")
Back to Journals » Clinical Interventions in Aging » Volume 9
Changes in spinal range of motion after a flexibility training program in elderly women
Authors Battaglia G , Bellafiore M, Carmazza G, Paoli A, Bianco A, Palma A
Received 21 December 2013
Accepted for publication 11 February 2014
Published 11 April 2014 Volume 2014:9 Pages 653—660
DOI https://doi.org/10.2147/CIA.S59548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Giuseppe Battaglia,1,2 Marianna Bellafiore,1,2 Giovanni Caramazza,2 Antonio Paoli,3 Antonino Bianco,1,2 Antonio Palma1,2
1Department of Law, Society, and Sport Sciences, University of Palermo, Palermo, Italy; 2Sicilian Regional Sports School of Italian National Olympic Committee (CONI), Sicily, Italy; 3Department of Biomedical Sciences, University of Padova, Padova, Italy
Background: Aging-related reduced spinal mobility can interfere with the execution of important functional skills and activities in elderly women. Although several studies have shown positive outcomes in response to spinal flexibility training programs, little is known about the management of sets and repetitions in training protocols. The purpose of this study was to investigate the effects of an 8-week specific and standardized flexibility training program on the range of spinal motion in elderly women.
Methods: Participants were recruited in a senior center of Palermo and randomly assigned in two groups: trained group (TG) and control group (CG), which included 19 and 18 women, respectively. TG was trained for 8 weeks at two sessions/week. In particular, every session included three phases: warm up (~10 minutes), central period (~50 minutes), and cool down (~10 minutes). CG did not perform any physical activity during the experimental period. Spinal ranges of motion (ROM) were measured from neutral standing position to maximum bending position and from neutral standing position to maximum extension position before and after the experimental period, using a SpinalMouse® device (Idiag, Volkerswill, Switzerland).
Results: After the training period, TG showed an increase in spinal inclination by 16.4% (P<0.05), in sacral/hip ROM by 29.2% (P<0.05), and in thoracic ROM by 22.5% (P>0.05) compared with CG from maximum extension position to maximum bending position. We did not observe any significant difference in TG's lumbar ROM compared with CG after the training period (P>0.05).
Conclusion: We found that an 8-week flexibility training program improved ROMs of the spine in elderly women. The training protocol appeared to be practicable for active elderly people with autonomy and the capability for self-care.
Keywords: exercise, ROM, spinal mouse, elderly, physical activity, stretching
Introduction
It is known that physical activity gradually reduces in elderly people1 and that a sedentary lifestyle represents a risk factor for decline in quality of life (QOL).2 In particular, the typical adaptive shortening of soft tissue and the partial loss of range of spinal motion that characterize the aging-related spinal dysfunction syndrome are mainly a result of a poor practice of exercise in older subjects.3,4 Elderly people generally assume the sitting position for a longer period of time,5 maintaining prolonged lumbar flexion. Several studies have demonstrated that exercise programs can improve body balance,6,7 bodyweight distribution on the feet,8 muscle strength, flexibility,9 and QOL10 in the elderly.
Imagama et al reported that a training program including muscle strength and spinal range of motion (ROM) might be able to affect positively primary factors related to QOL, such as lumbar lordosis angle, sagittal balance, spinal ROM, and back muscle strength in middle-aged and elderly subjects.11 Figueira et al showed that a governmental physical activity program improved several QOL-related factors such as sensorial functioning, social participation, perceptions of death and dying, and intimacy in Brazilian elderly people.10 In addition, flexibility is a central key in the daily functional health status of elderly people.
Suitable levels of joint flexibility are known to be fundamental in maintaining a high level of functional independence and performance in elderly subjects in several daily activities,12 such as dressing and bathing. Although joint flexibility may decline with age, elderly subjects could maintain and/or improve it through core stability, stretching, and articular mobility exercises. Gajdosik et al showed improvements in maximal length, extensibility, and passive resistive forces of elders’ calf muscles in response to an 8-week stretching program.13 Reid and McNair found that elderly people with and without arthritis of the knee were able to show sustained improvements in joint range of motion with stretching interventions.14 Moreover, Rider and Daly indicated a significant improvement in spinal mobility in trained elderly subjects after a series of flexibility exercises for a total of 10 weeks.15 In the light of the positive effects of exercise in elderly people, it is important to increase evidence-based recommendations for elderly adult exercise programs. Indeed, in agreement with the 2009 American College of Sports Medicine position statement, there are few studies on the potential benefits of flexibility-specific training interventions on ROM of elders’ spines, and there also is a lack of consensus concerning the prescription of stretching exercises for elderly people.16 Moreover, little is known about the management of workload parameters, such as the type of exercises and the number of sets and repetitions that should be used in training protocols to improve the health of the spine in the elderly.
The purpose of the current study was to investigate the changes in spinal ROM after an 8-week flexibility training program in elderly women, modulating the volume (sets and repetitions) of workload training. In this way, our study might increase knowledge about the training methodology to adopt in geriatric gymnastics to improve the flexibility and functionality of aging spines of elder patients. Indeed, we speculated that our training protocol, including several combined exercises for core stability and spine flexibility, might oppose the aging-related ROM reduction of the spine.
Materials and methods
Participants
Participants were Italian volunteers who attended the project named “Volare”, supported by local government, in 2012. This project was carried out in a senior center in Palermo, Sicily, Italy, in the first half of the year. All subjects were administered a questionnaire about health status, personal data, time dedicated to physical activity, history of falls in the last year, and autonomy and capability in self-care and normal household tasks. Subjects were eligible for the study if they met all of the following inclusion criteria: 60 or more years of chronological age, capacity to provide informed consent for study participation, a medical certificate attesting to their cognitive and physical suitability to participate in an experimental study including the practice of physical activity, at least 6 months of a programmed physical activity to recruit active elderly people, the availability to attend at least 80% of the training period, declared autonomy, stated capability in self-care and normal household tasks, and no falls in the last year.
Participants were excluded from the study if they had severe walking or standing disabilities4 or a high risk of falling and a score of 45 or less on the Berg balance scale.17
Forty-five subjects, including 41 women and 4 men, were accepted to the project, but only women were recruited. After starting the interview and screening, only 37 women were considered suitable for our study because the others did not meet all inclusion criteria. Participants were randomly assigned into one of two groups using a random numbers table: the trained group (TG) and a control group (CG), which included 19 and 18 women, respectively. The TG was trained for 8 weeks by two mesocycles of 4 weeks each, including two training sessions/week; the CG did not perform any organized physical activity during the experimental period in this double-blinded study. The examiner could not distinguish trained subjects from controls because he was not involved in the random assignment process or the training sessions. All tests were performed in the morning, three times, and the average value was provided for statistical analysis. The same investigator took all the measurements.
Before starting the study, an appropriate local ethics committee approval (Commissione Etica del Dipartimento DISMOT) and written informed consent from each participant were obtained. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Anthropometric measurements
Anthropometric measurements were assessed according to standardized procedures recommended at the Airlie Conference.18 In particular, body weight was measured using a Seca electronic scale (maximum weight recordable, 300 kg; resolution, 100 g; Seca, Hamburg, Germany), with the subjects wearing only underwear. Height was measured using a standard stadiometer (maximum height recordable, 220 cm; resolution, 1 mm), with the subjects barefoot and standing upright. Body mass index was calculated as body weight divided by height squared (kg·m−2).
Berg balance scale assessment
The Berg scale was used to measure balance during functional activities, using 14 items. These tasks were classified from 0 to 4, with 0 being the worst and 4 the best performance. The calculation of these points could reach a maximum of 56 points; the fewer points, the larger the risk to subjects’ balance. This scale had a cut point for the risk of falls: individuals with values lower than 45 present a high risk of falling.17
Measurement of spinal range of motion
Spinal ROM was evaluated by SpinalMouse®(Idiag, Volkerswill, Switzerland), an electronic, computer-aided measuring device that evaluates sagittal ROM of the spine and intersegmental angles in a noninvasive technique.19 The SpinalMouse was run paravertebrally along the spine from the seventh cervical (C7) to the third sacral (S3) vertebra. We measured each angle in a neutral standing position (NSP), maximum extension position (MEP), and maximum flexion position to evaluate thoracic, lumbar, and total spinal ROM. Participants were asked to try to touch their toes with their fingers, with the neck slightly flexed, their knees straight, and their feet about 30 cm apart. For extension, elderly women were invited to extend their back as far as possible without external help. All assessments were performed three times, but only the average value was provided for statistical analysis. The same investigator took all the measurements, and kyphotic angles were expressed as positive values, whereas lordotic angles were expressed as negative values. No warming up was performed before the assessment. We found intraclass coefficients of 0.90–0.94 for ROM measurements.
Exercise training protocol
The flexibility training program was performed for 8 weeks by two mesocycles of 4 weeks each, including two training sessions/week. Every session included three main phases, in agreement with a previous study20: warm-up (~10 minutes), central period (~50 minutes), and cool down (~10 minutes). In the warm-up phase, from a standing posture, participants executed a standard sequence of exercises (Table 1). In the central period phase, subjects performed twice a specific flexibility training mesocycle with a sinusoidal pattern of workload (sets and repetitions of exercises) during the training period (Table 1). In particular, the workload volume and intensity was augmented from the first to the third week and from the fifth to the seventh week, increasing the complexity and number of sets and repetitions by several exercises (see Table 2 for description of exercises). During the fourth and eighth weeks, the workload was reduced, decreasing the complexity and number of sets and repetitions by several exercises (Tables 1 and 2). The cool-down phase included a standard sequence of stretching exercises (Table 1).
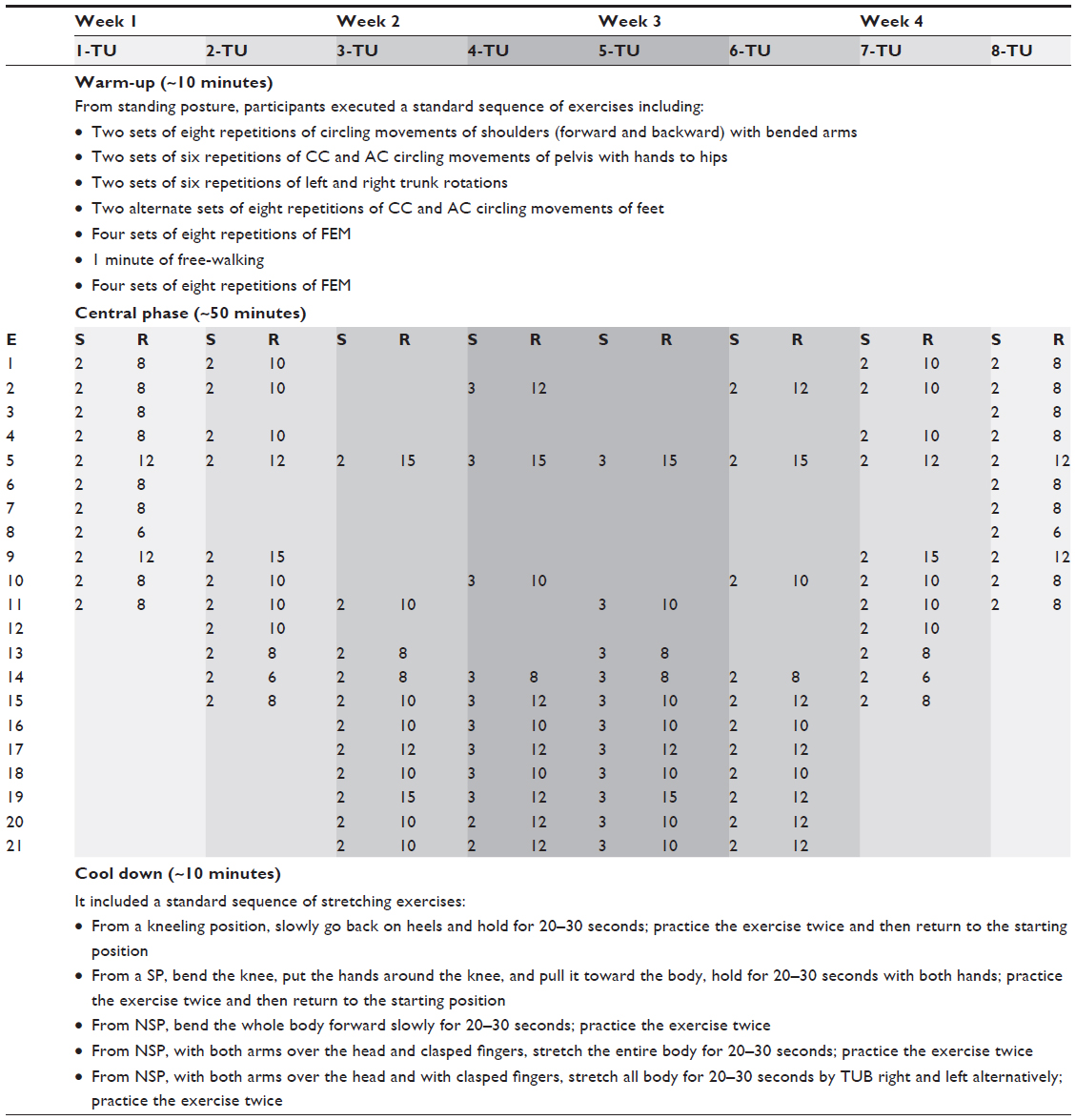 | Table 1 Mesocycle training |
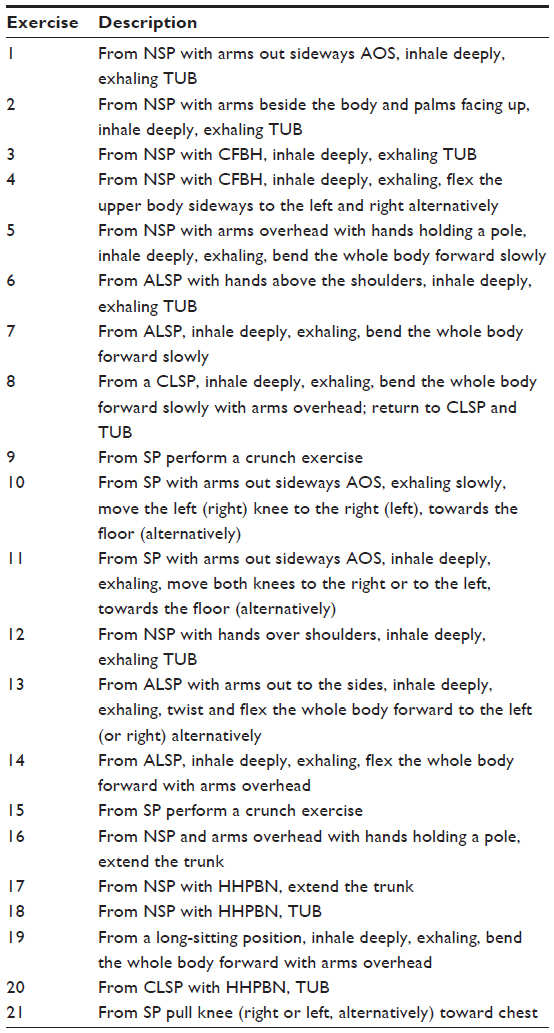 | Table 2 Description of exercises in central phase training. |
Statistical analysis
Results were expressed as means ± standard deviation. Two-way analysis of variance with repeated measures was used to evaluate differences over time in anthropometric parameters, Berg balance score, and spinal measures (thoracic and lumbar ROMs and sacral/hip and spinal inclination) between control and training groups in response to treatment. Time (baseline – posttest) × group (control-trained) interaction was considered, and the Bonferroni correction was applied as a post hoc test. Between-group comparisons at posttest by the analysis of covariance (ANCOVA) approach, using baseline scores as covariate, were performed when differences in pretest means were observed. Statistical significance was accepted as P<0.05. Levene’s test was used to assess the homogeneity of variance.
All data were analyzed using STATISTICA 8.0 software, version 10 (Statsoft Inc., Tulsa, OK, USA).
Results
Our research question was whether the means change in the outcome, from pre- to posttest, differed in the CG and TG groups in response to treatment. We performed an evaluation of differences among the two groups at baseline, followed by the assessment of posttraining differences between groups. In data analysis, two members of the TG group were excluded from the study because they did not attend 80% of the training; instead, five participants of CG were not considered because they were not subjected to the second assessment because of personal reasons. For these motivations, 30 women (17 trained subjects [TG] and 13 untrained ones [CG]) were considered for statistical analysis.
Data investigations revealed a normal distribution of variance for each dependent variable. We observed that both at baseline and after the experimental period, the TG and CG were equivalent in age, anthropometric characteristics, and Berg balance score (Tables 3 and 4). Moreover, before training, the two groups showed similar total ROMs (Table 3). Different values in spinal measures at baseline were used as covariates in ANCOVA analysis of posttest means.
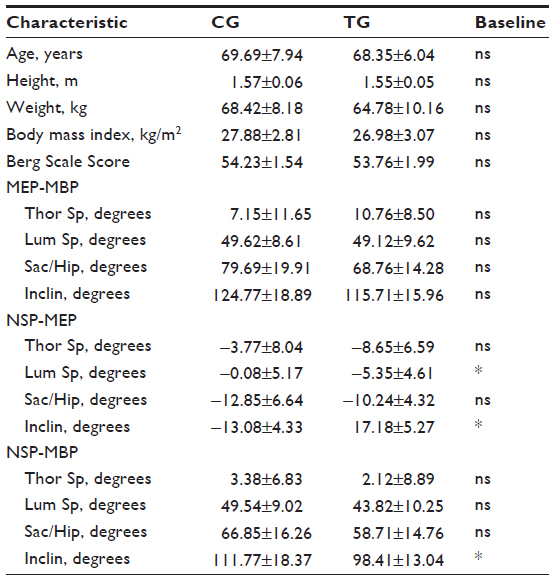 | Table 3 Characteristics of cohort at baseline |
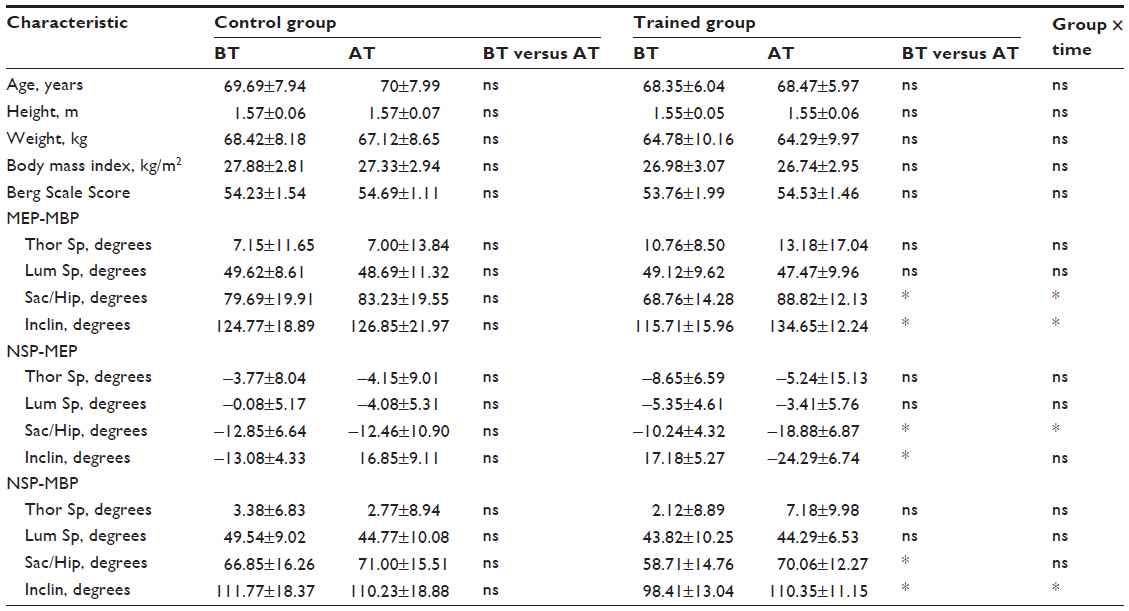 | Table 4 Assessment of measures and spinal ROMs in response to the training program |
The two-way analysis of variance with repeated measures with Bonferroni post hoc test indicated an increase in spinal inclination (16.4%; P<0.05) and sacral/hip (29.2%; P<0.05) and thoracic (22.5%; P>0.05) ROM, from MEP to maximum bending position (MBP), in the TG compared with the CG after the training period. Otherwise, the TG did not show any significant difference in the lumbar spine ROM compared with the CG (Table 4).
Comparisons between posttest means, adjusted for pretest scores in an ANCOVA analysis, revealed that from NSP to MEP, the TG did not show any significant difference in spinal inclination or lumbar and thoracic ROM after the training program compared with CG (Table 4). The TG showed, instead, a significant increment in sacral/hip value by 34% (P<0.05) compared with the CG at posttest.
As far as concerns measurements from NSP to MBP, we did not observe any significant difference in sacral/hip, lumbar, and thoracic ROMs in the TG compared with the CG after the training period. In contrast, at posttest, the spinal inclination value increased by 12.1% (P<0.05) in the TG compared with in the CG.
Discussion
Physical activity gradually decreases in elderly subjects, and a sedentary lifestyle is a risk factor for a decline in their state of health. It is important to increase methodological indications for exercise programs for elderly people. We used an innovative training protocol, including several combined exercises for core stability and spine flexibility, in order to oppose the aging-related ROM reduction of the spine.
The present study showed that elderly women who took part in the special flexibility training program showed enhanced ROMs in specific regions of the spine. After 8 weeks of training, exercised participants reported an increased total thoracic ROM (22.5%) in the spine compared with those in the CG. We did not find any significant difference in members of the TG’s total lumbar ROM from baseline to posttest. In contrast, after the training period, the TG showed a higher thoracic ROM of spine, compared with the CG, from upright posture to maximal bending position. Our results are consistent with previous investigations that highlighted increased ROMs in the major muscle–tendon groups in response to a specific flexibility training program.21–23 Girouard and Hurley found significant increases in hip and shoulder ROMs in elderly men after a 10-week period of flexibility exercise, including static stretching movements.22 Feland et al showed that 60 seconds of stretching, repeated 4 times (once a day, 5 times/week, for 6 weeks) could improve knee extension ROM more than similar regimens of 15 or 30 seconds of stretching in elderly people.23 However, 15–30 seconds of stretching (as in our training protocol) increased knee ROM in a stretched group when compared with a group that had no stretching.23
In agreement with several studies,24,11 we used a spinal flexibility training program including strength training (core stability), flexibility of spine, and stretching of the upper and lower body. Miyakoshi et al found that a decrease in spinal ROM had negative effects on quality of life in postmenopausal subjects with osteoporosis who were aged 50 years or older.24 In particular, they showed that the deterioration of back muscle strength was an important factor reducing ROM of spine.24 For these reasons, we included in our protocol several combined exercises (see Tables 1 and 2) to train, at the same time, core stability and spinal flexibility in the elderly women involved in the study. A good thoracic ROM, together with a good lumbar ROM and back muscle strength, appear to be related to the maintenance of the sagittal balance in middle-aged and elderly subjects.11 Imagama et al reported that an exercise training program including muscle strength and spinal flexibility exercises could be able to influence lumbar lordosis angle, sagittal balance, spinal ROM, and back muscle strength in middle-aged and elderly people.11
According to these findings, our original flexibility training protocol with a specific modulation in sets and repetitions of exercises during the training period appeared to be able to increase the thoracic ROM of the spine, which was known for being related to the maintenance of sagittal body balance.11 In addition, our results showed that the TG did not improve the thoracic and lumbar ROMs from NSP to MEP after the training period. These findings might be related to few spinal extension exercises included in our training protocol (see Tables 1 and 2). In contrast, the relevant improvement in the TG’s thoracic ROM, from baseline to posttest, during upright maximal bending test might be related to several spinal flexion exercises (see Tables 1–3) that we included in mesocycle training. Moreover, from baseline to posttest, we found that the TG significantly increased total and partial sacral/hip ROMs and spinal inclination compared with the CG. Probably, several TUB (twist the upper body to the left and right raising both arms over the head alternatively) exercises included in our training protocol had improved the sacral/hip ROM and spinal inclination in the TG compared with the CG. Rider and Daly reported that the spinal mobility of elderly women could be improved by regular participation in a flexibility training program. This study showed that after 10 weeks of a series of flexibility exercises (three times per week for 20–30 minutes of training per unit), trained elderly women increased their spinal flexion and extension compared with untrained subjects.15
With regard to the motivational aspect, our training protocol appeared to be particularly appropriate to encourage subjects to participate and adhere to the training program. Participation in an exercise training program is very difficult in all age groups, but particularly in elderly people, adherence to a physical activity period is challenging.25 Among elderly adults, there are several factors that have been identified as barriers to a regular exercise practice, including perceived poor health, low motivation, poor self-confidence, and perceived exercise enjoyment.26 Although we did not measure the level of satisfaction in studied subjects during the experimental period, we observed that in nearly every case, trained elderly woman attended at least 80% of the training periods (TG’s drop-out rate, 2/19). In the CG, we observed, instead, a high drop-out rate (5/18 subjects) for personal reasons, probably a result of the absence of motivational strategies in our experimental design. We speculated that the involvement of the CG in nonphysical activities (forums, reading workshops, occupational laboratories) or periodic telephone calls could limit the drop-out in the CG. Moreover, another limitation of this study was not to have measured subjective outcomes, such as perceived pain by trained subjects during the experimental period. Further studies are needed, therefore, to understand the effects of this specific flexibility training program on the health status of elderly people.
Conclusion
In conclusion, our findings indicate that the flexibility training protocol performed for 8 weeks could improve spinal ROMs in elderly women. These data might be suitable for increasing knowledge about the methodology of geriatric gymnastics. In particular, this study showed that a specific workload pattern (set, repetitions, type of exercise) could increase spinal ROM in elderly women. Moreover, we observed that the training protocol was practicable and safe for active elderly people with autonomy and the capability for self-care. In agreement with American College of Sports Medicine, this study could support the consensus in the prescription of flexibility exercises to improve spinal ROM and quality of life in elderly people.
Acknowledgments
We thank Marcello Saieva and Teresa Guglielmo for their support and assistance during the experimental period. We also acknowledge all the elderly women who were involved in the local project “Volare” of the Associazione Italiana Cultura Sport of Palermo.
Disclosure
The authors report no conflicts of interest in this work.
References
Aijö M, Heikkinen E, Schroll M, Steen B. Physical activity and mortality of 75-year-old people in three Nordic localities: a five-year follow-up. Aging Clin Exp Res. 2002;14(Suppl 3):83–89. | |
Hongo M, Itoi E, Sinaki M, et al. Effect of low-intensity back exercise on quality of life and back extensor strength in patients with osteoporosis: a randomized controlled trial. Osteoporos Int. 2007;18(10):1389–1395. | |
Smith RL, Mell DB. Effects of prone spinal extension exercise on passive lumbar extension range of motion. Phys Ther. 1987;67(10):1517–1521. | |
Hirano K, Imagama S, Hasegawa Y, Wakao N, Muramoto A, Ishiguro N. Impact of spinal imbalance and back muscle strength on locomotive syndrome in community-living elderly people. J Orthop Sci. 2012;17(5):532–537. | |
León-Muñoz LM, Martínez-Gómez D, Balboa-Castillo T, López-García E, Guallar-Castillón P, Rodríguez-Artalejo F. Continued sedentariness, change in sitting time, and mortality in older adults. Med Sci Sports Exerc. 2013;45(8):1501–1507. | |
Bellafiore M, Battaglia G, Bianco A, Paoli A, Farina F, Palma A. Improved postural control after dynamic balance training in older overweight women. Aging Clin Exp Res. 2011;23(5–6):378–385. | |
Bianco A, Patti A, Bellafiore M, et al. Group fitness activities for the elderly: an innovative approach to reduce falls and injuries. Aging Clin Exp Res. Epub September 21, 2013. | |
Battaglia G, Bellafiore M, Bianco A, Paoli A, Palma A. Effects of a dynamic balance training protocol on podalic support in older women. Pilot Study. Aging Clin Exp Res. 2010;22(5–6):406–411. | |
Seco J, Abecia LC, Echevarría E, et al. A long-term physical activity training program increases strength and flexibility, and improves balance in older adults. Rehabil Nurs. 2013;38(1):37–47. | |
Figueira HA, Figueira AA, Cader SA, et al. Effects of a physical activity governmental health programme on the quality of life of elderly people. Scand J Public Health. 2012;40(5):418–422. | |
Imagama S, Matsuyama Y, Hasegawa Y, et al. Back muscle strength and spinal mobility are predictors of quality of life in middle-aged and elderly males. Eur Spine J. 2011;20(6):954–961. | |
Stathokostas L, Little RM, Vandervoort AA, Paterson DH. Flexibility training and functional ability in older adults: a systematic review. J Aging Res. 2012;2012:306818. | |
Gajdosik RL, Vander Linden DW, McNair PJ, Williams AK, Riggin TJ. Effects of an eight-week stretching program on the passive-elastic properties and function of the calf muscles of older women. Clin Biomech (Bristol, Avon). 2005;20(9):973–983. | |
Reid DA, McNair PJ. Effects of a six week lower limb stretching programme on range of motion, peak passive torque and stiffness in people with and without osteoarthritis of the knee. N Z J Physiother. 2011;39(1):5–9. | |
Rider RA, Daly J. Effects of flexibility training on enhancing spinal mobility in older women. J Sports Med Phys Fitness. 1991;31(2):213–217. | |
Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK; American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2009;41(2):459–471. | |
Bogle Thorbahn LD, Newton RA. Use of the Berg Balance Test to predict falls in elderly persons. Phys Ther. 1996;76(6):576–583. | |
Faulkner G, Cohn T, Remington G, Irving H. Body mass index, waist circumference and quality of life in individuals with schizophrenia. Schizophr Res. 2007;90(1–3):174–178. | |
Post RB, Leferink VJ. Spinal mobility: sagittal range of motion measured with the SpinalMouse, a new non-invasive device. Arch Orthop Trauma Surg. 2004;124(3):187–192. | |
Battaglia G, Alesi M, Inguglia M, et al. Soccer practice as an add-on treatment in the management of individuals with a diagnosis of schizophrenia. Neuropsychiatr Dis Treat. 2019:595–603. | |
Garber CE, Blissmer B, Deschenes MR, et al; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334–1359. | |
Girouard CK, Hurley BF. Does strength training inhibit gains in range of motion from flexibility training in older adults? Med Sci Sports Exerc. 1995;27(10):1444–1449. | |
Feland JB, Myrer JW, Schulthies SS, Fellingham GW, Measom GW. The effect of duration of stretching of the hamstring muscle group for increasing range of motion in people aged 65 years or older. Phys Ther. 2001;81(5):1110–1117. | |
Miyakoshi N, Hongo M, Maekawa S, Ishikawa Y, Shimada Y, Itoi E. Back extensor strength and lumbar spinal mobility are predictors of quality of life in patients with postmenopausal osteoporosis. Osteoporos Int. 2007;18(10):1397–1403. | |
Dishman RK, Buckworth J. Increasing physical activity: a quantitative synthesis. Med Sci Sports Exerc. 1996;28(6):706–719. | |
Lee LL, Arthur A, Avis M. Using self-efficacy theory to develop interventions that help older people overcome psychological barriers to physical activity: a discussion paper. Int J Nurs Stud. 2008;45(11):1690–1699. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.