")
Back to Journals » Research Reports in Clinical Cardiology » Volume 5
Cardiovascular protection in type 2 diabetes: time to ADVANCE management ACCORDing to the evidence
Authors Hajhosseiny R, Khavandi K, Mashayekhi S, Greenstein A, Malik R
Received 3 September 2013
Accepted for publication 30 September 2013
Published 31 December 2013 Volume 2014:5 Pages 1—9
DOI https://doi.org/10.2147/RRCC.S34415
Review by Single anonymous peer review
Peer reviewer comments 2
Reza Hajhosseiny,1 Kaivan Khavandi,1 Soudeh Mashayekhi,2 Adam S Greenstein,3 Rayaz A Malik3
1British Heart Foundation Centre of Cardiovascular Excellence, St Thomas' Hospital, London, UK; 2Department of Primary Care and Public Health, Imperial College London, London, UK; 3Institute of Human Development, University of Manchester, Manchester, UK
Abstract: Individuals with type 2 diabetes mellitus are at very substantial risk of cardiovascular disease, and most will succumb to complications from premature coronary artery events. At the same time, the diabetic myocardium undergoes unique phenotypic alterations as a consequence of multiple structural and cellular injuries, which together form "diabetic cardiomyopathy." Attempts to curb risk through intensive modulation of glycemia and blood pressure have proven disappointing in preventing cardiovascular events, and potentially even dangerous. Conversely, prior to development of disease, there appears to be a linear relationship between risk parameters and events. These observations are likely the consequence of widespread vascular damage, which is present at the point that glycemic thresholds meet diagnostic criteria for diabetes. This is particularly true of the microcirculation. Interventions at the prediabetic stage have been consistent with this, where early intensive risk-factor modulation has been successful in preventing events and even regressing existing risk. Upstream, the force driving these pathologies is being overweight and obesity. High-risk individuals can be identified through simple body mass parameters, with confirmation of prediabetes/metabolic syndrome with further assessment of other metabolic parameters such as glucose and lipids. A number of novel pharmacotherapies may prove beneficial at this stage, and incretin-based therapies appear particularly promising in this respect. Similarly, bariatric procedures have shown remarkable improvements in metabolic and cardiovascular outcomes, but are clearly unsuitable as a population-wide strategy. Therapeutic lifestyle change and diet have consistently shown efficacy in reversing dysglycemia, lowering blood pressure, and optimizing cholesterol profiles. However, the longevity of these improvements is often limited, and alternative approaches therefore need to be considered. With an evolving and increasingly sophisticated evidence base for nutritional interventions, there is a clear window of opportunity to rescue these individuals from the clinical sequelae of diabetes and consequent cardiovascular complications.
Keywords: hypertension, diabetes, cardiovascular risk
Introduction
The prevalence of type 2 diabetes mellitus (T2DM) continues to rise, with over 360 million affected worldwide in 2011 and forecast to reach 550 million by 2030.1 The financial impact of this global epidemic is devastating, with approximately 10% of the entire UK National Health Service budget spent on diabetes.2 Alarmingly, low/middle-income countries have the highest projected increase in prevalence, which threatens to rapidly overwhelm resource-deprived health care systems.1 Complications from T2DM are broad and progressive. Microvascular injury begins early in the disease process, and causes substantial morbidity through retinopathy, neuropathy, and nephropathy, whilst macrovascular disease, most notably cardiovascular events, are responsible for the majority of deaths.3,4 Treatment of established coronary heart disease is challenging in these patients, with atypical or silent presentations of acute myocardial infarcts.5 Percutaneous coronary intervention is also typically more complex.6 The focus has therefore been on reducing cardiovascular risk, and adopting an empirical approach of more intensified treatment targets. In this review, we summarize some of the recent trials that have addressed the issue of optimal risk-factor control in diabetes, and provide potential explanations for their findings.
Mechanisms of risk and disease
The pathophysiology of T2DM involves both insulin resistance and reduced insulin production, through progressive pancreatic beta-cell dysfunction.7 Chronic insulin resistance demands increased activity of pancreatic beta cells to secrete insulin. These cells eventually decompensate, and hyperglycemia follows.7 There is an intermediary, or “prediabetic” stage between normoglycemia and overt DM, which can involve impaired fasting glucose (IFG), where fasting plasma glucose is 6.1–6.9 mmol/L, or impaired glucose tolerance (IGT), where plasma glucose 2 hours after a 75 g glucose load is 7.8–11.0 mmol/L.8 The cardiovascular risk associated with hyperglycemia exists across this spectrum, from early dysglycemia to prediabetes and T2DM. By the time a formal diagnosis is made, there is already significant cardiac risk.8 Indeed, one-third of patients with coronary artery disease have abnormal oral glucose-tolerance test results, and 22% with acute and 14% with stable coronary heart disease have newly diagnosed T2DM. As such, there is clear excess cardiovascular risk with IFG9 and IGT.10 The underlying mechanisms are legion. Diabetic individuals experience accelerated atherosclerosis,11 which is itself multifactorial. Dyslipidemia plays a central role, typically including elevated triglycerides and decreased high-density lipoprotein (HDL) cholesterol.12 Along with dysglycemia, this lipid profile is frequently seen in combination with obesity and high blood pressure, which together form metabolic syndrome, a highly atherogenic predisease condition. Diabetic individuals also exhibit elevated levels of small-dense, low density lipoprotein (LDL) cholesterol, which are more penetrating and particularly susceptible to oxidation.11 Lipoproteins are also the subject of glycation with elevated blood sugars, which increases the half-life of LDL cholesterol but reduces that of HDL.13,14
Microvascular injury develops as a consequence of a variety of molecular pathways, including alterations in redox and inflammatory states. Diabetes is independently associated with endothelial dysfunction,15 tipping the balance of vasoactive agents in favor of vasoconstriction, with increased levels of endothelin 1 and other constricting factors, contributing to increased peripheral vascular resistance and hypertension.11,16 Angiotensin II type 1 (AT1)-receptor activation is associated with increased free radical release and oxidative stress.17,18 We have previously shown that blocking the AT1 receptors with an angiotensin-receptor blocker is associated with significant improvement in resistance-vessel endothelial function in patients with T2DM.18 Cardiac autonomic neuropathy is common in T2DM and an independent risk factor for cardiovascular events.11,19,20 Corneal confocal microscopy is a powerful tool for the early detection of small-fiber damage in diabetes and prediabetes.21 Autoregulation of the small arteries is also lost in diabetes. Schofield et al demonstrated impaired myogenic responsiveness in small arteries from individuals with T2DM,22 which is thought to be the trigger to arterial wall hypertrophy and structural detriment.23 Hyperglycemia also leads to capillary basement-membrane thickening, resulting in impaired transport of metabolites and nutrients between the circulation and tissues.24 Interestingly, in patients with T1DM, improved metabolic profiles can result in regression of maladaptive hypertrophic changes of small arteries to the more favorable eutrophic remodeling.25 Many of these mechanisms – autonomic dysfunction, microvascular disease, alterations to reactive oxygen species, and intracellular calcium homeostasis – lead to cellular, structural, and functional injuries, which lead to diabetic cardiomyopathy. There are a number of dedicated reviews focusing on this subject.15,26,27
Optimizing cardiovascular risk: glycemic control
The UK Prospective Diabetes Study (UKPDS) was a randomized, prospective, multicenter trial of intensive glucose therapy in subjects with newly diagnosed T2DM.28 The trial reported significantly reduced risk of clinically evident microvascular complications in those receiving intensive intervention,28 with macrovascular benefits becoming apparent with long-term follow-up.4 These findings have not been reproduced in recent randomized controlled trials (summarized in Table 1): the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation)29 trial and VADT (Veterans Affairs Diabetes Trial)30 failed to show improved outcomes in terms of cardiovascular disease, microvascular complications, and mortality with intensive glycemic control. Indeed the ACCORD (Action to Control Cardiovascular Risk in Diabetes)31 trial showed a trend towards increased mortality with intensive glycemic control, leading to premature termination of the trial. The reasons behind these findings are unclear, though a number of potential causes have been postulated. There was worse prognosis amongst intensively treated patients with one or more episodes of severe hypoglycemia, but secondary analysis of all patients suffering hypoglycemic events requiring assistance showed a nonsignificant trend to lower mortality risk with intensive therapy.32 Furthermore, only one of 451 deaths in the ACCORD trial were conclusively a consequence of hypoglycemia. The substantial weight gain in intensively treated patients is also concerning, but was not shown to be associated with mortality. Indeed, these findings have led to changes in the clinical recommendation for risk targets, though there is some discrepancy between guidelines. The American Diabetes Association (ADA), the American Heart Association (AHA), the American College of Cardiology (ACC) Foundation, and the Australian Diabetes Association still advise target glycosylated hemoglobin (HbA1c) levels <7%, presumably due to evidence for protection from microvascular complications.33 The National Institute of Clinical Excellence (NICE) has now altered HbA1c targets from <6.5% to between 6.5% and 7.5%,34 in conjunction with recent evidence. Similarly, the International Diabetes Federation has recently changed targets for HbA1c from <6.5% to <7%,35 and the joint European Society of Cardiology (ESC) and European Association for the Study of Diabetes recommend targets between 6.5% and 7.0%.36
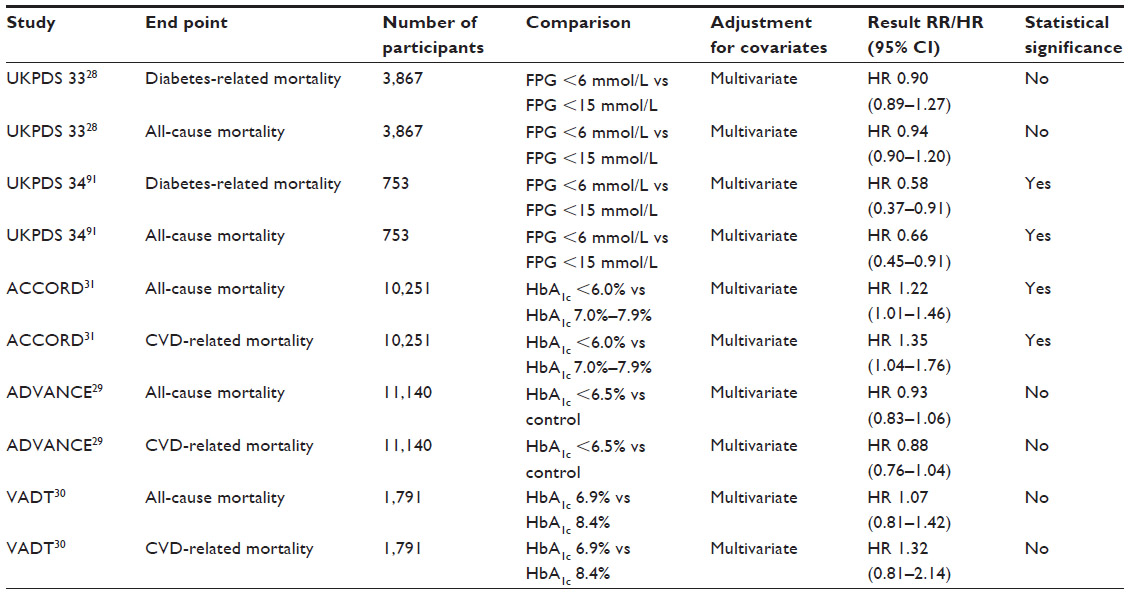 | Table 1 Comparison of glycemic targets on major diabetes-related and cardiovascular outcomes |
Blood pressure control
The UKPDS showed intensive blood pressure lowering was associated with major reductions in important clinical end points, including a 32% reduction in diabetes-related death, 44% reduction in stroke, and 37% reduction in microvascular end points.33,37 At the same time, the Hypertension Optimal Trial (HOT) demonstrated a significantly lower rate of cardiovascular events and mortality in individuals with T2DM with intensely controlled blood pressure, compared with standard management.38 In the ABCD (Appropriate Blood Pressure Control in Diabetes) trial,39 intense blood pressure control was not associated with improved cardiovascular end points after 5 years of follow-up. The ACCORD trial randomized patients with T2DM to either intensive blood pressure control (BP <120 mmHg) or conventional therapy. Although an impressive reduction in blood pressure to 119/64 mmHg was achieved with intensive treatment, this was not associated with an improvement in cardiovascular end points compared with a blood pressure of 134/71 mmHg.40 It should be noted that participants in the ACCORD trial were recruited 10 years after diagnosis, and as such there was a high prevalence of preexisting cardiovascular disease.33 These findings were further supported in ADVANCE41 and INVEST,42 which did not support blood pressure lowering below 130 mmHg systolic. There is now consensus for a U-shaped relationship between blood pressure control and cardiovascular-related end points in T2DM, with no evidence for a benefit in blood pressure reduction below 130 mmHg33,43 and potential for adverse hypotension, hypokalemia, bradycardia, and renal impairment. This is now reflected in major guidelines, with the AHA, ADA, NICE, and ESC no longer recommending blood pressure reduction <130/80 mmHg.33 There are exception groups at particular risk of cerebrovascular accidents, such as those with transient ischemic attacks, or certain ethnic groups, such as African Caribbeans and South Asians,33,44 where a lower blood pressure target might be justified. Table 2 summarizes the main trials investigating blood pressure targets on cardiovascular outcomes in T2DM.
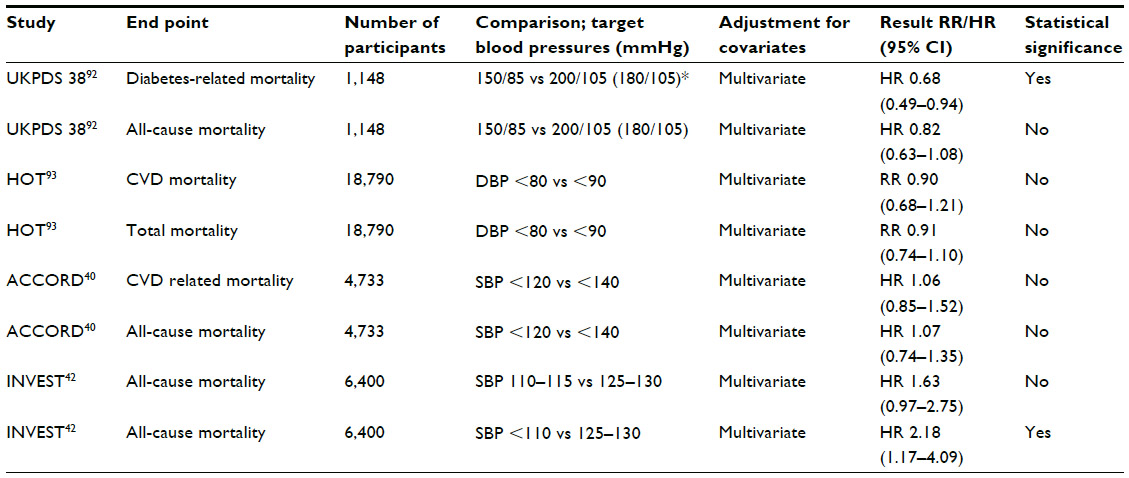 | Table 2 Comparison of blood pressure targets on major diabetes-related and cardiovascular outcomes |
Taking the results from UKPDS, ADVANCE, VADT, and ACCORD together, there is a suggestion that intensive glycemic modification is beneficial in the early stages of diabetes, but that this opportunity is lost later in disease. Indeed, subgroup analysis of the VADT and ACCORD trials showed that patients free of cardiovascular disease and with a recent diagnosis of diabetes gained the most benefit from intensive glycemic control.33 Indeed, the concept of a “legacy effect” has gained interest after extended follow-up of trials, where an early, transient phase of tight glycemic control may have benefit extending many years after the intervention period. Following completion of the UKPDS, participants in the glycemic control arm were asked to attend annual UKPDS clinics for an additional five years, but no attempts were made to maintain their previously assigned therapies. A further 5 years of follow-up was established through annual questionnaires. One year after closure of the trial, between-group differences in glycemic control were lost, yet after 10 years of follow-up, those assigned to the intensive control arm with sulfonylurea and insulin had significantly reduced risks for microvascular disease (24%), myocardial infarction (15%), death from any cause (13%), and any diabetes-related end point (9%), compared with subjects assigned to conventional therapy.45 Similar results were seen in those assigned to metformin compared to controls.
A similar post-trial follow-up of the hypertension arm of the UKPDS has also been performed. Between-group differences in blood pressure control were lost 2 years after closure of the trial. Surprisingly, 51% of the trial participants had died by the 10-year follow-up post-closure of the trial.45 Additionally, the significant benefits in terms of diabetes-related end points, diabetes-related death, microvascular disease, and stroke established during the trial with tight blood pressure control were not sustained after the post-trial follow-up.45 The evidence for a legacy effect of tight blood pressure control in diabetes is therefore lacking, and indeed for initial benefits to be sustainable, blood pressure control must be sustained consistently over time.
Primordial prevention
An increasingly overweight and obese population is the primary force responsible for the rising prevalence of T2DM. The Nurses’ Health Study followed 84,941 females for up to 16 years, and reported a relative risk of diabetes of 38.8 and 20.2 for women with a body mass index (BMI) ≥35 and 30–34.9 kg/m2, respectively, compared with women who had a BMI <23 kg/m2. Weight loss improves outcomes in T2DM and delays or prevents progression from IGT/IFG to diabetes. Epidemiological data from the Framingham study46 have shown that sustained weight loss in overweight individuals can have a primary preventative effect on the incidence of T2DM. As a result, many strategies aimed at preventing T2DM have focused primarily on weight loss. The largest study to date was conducted by the Diabetes Prevention Program47 (DPP) research group. This involved 3,234 nondiabetic (ethnically and racially diverse) individuals with IGT of mean age 51 years and BMI 34 kg/m2 randomized to placebo, metformin, or lifestyle intervention. The lifestyle-intervention group were expected to maintain a weight reduction of 7% through dietary means and physical activity, performing at least 150 minutes of moderate-intensity activity per week. Lifestyle intervention was associated with an impressive 58% reduction in the incidence of diabetes when compared with placebo and was superior to metformin. Indeed, for every 1 kg reduction in weight, there was an associated 16% reduction in the incidence of diabetes. Follow-up studies have confirmed that this preventative or delaying effect persists at 10 years.48 Similar outcomes have been shown in the Finnish Diabetes Prevention Study49 and the Chinese Da Qing IGT and Diabetes Study50 where intense weight-loss interventions in IFG/IGT delayed/prevented the onset of full-blown T2DM. Indeed, Gregg et al51 have recently shown that intense weight-loss interventions (limiting calorie intake to 1,200–1,800 kcal/day and 175 minutes of physical activity/week) resulted in a significant partial remission of diabetes, defined as transition from meeting diabetes criteria to a prediabetes level of glycemia. However, recently in a cohort of overweight or obese individuals with T2DM, the Look AHEAD (Action for Health in Diabetes) research group52 failed to show any reduction in cardiovascular events with intense intervention focusing on weight loss (through reduced calorie intake and increased physical activity), despite greater reduction in individual risk parameters. This emphasizes that nonpharmacological interventions may be less effective later in the course of diabetes. Looking beyond weight loss alone, data have begun to accrue reporting on the efficacy of specific nutritional interventions in reducing risk factors and preventing hard cardiovascular end points.
Although nutritional evidence has been muddied by claims from pseudoscientific fad diets introduced by media figures and food corporations, powerful data and high-quality evidence do exist for effective dietary interventions. The Early ACTID (Early ACTivity In Diabetes trial) was a randomized controlled trial that investigated the effects of an intense dietary regime (the Diabetes UK dietary guidelines53) on glycemic control in 593 T2DM patients. The study found that intensive dietary intervention when instituted soon after diagnosis improved glycemic control.54 The DASH (Dietary Approaches to Stop Hypertension) trial demonstrated that a dietary pattern consisting of (potassium-rich) vegetables, fruit, nuts, seeds, whole grains, and low-fat dairy products and low in meat, poultry, eggs, salt, and overall fat diet was effective in reducing blood pressure.55 The DASH diet was subsequently shown also to prevent or reverse the onset of T2DM.56 More recently, the Mediterranean diet (consisting of plenty of fruit and vegetables, olive oil, seafood, oily fish, and wine) was tested in a multicenter randomized controlled trial (the PREDIMED [Prevención con Dieta Mediterránea] trial)57 in 7,447 patients at high risk of cardiovascular complications, compared with a control arm that involved advice to reduce dietary fat. The primary end-point event was myocardial infarction, stroke, or death from cardiovascular causes. Multivariable-adjusted hazard ratios were 0.70 (95% confidence interval [CI] 0.54–0.92) and 0.72 (95% CI 0.54–0.96) in those assigned to a Mediterranean diet with extra-virgin olive oil (96 events) and the group assigned to a Mediterranean diet with nuts (83 events), respectively, versus the control group (109 events). There were no reports of diet-related adverse effects. A recent meta-analysis of 20 randomized controlled trials, involving 3,073 patients with T2DM, low-carbohydrate, Mediterranean, and high-protein diets all led to an improvement in glycemic control (HbA1c reductions of −0.12% [P=0.04], −0.47% [P<0.00001], and −0.28% [P<0.00001], respectively) compared with their respective control diets, with the largest effect size seen in the Mediterranean diet, which was incidentally associated with the greatest weight loss.58 Although yet to be tested in large trials, dietary sources rich in inorganic nitrates (eg, beetroot, rocket, and rhubarb) may provide an alternative source of nitric oxide that can be supplied by the serial conversion of inorganic nitrates to nitric oxide and other bioactive nitrogen oxides.59,60 Carlström et al59 produced a near-complete compensation of nitric oxide in endothelial nitric oxide synthase-deficient mice through dietary supplementation with sodium nitrate. Early clinical studies have been very promising in terms of blood pressure reduction,61 and further trials are in development. Table 3 summarizes some of the larger studies investigating the effects of nutritional and lifestyle interventions on major diabetes and cardiovascular outcomes.
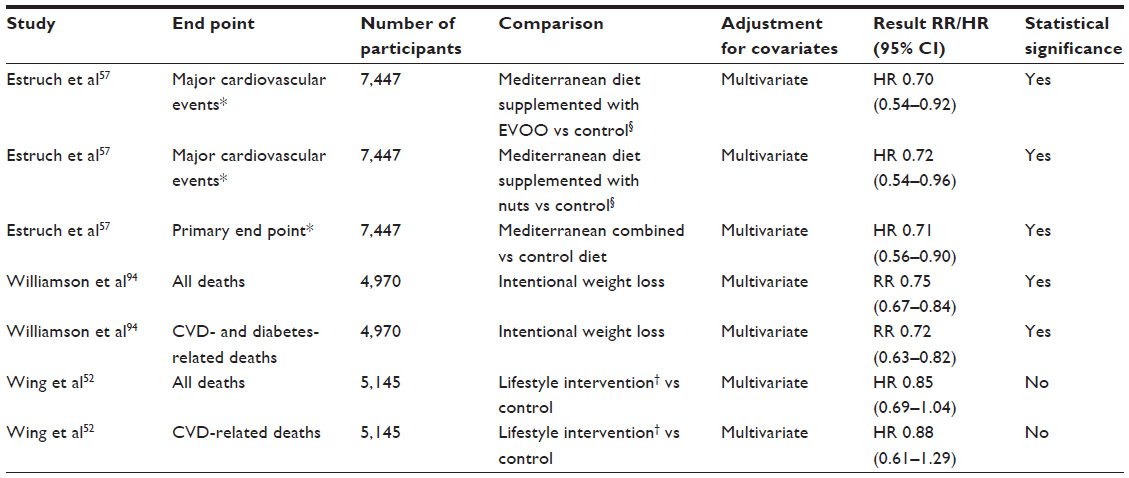 | Table 3 Studies employing lifestyle or nutritional interventions as primary prevention strategies in relation to cardiovascular outcomes |
We now know that the effects of vitamin D extend beyond traditional roles in bone metabolism and skeletal mineralization, and strong associations exist with cardiometabolic health and disease. In addition to numerous epidemiological studies linking vitamin D insufficiency/deficiency with diabetes,62–66 parallel mechanistic studies have shown the vitamin D receptor ubiquitously expressed. Experimental studies of animal models have shown high doses of active vitamin D to prevent diabetes,67 with underlying mechanisms involving modification of dendritic cell phenotype, lymphocyte proliferation, and cytokine production,68,69 as well as direct effects of vitamin D on insulin action.70,71 Vitamin D promotes the action of insulin in skeletal muscle and adipose tissue, through its effect on calcium handling.72,73 Treatment with cholecalciferol has been shown to increase the disposition index (which reflects insulin action) in a population at risk of developing diabetes.74 Further, recent analysis of the DPP data showed those individuals in the highest tertile of vitamin D levels had a hazard ratio of 0.74 for developing diabetes when compared with those in the lowest tertile. Meta-analysis data have also supported evidence for a relationship between low vitamin D status, calcium or dairy dietary intake, and prevalence of T2DM, metabolic syndrome,75,76 and obesity.77,78 Central to the mechanisms proposed for the observed associations between vitamin D levels, hypertension, and diabetes is alterations to the renin–angiotensin–aldosterone system. A recent systematic review of the relationship between vitamin D levels and arterial hypertension by Pilz et al concluded that adequate levels of vitamin D are associated with lower arterial blood pressures, and that the antihypertensive effect of vitamin D is greatest in individuals with a combination of both vitamin deficiency and a previous diagnosis of hypertension.79 Although there is evidence supporting the blood pressure-lowering effect of vitamin D from a number of other small trials,80 there remains a paucity of adequately powered trials to prove a cause-and-effect relationship to support these observations, and the results of VITAL (VITamin D and OmegA-3 TriaL) are eagerly anticipated.81
A number of pharmacological and surgical strategies have been effective at preventing diabetes and reducing associated cardiovascular risk. The gastrointestinal lipase inhibitor orlistat has been shown to significantly lower fasting plasma glucose and HbA1c levels.82 Newer incretin-based therapies, such as glucagon-like peptide-1 agonists/analogs83 and dipeptidyl peptidase-4 inhibitors,84 form a particularly promising group of antidiabetic medications, with parallel benefits in weight reduction and possibly cardiovascular risk. For a comprehensive review, please see Khavandi et al.85 Bariatric surgery achieves weight loss by restrictive or malabsorptive mechanisms, and has shown some truly remarkable metabolic outcomes in tandem with weight reduction. The Roux-en-Y gastric bypass, a combination of the two, is associated with the best outcomes and is therefore accepted as the criterion standard.86 Long-term outcomes in patients undergoing obesity surgery have confirmed a reduction in overall mortality when compared with conventional treatment for obesity.87 Evidence suggests that bariatric surgery can also induce long-term remission of T2DM in both obese and morbidly obese patients.88 It has become clear that these benefits extend beyond those explained simply by the reduced capacity for consumption, with a wide array of alterations to gut hormones.89 Further mechanistic insights have been gained recently from investigation of the small arteries before and after bariatric interventions, which show alteration in the function of perivascular adipose tissue.90
Conclusion
DM confers an exceptionally high risk of cardiovascular disease. The traditional strategy has been to intensify interventions and achieve greater reductions in risk parameters. Recent randomized control trial data have failed to show benefit in terms of cardiovascular end points with this approach in patients with established T2DM. At an earlier stage in the disease course, however, there is potential to improve risk and prevent cardiovascular events through aggressive modulation of blood pressure and glycemia. Given the now-epidemic proportion of diabetes, an optimal approach to this global problem should involve dual reduction in cardiac risk and prevention of diabetes itself. This can be achieved through appropriate diet and therapeutic lifestyle change. Whilst weight loss per se has antihypertensive and antidiabetic benefits, more specific nutritional interventions are accruing evidence for their powerful potential to reduce cardiovascular risk and improve metabolic profiles. Dietary modification can therefore achieve substantial reductions in the incidence of T2DM and improve the cardiovascular health of the population. This will clearly require engagement from policy-makers as well as the medical community. In specific cohorts, novel agents targeting gut hormones and bariatric interventions have the potential to improve metabolic profiles in conjunction with weight loss and cardiovascular risk reduction, to complement nonpharmacological strategies.
Disclosure
The authors report no conflicts of interest in this work.
References
http://www.diabetes.org.uk/Documents/Reports/Diabetes-in-the-UK-2012.pdf Accessed on 14/08/2013. | |
Hex N, Bartlett C, Wright D, Taylor M, Varley D. Estimating the current and future costs of type 1 and type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabet Med. 2012;29(7):855–862. | |
Morrish NJ, Wang SL, Stevens LK, Fuller JH, Keen H. Mortality and causes of death in the WHO Multinational Study of Vascular Disease in Diabetes. Diabetologia. 2001;44 Suppl 2:S14–S21. | |
Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–1589. | |
Chiariello M, Indolfi C. Silent myocardial ischemia in patients with diabetes mellitus. Circulation. 1996;93(12):2089–2091. | |
Berry C, Tardif JC, Bourassa MG. Coronary heart disease in patients with diabetes: part II: recent advances in coronary revascularization. J Am Coll Cardiol. 2007;49(6):643–656. | |
Garber AJ. Obesity and type 2 diabetes: which patients are at risk? Diabetes Obes Metab. 2012;14(5):399–408. | |
Santaguida PL, Balion C, Hunt D, et al. Diagnosis, prognosis, and treatment of impaired glucose tolerance and impaired fasting glucose. Evid Rep Technol Assess (Summ). 2005;(128):1–11. | |
Shaw JE, Hodge AM, de Courten M, Chitson P, Zimmet PZ. Isolated post-challenge hyperglycaemia confirmed as a risk factor for mortality. Diabetologia. 1999;42(9):1050–1054. | |
Tominaga M, Eguchi H, Manaka H, Igarashi K, Kato T, Sekikawa A. Impaired glucose tolerance is a risk factor for cardiovascular disease, but not impaired fasting glucose. The Funagata Diabetes Study. Diabetes Care. 1999;22(6):920–924. | |
Dokken BB. The pathophysiology of cardiovascular disease and diabetes: beyond blood pressure and lipids. Diabetes Spectr. 2008;21(3):160–165. | |
Fagot-Campagna A, Gary TL, Benjamin SM. Cardiovascular risk in diabetes: a story of missed opportunities? Diabetes Care. 2001;24(11):2015–2016. | |
Napoli C, Triggiani M, Palumbo G, Condorelli M, Chiariello M, Ambrosio G. Glycosylation enhances oxygen radical-induced modifications and decreases acetylhydrolase activity of human low density lipoprotein. Basic Res Cardiol. 1997;92(2):96–105. | |
Bucala R, Makita Z, Koschinsky T, Cerami A, Vlassara H. Lipid advanced glycosylation: pathway for lipid oxidation in vivo. Proc Natl Acad Sci U S A. 1993;90(14):6434–6438. | |
Khavandi K, Khavandi A, Asghar O, et al. Diabetic cardiomyopathy – a distinct disease? Best Pract Res Clin Endocrinol Metab. 2009;23(3):347–360. | |
Tessari P, Cecchet D, Cosma A, et al. Nitric oxide synthesis is reduced in subjects with type 2 diabetes and nephropathy. Diabetes. 2010;59(9):2152–2159. | |
Griendling KK, Minieri CA, Ollerenshaw JD, Alexander RW. Angiotensin II stimulates NADH and NADPH oxidase activity in cultured vascular smooth muscle cells. Circ Res. 1994;74(6):1141–1148. | |
Malik RA, Schofield IJ, Izzard A, Austin C, Bermann G, Heagerty AM. Effects of angiotensin type-1 receptor antagonism on small artery function in patients with type 2 diabetes mellitus. Hypertension. 2005;45(2):264–269. | |
Smith SE, Smith SA, Brown PM. Cardiac autonomic dysfunction in patients with diabetic retinopathy. Diabetologia. 1981;21(6):525–528. | |
Ewing DJ, Campbell IW, Clarke BF. The natural history of diabetic autonomic neuropathy. Q J Med. 1980;49(193):95–108. | |
Tavakoli M, Petropoulos IN, Malik RA. Assessing corneal nerve structure and function in diabetic neuropathy. Clin Exp Optom. 2012;95(3):338–347. | |
Schofield I, Malik R, Izzard A, Austin C, Heagerty A. Vascular structural and functional changes in type 2 diabetes mellitus: evidence for the roles of abnormal myogenic responsiveness and dyslipidemia. Circulation. 2002;106(24):3037–3043. | |
Khavandi K, Arunakirinathan M, Greenstein AS, Heagerty AM. Retinal arterial hypertrophy: the new LVH? Curr Hypertens Rep. 2013;15(3):244–252. | |
Hayden MR, Sowers JR, Tyagi SC. The central role of vascular extracellular matrix and basement membrane remodeling in metabolic syndrome and type 2 diabetes: the matrix preloaded. Cardiovasc Diabetol. 2005;4(1):9. | |
Greenstein AS, Price A, Sonoyama K, et al. Eutrophic remodeling of small arteries in type 1 diabetes mellitus is enabled by metabolic control: a 10-year follow-up study. Hypertension. 2009;54(1):134–141. | |
Asghar O, Al-Sunni A, Khavandi K, et al. Diabetic cardiomyopathy. Clin Sci. 2009;116(10):741–760. | |
Poornima IG, Parikh P, Shannon RP. Diabetic cardiomyopathy: the search for a unifying hypothesis. Circ Res. 2006;98(5):596–605. | |
[No authors listed]. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837–853. | |
Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–2572. | |
Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360(2):129–139. | |
Gerstein HC, Miller ME, Byington RP, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–2559. | |
Bonds DE, Miller ME, Bergenstal RM, et al. The association between symptomatic, severe hypoglycaemia and mortality in type 2 diabetes: retrospective epidemiological analysis of the ACCORD study. BMJ. 2010;340:b4909. | |
Rutter MK, Nesto RW. Blood pressure, lipids and glucose in type 2 diabetes: how low should we go? Re-discovering personalized care. Eur Heart J. 2011;32(18):2247–2255. | |
Lehman R, Krumholz HM. Glycated haemoglobin below 7%. No to QOF target of less than 7%, again. BMJ. 2010;340:c985. | |
Czupryniak L. Guidelines for the management of type 2 diabetes: is ADA and EASD consensus more clinically relevant than the IDF recommendations? Diabetes Res Clin Pract. 2009;86 Suppl 1:S22–25. | |
Rydén L, Standl E, Bartnik M, et al. Guidelines on diabetes, pre-diabetes, and cardiovascular diseases: executive summary. The Task Force on Diabetes and Cardiovascular Diseases of the European Society of Cardiology (ESC) and of the European Association for the Study of Diabetes (EASD). Eur Heart J. 2007;28(1):88–136. | |
Jensen CE, Tuck SM, Agnew JE, et al. High prevalence of low bone mass in thalassaemia major. Br J Haematol. 1998;103(4):911–915. | |
Zanchetti A, Hansson L, Clement D, et al. Benefits and risks of more intensive blood pressure lowering in hypertensive patients of the HOT study with different risk profiles: does a J-shaped curve exist in smokers? J Hypertens. 2003;21(4):797–804. | |
Estacio RO, Jeffers BW, Gifford N, Schrier RW. Effect of blood pressure control on diabetic microvascular complications in patients with hypertension and type 2 diabetes. Diabetes Care. 2000;23 Suppl 2: B54–B64. | |
Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010; 362(17):1575–1585. | |
Patel A, Group AC, MacMahon S, et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. 2007;370(9590):829–840. | |
Cooper-DeHoff RM, Gong Y, Handberg EM, et al. Tight blood pressure control and cardiovascular outcomes among hypertensive patients with diabetes and coronary artery disease. JAMA. 2010;304(1):61–68. | |
Mancia G. Effects of intensive blood pressure control in the management of patients with type 2 diabetes mellitus in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Circulation. 2010; 122(8):847–849. | |
Gunarathne A, Patel JV, Gammon B, Gill PS, Hughes EA, Lip GY. Ischemic stroke in South Asians: a review of the epidemiology, pathophysiology, and ethnicity-related clinical features. Stroke. 2009;40(6):e415–e423. | |
Klonoff DC. United Kingdom prospective diabetes study follow-up studies establish a legacy effect of therapy for hyperglycemia but not hypertension. J Diabetes Sci Technol. 2008;2(6):922–924. | |
Moore LL, Visioni AJ, Wilson PW, D’Agostino RB, Finkle WD, Ellison RC. Can sustained weight loss in overweight individuals reduce the risk of diabetes mellitus? Epidemiology. 2000;11(3):269–273. | |
Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393–403. | |
Knowler WC, Fowler SE, Hamman RF, et al. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet. 2009;374(9702):1677–1686. | |
Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344(18):1343–1350. | |
Pan XR, Li GW, Hu YH, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care. 1997;20(4):537–544. | |
Gregg EW, Chen H, Wagenknecht LE, et al. Association of an intensive lifestyle intervention with remission of type 2 diabetes. JAMA. 2012; 308(23):2489–2496. | |
Wing RR, Bolin P, Brancati FL, et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369(2):145–154. | |
Connor H, Annan F, Bunn E, et al. The implementation of nutritional advice for people with diabetes. Diabet Med. 2003;20(10):786–807. | |
Andrews RC, Cooper AR, Montgomery AA, et al. Diet or diet plus physical activity versus usual care in patients with newly diagnosed type 2 diabetes: the Early ACTID randomised controlled trial. Lancet. 2011;378(9786):129–139. | |
Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336(16):1117–1124. | |
Liese AD, Nichols M, Sun X, D’Agostino RB Jr, Haffner SM. Adherence to the DASH diet is inversely associated with incidence of type 2 diabetes: the insulin resistance atherosclerosis study. Diabetes Care. 2009;32(8):1434–1436. | |
Estruch R, Ros E, Salas-Salvadó J, et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med. 2013;368(14):1279–1290. | |
Ajala O, English P, Pinkney J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. Am J Clin Nutr. 2013;97(3):505–516. | |
Carlström M, Larsen FJ, Nyström T, et al. Dietary inorganic nitrate reverses features of metabolic syndrome in endothelial nitric oxide synthase-deficient mice. Proc Natl Acad Sci U S A. 2010;107(41):17716–17720. | |
Lundberg JO, Carlström M, Larsen FJ, Weitzberg E. Roles of dietary inorganic nitrate in cardiovascular health and disease. Cardiovasc Res. 2011;89(3):525–532. | |
Ghosh SM, Kapil V, Fuentes-Calvo I, et al. Enhanced vasodilator activity of nitrite in hypertension: critical role for erythrocytic xanthine oxidoreductase and translational potential. Hypertension. 2013;61(5):1091–1102. | |
Chonchol M, Scragg R. 25-Hydroxyvitamin D, insulin resistance, and kidney function in the Third National Health and Nutrition Examination Survey. Kidney Int. 2007;71(2):134–139. | |
Pittas AG, Dawson-Hughes B, Li T, et al. Vitamin D and calcium intake in relation to type 2 diabetes in women. Diabetes Care. 2006;29(3):650–656. | |
Hypponen E, Power C. Vitamin D status and glucose homeostasis in the 1958 British birth cohort: the role of obesity. Diabetes Care. 2006;29(10):2244–2246. | |
Chiu KC, Chu A, Go VL, Saad MF. Hypovitaminosis D is associated with insulin resistance and beta cell dysfunction. Am J Clin Nutr. 2004;79(5):820–825. | |
Isaia G, Giorgino R, Adami S. High prevalence of hypovitaminosis D in female type 2 diabetic population. Diabetes Care. 2001;24(8):1496. | |
Mathieu C, Waer M, Laureys J, Rutgeerts O, Bouillon R. Prevention of autoimmune diabetes in NOD mice by 1,25 dihydroxyvitamin D3. Diabetologia. 1994;37(6):552–558. | |
D’Ambrosio D, Cippitelli M, Cocciolo MG, et al. Inhibition of IL-12 production by 1,25-dihydroxyvitamin D3. Involvement of NF-kappaB downregulation in transcriptional repression of the p40 gene. J Clin Invest. 1998;101(1):252–262. | |
van Halteren AG, van Etten E, de Jong EC, Bouillon R, Roep BO, Mathieu C. Redirection of human autoreactive T-cells upon interaction with dendritic cells modulated by TX527, an analog of 1,25 dihydroxyvitamin D(3). Diabetes. 2002;51(7):2119–2125. | |
Norman AW, Frankel JB, Heldt AM, Grodsky GM. Vitamin D deficiency inhibits pancreatic secretion of insulin. Science. 1980; 209(4458):823–825. | |
Zeitz U, Weber K, Soegiarto DW, Wolf E, Balling R, Erben RG. Impaired insulin secretory capacity in mice lacking a functional vitamin D receptor. FASEB J. 2003;17(3):509–511. | |
McCarty MF, Thomas CA. PTH excess may promote weight gain by impeding catecholamine-induced lipolysis – implications for the impact of calcium, vitamin D, and alcohol on body weight. Med Hypotheses. 2003;61(5–6):535–542. | |
Milner RD, Hales CN. The role of calcium and magnesium in insulin secretion from rabbit pancreas studied in vitro. Diabetologia. 1967;3(1):47–49. | |
Mitri J, Dawson-Hughes B, Hu FB, Pittas AG. Effects of vitamin D and calcium supplementation on pancreatic beta cell function, insulin sensitivity, and glycemia in adults at high risk of diabetes: the Calcium and Vitamin D for Diabetes Mellitus (CaDDM) randomized controlled trial. Am J Clin Nutr. 2011;94(2):486–494. | |
Pittas AG, Lau J, Hu FB, Dawson-Hughes B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2007;92(6):2017–2029. | |
Ford ES, Ajani UA, McGuire LC, Liu S. Concentrations of serum vitamin D and the metabolic syndrome among US adults. Diabetes Care. 2005;28(5):1228–1230. | |
Arunabh S, Pollack S, Yeh J, Aloia JF. Body fat content and 25-hydroxyvitamin D levels in healthy women. J Clin Endocrinol Metab. 2003;88(1):157–161. | |
Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr. 2000;72(3):690–693. | |
Pilz S, Tomaschitz A, Ritz E, Pieber TR. Vitamin D status and arterial hypertension: a systematic review. Nat Rev Cardiol. 2009;6(10):621–630. | |
Pfeifer M, Begerow B, Minne HW, Nachtigall D, Hansen C. Effects of a short-term vitamin D(3) and calcium supplementation on blood pressure and parathyroid hormone levels in elderly women. J Clin Endocrinol Metab. 2001;86(4):1633–1637. | |
Manson JE, Bassuk SS, Lee IM, et al. The VITamin D and OmegA-3 TriaL (VITAL): rationale and design of a large randomized controlled trial of vitamin D and marine omega-3 fatty acid supplements for the primary prevention of cancer and cardiovascular disease. Contemp Clin Trials. 2012;33(1):159–171. | |
Toplak H, Ziegler O, Keller U, et al. X-PERT: weight reduction with orlistat in obese subjects receiving a mildly or moderately reduced-energy diet: early response to treatment predicts weight maintenance. Diabetes Obes Metab. 2005;7(6):699–708. | |
Astrup A, Rossner S, Van Gaal L, et al. Effects of liraglutide in the treatment of obesity: a randomised, double-blind, placebo-controlled study. Lancet. 2009;374(9701):1606–1616. | |
Dicker D. DPP-4 inhibitors: impact on glycemic control and cardiovascular risk factors. Diabetes Care. 2011;34 Suppl 2:S276–S278. | |
Khavandi K, Brownrigg J, Hankir M, et al. Interrupting the natural history of diabetes mellitus: lifestyle, pharmacological and surgical strategies targeting disease progression. Curr Vasc Pharmacol. Epub January 20, 2012. | |
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724–1737. | |
Sjostrom L, Narbro K, Sjostrom CD, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357(8):741–752. | |
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122(3):248–256. e245. | |
le Roux CW, Aylwin SJ, Batterham RL, et al. Gut hormone profiles following bariatric surgery favor an anorectic state, facilitate weight loss, and improve metabolic parameters. Ann Surg. 2006;243(1):108–114. | |
Aghamohammadzadeh R, Greenstein AS, Yadav R, et al. Effects of bariatric surgery on human small artery function: evidence for reduction in perivascular adipocyte inflammation, and the restoration of normal anticontractile activity despite persistent obesity. J Am Coll Cardiol. 2013;62(2):128–135. | |
[No authors listed]. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):854–865. | |
[No authors listed]. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317(7160):703–713. | |
Hansson L, Zanchetti A, Carruthers SG, et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet. 1998;351(9118):1755–1762. | |
Williamson DF, Thompson TJ, Thun M, Flanders D, Pamuk E, Byers T. Intentional weight loss and mortality among overweight individuals with diabetes. Diabetes Care. 2000;23(10):1499–1504. |
 © 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.