caucasian (geometric mean 0.928) and Japanese (geometric mean 0.830) healthy subjects, suggesting that the pharmacokinetics of AZD3199 are time-independent. The outcome in patients presented similarly dose-proportional pharmacokinetics of AZD3199. CL/F in healthy Japanese male subjects was about 40% higher, in asthma patients about 35% lower, and in COPD patients about double that in healthy Caucasian subjects. The resulting lower-than-expected magnitude of systemic AZD3199 exposure in COPD patients was positively noteworthy from a tolerability perspective, whereas differences vis-à-vis healthy Caucasian volunteers were clinically of minor importance with respect to the healthy Japanese men and patients with asthma (Figure 2). The study in the COPD patients demonstrated that there were no differences in exposure between men and women.
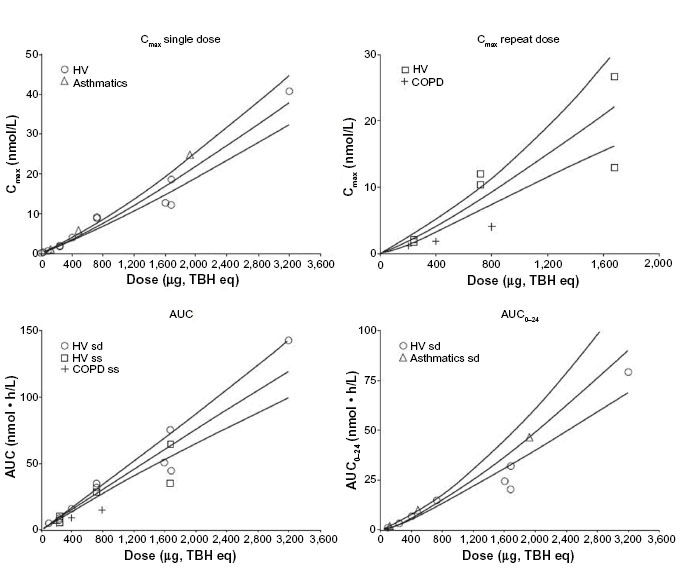 | Figure 2 Dose proportionality of AZD3199 Cmax and AUC, after single dose and after multiple doses. Fitted power models (based on healthy-volunteer data) with 95% confidence limits are superimposed. |
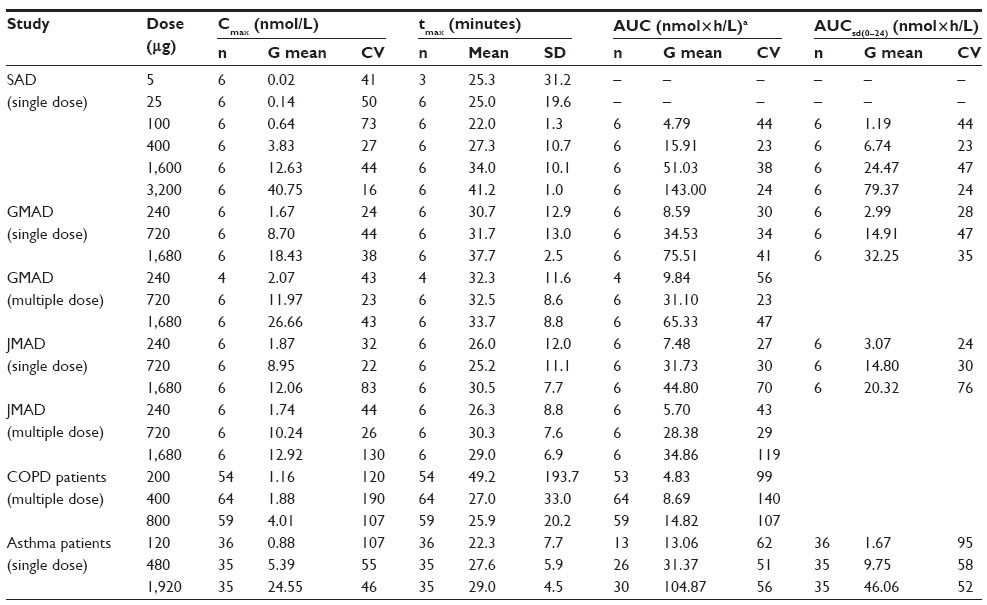 | Table 3 Summary of exposure, by study and dose level |
Tolerability and magnitude of effects
Overall, AZD3199 was well tolerated at both single and multiple dosing. No deaths, serious adverse events, discontinuations due to adverse events, or other significant adverse events were reported among healthy subjects or asthmatic patients. One death occurred in the COPD study, in a patient receiving placebo.12 Ten evenly distributed serious adverse events were recorded in COPD patients, of which two were considered to be causally related to the study medication: in both cases, formoterol. Furthermore, eleven COPD patients discontinued treatment due to adverse events (primarily exacerbation of COPD).
After single dosing, asthmatic patients spontaneously reported primarily headache and nasopharyngitis.12 The majority of adverse events during repeat once-daily dosing in COPD patients (95.3%) were considered to be of mild or moderate intensity; most frequently, nasopharyngitis, cough, COPD exacerbation, and throat irritation were reported.
Dose-dependent but mild systemically mediated class effects were observed in healthy volunteers (Table 4), and as previously presented, in patients with asthma11 and COPD,12 with small decreases in potassium levels and increases in heart rate and QTcB. AZD3199 demonstrated minimal or no effects on tremor and palpitation scores, lactate concentrations, and blood pressure in the studies where these parameters were assessed.
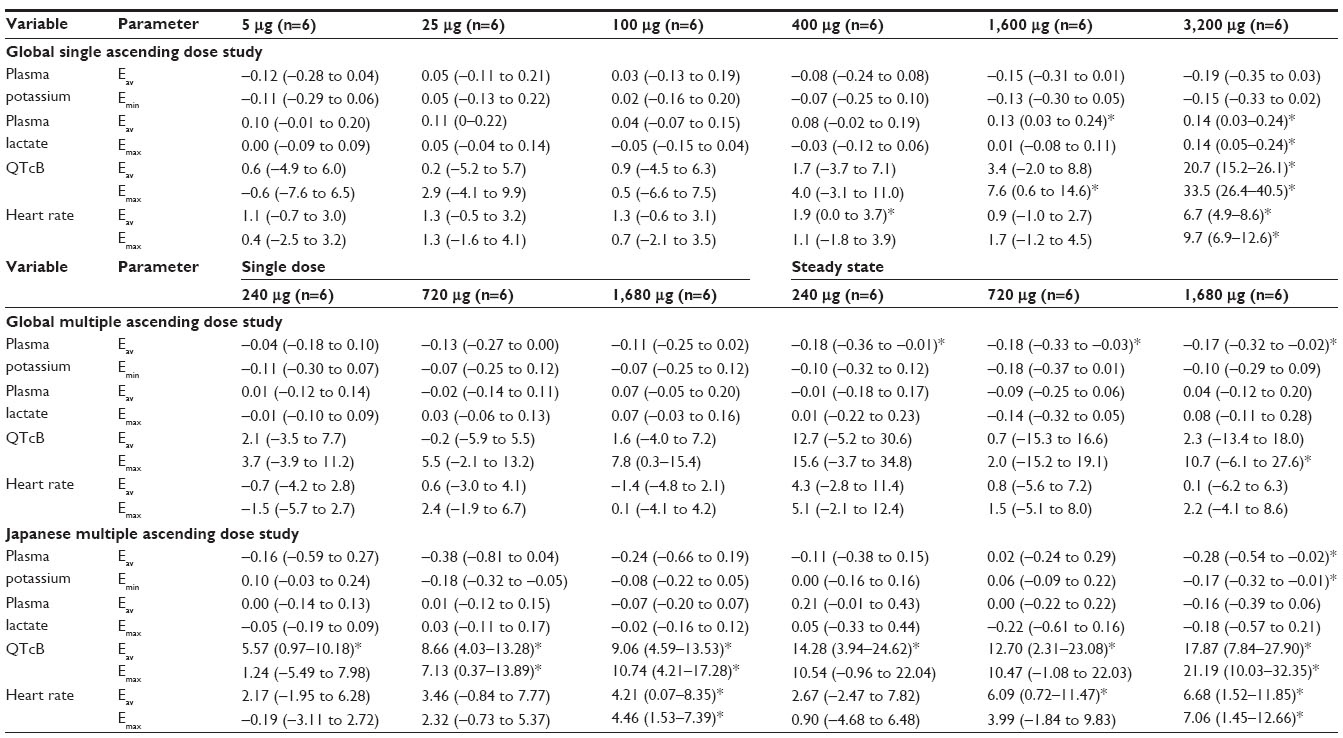 | Table 4 Summary of effects, expressed as mean difference vs placebo (95% confidence interval), on potassium, lactate, QTcB, and heart rate in healthy volunteers |
Discussion
This paper outlines the results of five clinical trials on AZD3199, a uLABA with the potential to be used in the treatment of asthma and COPD. Three studies in healthy volunteers assessed the safety and tolerability of AZD3199, monitoring for pharmacokinetic- and β2-adrenoreceptor-mediated adverse effects. Two further studies assessed the efficacy, safety, tolerability vis-à-vis formoterol, and pharmacokinetics of AZD3199 in patients with asthma or COPD (separately reported).
Concentration–time profiles for AZD3199 suggested a multicompartmental decline in plasma, reminiscent of that seen in the rat and the dog (AstraZeneca, data on file). A predefined upper limit of plasma exposure (AUC <111 nmol < h/L) was reached after a Turbuhaler-equivalent lung dose of 3,200 μg in healthy volunteers, and was consequently assigned the maximum dose that could be administered to patients. Inhaled AZD3199 adequately sustained bronchodilatation around the clock after a single inhaled dose of at least 480 μg in asthmatic patients and after at least 200 μg during repeat once-daily dosing in COPD patients.11,12 The outcome presented in this paper shows that these clinically relevant dose levels would elicit minimal systemically mediated cardiovascular and metabolic class effects. Pharmacokinetic data demonstrated fast initial absorption and a mean elimination half-life of up to 142 hours. Further pharmacokinetic studies would be required to determine whether the long half-life of AZD3199 could be related to slow systemic elimination or an elimination rate limited by slow pulmonary terminal absorption and/or lung retention.
Overall, plasma exposure of AZD3199 was compatible with linear kinetics. Similar exposure after a single dose (AUC extrapolated to infinity) and during a dosage interval at repeat dosing (AUC0–24h after 12 days of once-daily dosing) in the MAD studies suggested time linearity. The accumulation index based on plasma AUC was approximately 2. The trough concentration of AZD3199 increased eightfold during once-daily administration, an expected consequence of a slow terminal rate of elimination. However, importantly for potentially adverse systemically driven class effects, the Cmax of inhaled AZD3199 increased only marginally during repeat dosing once daily; no call for dose adjustment during regular treatment. Shorter MRT than terminal half-life can be explained by the fact that a significant fraction of AZD3199 is distributed into extravascular compartments, and that redistribution to plasma limits the overall rate of elimination.13
Despite differences in how the nominal dose of AZD3199 was defined after inhalation via the nebulizer and the dry-powder Turbuhaler inhaler, the systemic fate of AZD3199 was presumably similar irrespective of the mode of administration. The plasma levels recorded in the studies presented in this paper supported the hypothesized relation between devices with respect to overall rate and extent of drug reaching the lungs and ultimately the systemic circulation.
There were minor differences in the systemic exposure of AZD3199 in healthy Japanese volunteers and patients with asthma, compared with that in healthy Caucasian male volunteers. Importantly, from a clinical tolerability perspective, the observed relatively higher exposure in asthmatics was still not high enough to be clearly expressed as more pronounced systemically mediated adverse effects. However, the evaluation of AZD3199 pharmacokinetics after 1 month of once-daily dosing in patients with COPD indicated dose proportionality; the systemic exposure to AZD3199 was approximately half that seen in healthy volunteers after multiple dosing and in asthmatic patients with a moderately reduced FEV1 after single dosing. Similar results have been observed with formoterol inhaled via Turbuhaler, with systemic exposure in patients with COPD tending to be lower compared with healthy volunteers (AstraZeneca, data on file). Previous studies have also demonstrated systemic exposure of inhaled budesonide and fluticasone in patients with moderate-to-severe COPD to be approximately half that observed in healthy volunteers.14 For budesonide, this difference was not apparent when comparing patients with mild asthma with healthy volunteers, in line with the present study.15 The lower systemic exposure of AZD3199 in COPD patients could imply that relatively less inhaled AZD3199 reached the lungs in these patients compared with patients with asthma or healthy volunteers. However, differences in pulmonary absorption may complicate such a comparison, since systemic exposure is only an indirect measure of lung deposition. In fact, the results show that a clinically relevant effect was achieved in COPD patients at doses similar to those shown to be effective in an asthma population.
The five studies demonstrated that inhaled AZD3199 was well tolerated, had a good safety profile, and was not associated with consistent or clinically relevant systemic adverse effects in healthy volunteers or patients with asthma or COPD. Marginal but dose-dependent effects were observed on plasma potassium, pulse, heart rate, and QTcB in the first 4 hours postdose in comparison with placebo. No, or minimal, effects of AZD3199 were observed on parameters that are commonly affected by β2-adrenoreceptor agonists, including tremor and palpitation scores, lactate concentrations, or blood pressure.
Conclusion
In conclusion, AZD3199 plasma exposure suggested linear pharmacokinetics and a long half-life. Systemic availability was similar in healthy subjects and patients with asthma, but was lower in patients with COPD. AZD3199 showed no, or at-most mild, systemic effects. These clinical trials suggest that AZD3199 is well tolerated in healthy male volunteers and patients with asthma or COPD, and no safety concerns were identified to preclude further development of the drug as a uLABA.
Acknowledgments
All studies reported here were funded by AstraZeneca. The authors thank David Candlish and Natasha Hausman of in- Science Communications, Springer Healthcare, for medical writing assistance funded by AstraZeneca.
Author contributions
All authors contributed toward drafting and revising the paper and agree to be accountable for all aspects of the work. LB was involved as the principal investigator in the phase I (healthy volunteer) and phase IIa (asthma) studies; PK was involved as the principal investigator in the phase IIb (COPD) study; CJ is the AstraZeneca physician responsible for the AZD3199 studies; TB was the AstraZeneca statistician responsible for the AZD3199 studies; JR was the AstraZeneca pharmacokineticist responsible for the AZD3199 studies.
Disclosure
LB has during the last 3 years received honoraria for attending advisory board meetings or giving lectures for the following companies: Almirall, AstraZeneca, Airsonette, Andre Pharma-Chiesi, Boehringer, GlaxoSmithKline, Meda, Merck, Mundipharma, Nigaard Pharma, Novartis, Pfizer, Takeda/Nycomed, and Teva. PK has received consulting fees from Almirall, Boehringer Ingelheim, AstraZeneca, GSK, Novartis, Chiesi, and MSD, has been reimbursed for travel to medical conferences by Boehringer Ingelheim, Novartis, AstraZeneca, Chiesi, Allergopharma, Almirall, and FAES, and has received fees for speaking from Adamed, Allergopharma, AstraZeneca, Boehringer Ingelheim, GSK, Krka, MSD, Novartis, Pfizer, Stallergen, Leva, Polpharma, FAES, and Chiesi. CJ is an employee of AstraZeneca, and holds shares in the company. TB and JR were employees of AstraZeneca at the time these studies were conducted and analyzed.
References
Löfdahl CG, Svedmyr N. Formoterol fumarate, a new beta 2-adrenoceptor agonist. Acute studies of selectivity and duration of effect after inhaled and oral administration. Allergy. 1989;44:264–271. | |
Global initiative for chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Bethesda (MD):GOLD; 2011. Available from: http://www.goldcopd.org/uploads/users/files/GOLDReport_April112011.pdf. Accessed August 1, 2014. | |
Hochhaus G, Möllmann H, Darendorf H, Gonzalez-Rothi R. Pharmacokinetic/pharmacodynamic aspects of aerosol therapy using glucocorticoids as model. J Clin Pharmacol. 1997;37:881–892. | |
Edsbäcker S, Jendbro M. Modes to achieve topical selectivity of inhaled glucocorticoids – focus on budesonide. Respir Drug Delivery. 1998;6:71–82. | |
Rosenborg J, Larsson P, Rott Z, Böcskei C, Poczi M, Juhász G. Relative therapeutic index between inhaled formoterol and salbutamol in asthma patients. Respir Med. 2002;94:412–417. | |
Malolepszy J, Böszörményi Nagy G, Selroos O, Larsso P, Brander R. Safety of formoterol Turbuhaler at cumulative dose of 90 μg in patients with acute bronchial obstruction. Eur Respir J. 2001;18:928–934. | |
Anderson GP, Linden A, Rabe KF. Why are long-acting beta-adrenoceptor agonists long-acting? Eur Respir J. 1994;7:569–578. | |
Masoli M, Weatherall M, Ayling J, Williams M, Beasley R. The 24 h duration of bronchodilator action of the salmeterol/fluticasone combination inhaler. Respir Med. 2005;99:545–552. | |
Masoli M, Williams M, Weatherall M, Beasley R. The 24 h duration of bronchodilator action of the budesonide/formoterol combination inhaler. Respir Med. 2006;100:20–25. | |
Beeh KM, Derom E, Kanniess F, Cameron R, Higgins M, van As A. Indacaterol, a novel inhaled β2-agonist, provides sustained 24-h bronchodilation in asthma. Eur Respir J. 2007;29:871–878. | |
Bjermer L, Rosenborg J, Bengtsson T, Lötvall J. Comparison of the bronchodilator and systemic effects of AZD3199, an inhaled ultra-long-acting β2-adrenoceptor agonist, with formoterol in patients with asthma. Ther Adv Respir Dis. 2013;7:264–271. | |
Kuna P, Ivanov Y, Trofimov VI, et al. Efficacy and safety of AZD3199 vs formoterol in COPD: a randomized, double-blind study. Respir Res. 2013;14:64. | |
Riegelman S, Collier P. The application of statistical moment theory to the evaluation of in vivo dissolution time and absorption time. J Pharmacokinet Biopharm. 1980;8:509–534. | |
Dalby C, Polanowski T, Larsson T, Borgström L, Edsbäcker S, Harrison TW. The bioavailability and airway clearance of the steroid component of budesonide/formoterol and salmeterol/fluticasone after inhaled administration in patients with COPD and healthy subjects: a randomized controlled trial. Respir Res. 2009;10:104. | |
Edsbäcker S, Wollmer P, Selroos O, Borgström L, Olsson B, Ingelf J. Do airway clearance mechanisms influence the local and systemic effects of inhaled corticosteroids? Pulm Pharmacol Ther. 2008;21:247–258. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.