")
Back to Journals » Clinical Interventions in Aging » Volume 10
Characteristics of abdominal cavity drainage fluid in Chinese patients without postoperative complications after surgery for gastrointestinal or retroperitoneal tumors
Received 28 October 2014
Accepted for publication 3 December 2014
Published 28 January 2015 Volume 2015:10 Pages 367—370
DOI https://doi.org/10.2147/CIA.S76512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Jing Zhou,1 Hongying Pi,2 Yingying Zheng1
1General Surgery, 2Nursing Department, Chinese People’s Liberation Army General Hospital, Beijing, People’s Republic of China
Background: Abdominal cavity drainage fluid can be used as an early diagnostic tool of postoperative complications, and observing its characteristics can help us to judge and handle postoperative complications. There is no accurate standard reference range on its characteristics after surgeries for gastrointestinal or retroperitoneal tumors. This research attempted to analyze its characteristics in Chinese patients without postoperative complications after surgery for gastrointestinal or retroperitoneal tumors, and to offer an experimental basis for establishing a reliable standard reference range for abdominal cavity drainage fluid used to detect postoperative complications.
Methods: This study enrolled 262 Chinese patients without postoperative complications after surgery for gastrointestinal or retroperitoneal tumors.
Results: All patients had a median age (range) of 55 (19–72) years, and 150 (57.3%) were men. There were 93 (35.5%), 115 (43.9%), and 54 (20.6%) patients who underwent surgery for upper gastrointestinal tumors, lower gastrointestinal tumors, and retroperitoneal tumors, respectively. The total amount, density, and pH of the abdominal cavity drainage fluid were 204 (0–6,195) mL, 1.032 (1.011–1.047) kg/m3, and pH 7.0 (5.0–7.5), respectively. The total numbers of cells and white blood cells were 1.3×1011 (5.5×108–6.2×1012)/L and 3.7×109 (1.0×107–5.0×1011)/L, respectively. The levels of sugar and protein were 3 (0–37) mmol/L and 39 (1–272) g/L. The total amount of abdominal cavity drainage fluid, the total number of cells, the total number of white blood cells, the number of multinucleated cells, the number of monocytes, and the levels of sugar were statistically significantly different between the three groups (P<0.05 for all).
Conclusion: This study described the characteristics of abdominal cavity drainage fluid in Chinese patients without postoperative complications after surgery for gastrointestinal or retroperitoneal tumors, and provided an experimental basis for establishing a reliable standard reference range for abdominal cavity drainage fluid for screening for postoperative complications.
Keywords: abdominal cavity drainage fluid, People’s Republic of China, gastrointestinal tumors, postoperative complications, retroperitoneal tumors
Introduction
Normal abdominal cavity fluid of adults is less than 50 mL, mainly playing the role of lubrication in the cavities and is generally not easily collected. A large amount of abdominal cavity fluid is accumulated after surgery for gastrointestinal or retroperitoneal tumors, and it is standard practice to place a drainage tube in the abdomen to drain the residual hemorrhage, effusion, chylous fluid, pancreatic juice, and intestinal fluid.1–6 Surgery for gastrointestinal or retroperitoneal tumors is a common and complex kind of general surgical operations, and its common postoperative complications are bleeding, biliary fistula, pancreatic fistula, chyle fistula, intestinal fistula, and abdominal cavity infection.7,8 Drainage insertion is an effective method of managing possible leakage, providing evidence of leakage or postoperative hemorrhaging, or preventing postoperative infection by discharging blood and avoiding the formation of abdominal abscesses.9,10 Data of abdominal cavity fluid are a predictive marker for future postoperative complications. Abdominal cavity drainage fluid can be used as an early diagnostic tool of postoperative complications, and observing the characteristics of abdominal cavity drainage fluid can help us to judge and handle any postoperative complications as soon as possible.1 There is still no accurate standard reference range for the characteristics of abdominal cavity drainage fluid after surgery for gastrointestinal or retroperitoneal tumors, and thus clinical laboratories can only borrow the reference range of serous cavity effusion. Therefore, the current research attempted to analyze the characteristics of abdominal cavity drainage fluid in Chinese patients without postoperative complications after surgery for gastrointestinal or retroperitoneal tumors, and offer an experimental basis for establishing a reliable standard reference range for abdominal cavity drainage fluid used to detect any postoperative complications.
Methods
Study participants
From June 2012 to July 2013, 262 patients were diagnosed with gastrointestinal or retroperitoneal tumors at the General Surgery of Chinese People’s Liberation Army General Hospital and enrolled in the current study. All of these patients had no bleeding, biliary fistula, pancreatic fistula, chyle fistula, intestinal fistula, or abdominal cavity infection, and smoothly discharged from the hospital. According to preoperative computed tomography, magnetic resonance imaging, and postoperative pathology, patients with the following were excluded: those without a tumor tissue source of gastrointestinal or retroperitoneal tumors, such as lymphatic hematopoietic or urogenital tumors, and those with tumors of a wide range and preoperative ascitic fluid. Study patients were divided into groups according to the type of tumors: upper gastrointestinal tumors, lower gastrointestinal tumors, and retroperitoneal tumors. The study protocol was approved by the Ethics Committee of the Chinese People’s Liberation Army General Hospital (Beijing, People’s Republic of China) and in accordance with the Helsinki Declaration of 1975 (as revised in 1983). Each participant provided written informed consent to be included in the study.
Data collection
From the first postoperative day, abdominal cavity drainage fluid was collected in the morning until the liquid drainage tube was pulled up, and then the total amount of abdominal cavity drainage fluid was measured. Meanwhile, the color and transparency of the fluid were recorded. The drainage fluid specimens were sent to the clinical laboratory of the Chinese People’s Liberation Army General Hospital, and then the density, pH, the total number of cells, the total number of white blood cells, the number of multinucleated cells, the number of monocytes, and the levels of sugar, protein, and chloride were measured.
Statistical analysis
Categorical variables were reported as number with percentage, normally distributed continuous variables as mean with standard deviation, and non-normally distributed continuous variables as median with interquartile range. Differences between the groups were analyzed using the chi-square test for categorical variables, independent t-test for normally distributed continuous variables and Mann–Whitney test for non-normally distributed continuous variables. All statistical tests were two-sided, with P<0.05 as the level of significance. Statistical analyses were performed using SPSS software (v17; IBM Corporation, Armonk, NY, USA).
Results
For all patients, there was a median age (range) of 55 (19–72) years, and 150 (57.3%) were men. There were 93 (35.5%), 115 (43.9%), and 54 (20.6%) patients who underwent surgery for upper gastrointestinal tumors, lower gastrointestinal tumors, and retroperitoneal tumors, respectively. The total amount, density, and pH of the abdominal cavity drainage fluid were 204 (0–6,195) mL, 1.032 (1.011–1.047) kg/m3, and pH 7.0 (5.0–7.5), respectively. The total numbers of cells and white blood cells were 1.3×1011 (5.5 ×108–6.2×1012)/L and 3.7×109 (1.0 ×107–5.0×1011)/L, respectively. The levels of sugar and protein were 3 (0–37) mmol/L and 39 (1–272) g/L. The mean characteristics of the abdominal cavity drainage fluid are shown in Table 1. The total amount of abdominal cavity drainage fluid, the total number of cells, the total number of white blood cells, the number of multinucleated cells, the number of monocytes, and the levels of sugar were statistically significantly different between the three groups (P<0.05 for all). The color, transparency, density, pH, and the levels of protein and chloride were similar between the three groups (P>0.05 for all).
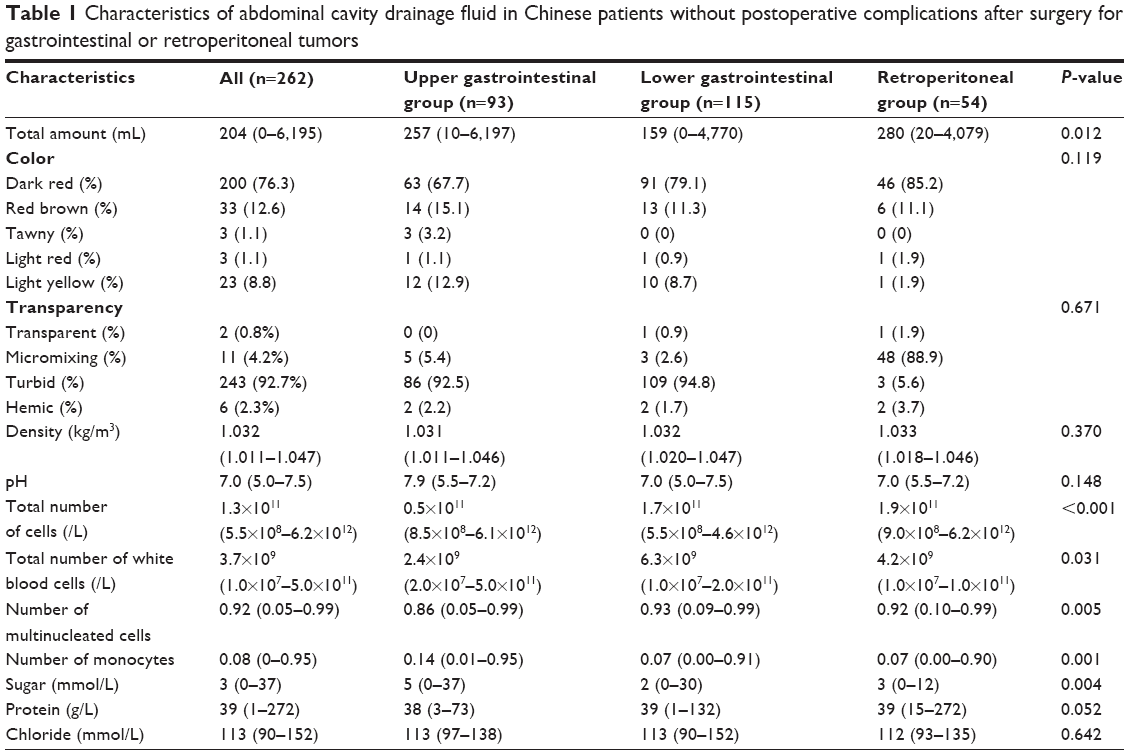 | Table 1 Characteristics of abdominal cavity drainage fluid in Chinese patients without postoperative complications after surgery for gastrointestinal or retroperitoneal tumors |
Discussion
For several decades, the routine use of postoperative abdominal drainage has been standard practice in abdominal surgery.1–6 Most surgeons insert routine drainage following abdominal surgeries. The early identification and monitoring of fluid collection in the abdomen, the detection of postoperative bleeding or anastomotic leakage, and the prevention of their negative impact on the patient’s recovery can be accomplished by postoperative abdominal drainage.9,10 Due to the lack of a standard reference range for the characteristics of abdominal cavity drainage fluid after surgery for gastrointestinal or retroperitoneal tumors, clinical laboratories have no choice but to use the reference range for serous cavity effusion as an alternative standard. The present study is the first Chinese study to examine the color and characteristics of abdominal cavity drainage fluid in patients without postoperative complications after surgery for gastrointestinal or retroperitoneal tumors. The information of abdominal cavity drainage fluid could pave the way for the establishment of a standard reference range for abdominal cavity drainage fluid, outside of which could prompt the emergence and development of postoperative complications, and thus help with the prompt diagnosis and control of postoperative complications.
The current study showed that a great number of cells and white blood cells were present in the abdominal cavity drainage fluid of patients without postoperative complications, and demonstrated that a certain amount of cells and white blood cells are not an indicator of infection. Postoperative stress, ischemia reperfusion, and tissue repair can lead to aseptic inflammation as well as the increase of cells and white blood cells in the abdominal cavity drainage fluid. After surgery for upper gastrointestinal tumors, lower gastrointestinal tumors, or retroperitoneal tumors, there was a difference in the total numbers of cells and white blood cells in the abdominal cavity drainage fluid, which could be caused by the distinction of peritoneal distribution and lymphatic drainage.11–14
The results from the present study suggested that abdominal cavity drainage fluid had a certain amount of protein. Surgery for gastrointestinal or retroperitoneal tumors have a large wound surface area, a widely cleaning of lymph nodes, and a severe cutting off of blood capillaries and lymphatic vessels, all of which can lead to the transfer of protein from tissue fluid into the abdominal cavity drainage fluid. Quek et al observed that even if adding protein, some patients still had the levels of serum protein fallen.15 Loss of protein through abdominal cavity drainage fluid should be specially considered in these patients and it is very important to supply the protein in time according to the total amount of abdominal cavity drainage fluid.
Conclusion
In conclusion, the current study described the characteristics of abdominal cavity drainage fluid in patients without postoperative complications after surgery for gastrointestinal or retroperitoneal tumors, and provided an experimental basis for establishing a reliable standard reference range for abdominal cavity drainage fluid used to screen for postoperative complications.
Acknowledgment
We are grateful to all the patients for their participation in the study. This study was supported by the Key Nursery Fund of the Chinese People’s Liberation Army General Hospital technical innovation (13KMZ04) and the Medical Scientific Research Fund of the Hainan Provincial Health Department.
Disclosure
The authors report no conflicts of interest in this work.
References
van der Wilt AA, Coolsen MM, de Hingh IH, et al. To drain or not to drain: a cumulative meta-analysis of the use of routine abdominal drains after pancreatic resection. HPB (Oxford). 2013;15(5):337–344. | ||
Puleo FJ, Mishra N, Hall JF. Use of intra-abdominal drains. Clin Colon Rectal Surg. 2013;26(3):174–177. | ||
Petrowsky H, Demartines N, Rousson V, Clavien PA. Evidence-based value of prophylactic drainage in gastrointestinal surgery: a systematic review and meta-analyses. Ann Surg. 2004;240(6):1074–1084; discussion 1084–1085. | ||
Giovinazzo F, Butturini G, Salvia R, et al. Drain management after pancreatic resection: state of the art. J Hepatobiliary Pancreat Sci. 2011;18(6):779–784. | ||
Niola R, D’Agostino H, Hoyt A, et al. [A comparative multicenter study of the efficacy of single- and double-lumen catheter drainage]. Radiol Med. 1996;91(1–2):107–110. Italian. | ||
Broomé AE, Hansson LC, Tyger JF. Efficiency of various types drainage of the peritoneal cavity – an experimental study in man. Acta Chir Scand. 1983;149(1):53–55. | ||
Gupta R, Sample C, Bamehriz F, Birch DW. Infectious complications following laparoscopic appendectomy. Can J Surg. 2006;49(6):397–400. | ||
Kobayashi M, Okabayashi T, Namikawa T, Okamoto K, Araki K. Management of intra-abdominal abscess due to surgical site infection. Surg Technol Int. 2006;15:37–39. | ||
Shrikhande SV, Barreto SG, Shetty G, et al. Post-operative abdominal drainage following major upper gastrointestinal surgery: single drain versus two drains. J Cancer Res Ther. 2013;9(2):267–271. | ||
Iwata N, Kodera Y, Eguchi T, et al. Amylase concentration of the drainage fluid as a risk factor for intra-abdominal abscess following gastrectomy for gastric cancer. World J Surg. 2010;34(7):1534–1539. | ||
Azzali G. The lymphatic vessels and the so-called “lymphatic stomata” of the diaphragm: a morphologic ultrastructural and three-dimensional study. Microvasc Res. 1999;57(1):30–43. | ||
Cheynel N, Valleix D, Durand-Fontanier S, Mabit C, Descottes B. [Role of the lymphatics of the diaphragm in the absorption of intraperitoneal liquids]. Morphologie. 2001;85(268):13–15. French. | ||
Castenholz A, Hauck G, Rettberg U. Light and electron microscopy of the structural organization of the tissue-lymphatic fluid drainage system in the mesentery: an experimental study. Lymphology. 1991;24(2):82–92. | ||
Hollender LF, Meyer C, Calderoli H, Alexiou D. [Peritoneum: anatomy applied to abdominal drainage]. Morphol Med. 1981;1(1):9–14. French. | ||
Quek ML, Stein JP, Clark PE, et al. Microscopic and gross extravesical extension in pathological staging of bladder cancer. J Urol. 2004;171(2 Pt 1):640–645. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.