")
Back to Journals » Patient Preference and Adherence » Volume 8
A qualitative study on hypertensive care behavior in primary health care settings in Malaysia
Authors Shima R, Farizah MH, Abdul Majid H
Received 19 June 2014
Accepted for publication 3 September 2014
Published 17 November 2014 Volume 2014:8 Pages 1597—1609
DOI https://doi.org/10.2147/PPA.S69680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Razatul Shima,1,3 Mohd Hairi Farizah,1,2 Hazreen Abdul Majid1,2
1Department of Social and Preventive Medicine; 2Centre for Population Health, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia; 3Ministry of Health Malaysia, Putrajaya, Malaysia
Purpose: The aim of this study was to explore patients’ experiences with their illnesses and the reasons which influenced them in not following hypertensive care recommendations (antihypertensive medication intake, physical activity, and diet changes) in primary health clinic settings.
Patients and methods: A qualitative methodology was applied. The data were gathered from in-depth interviews with 25 hypertensive patients attending follow-up in nine government primary health clinics in two districts (Hulu Langat and Klang) in the state of Selangor, Malaysia. The transcribed data were analyzed using thematic analysis.
Results: There was evidence of lack of patient self-empowerment and community support in Malaysian society. Most of the participants did not take their antihypertensive medication or change their physical activity and diet after diagnosis. There was an agreement between the patients and the health care professionals before starting the treatment recommendation, but there lacked further counseling and monitoring. Most of the reasons given for not taking antihypertensive medication, not doing physical activity and not following diet recommendations were due to side effects or fear of the side effects of antihypertensive medication, patients’ attitudes, lack of information from health care professionals and insufficient social support from their surrounding environment. We also observed the differences on these reasons for nonadherence among the three ethnic groups.
Conclusion: Health care professionals should move toward supporting adherence in the management of hypertensive patients by maintaining a dialogue. Patients need to be given time to enable them to overcome their inhibition of asking questions and to accept the recommendations. A self-management approach must be responsive to the needs of individuals, ethnicities, and communities.
Keywords: adherence, hypertension, in-depth interview, qualitative research
Introduction
Globally, many patients diagnosed with hypertension do not follow medical or lifestyle recommendations.1 There are many terminologies related to the definitions and the measurements of why patients do not take their prescribed medication and do not follow health recommendation, but the evidence converges on average at only 50%.1,2 The most widely used terms to describe patients’ behavior are compliance and adherence. The main difference is that adherence requires patients’ agreement to the recommendations from the health care provider.2 Most of the studies did not state if the patients’ previous agreement to the recommendations was taken into consideration. A study in Malaysia, which was done among hypertensive patients in a community health clinic in the state of Selangor found that the participants perceive prescribed Western medicine from the health clinic as scientifically proven but having undesirable side effects. Therefore, complementary and alternative medicine was used to counteract the harmful effects of the Western medicine. The types of adherence behavior found in the study include faithful follower, self-regulator, and intentional nonadherer.3 These behaviors pose a major concern in health care research, especially in the management of chronic conditions such as hypertension, where drug treatment and lifestyle changes are the principal management in preventing cardiovascular mortality and morbidity.2,4 Lack of conformance toward health care recommendations is associated with greater health care utilization, via cardiovascular-related hospitalizations and emergency department visits, which contribute to increases in total health care costs.5
It has been proposed that primary health care centers play a major role in providing care to hypertensive patients.6 Globally, the medication adherence rate was found to be low among primary care hypertensive patients.2 In Malaysia, 78.4% of known hypertensive patients claimed to be on oral antihypertensive medications, 82.7% were on specific diet, and 75.2% had been advised to be more physically active or to start exercising, whereby half of them received treatment at the government primary health clinics (53%).7 Nevertheless, good medication adherence rate among hypertensive patients treated at primary care facilities in Malaysia was only 53.4%.8
A study carried out in the outpatient hypertension clinic in Penang General Hospital, Malaysia revealed that 51.3% of hypertensive patients had poor adherence to antihypertensive medication, and a study conducted at the Family Medicine Clinic, University of Science in Kelantan, Malaysia had identified that 55.8% of hypertensive patients were noncompliant to their antihypertensive medication.9,10 It is important to recognize the reasons why hypertensive patients do not follow hypertensive care recommendations by their health care provider before implementing any intervention programs for hypertensive patients undergoing follow-up in primary health care facilities in Malaysia. Most studies done in Malaysia focus on quantitative measurements of the determinants of nonadherence.8–10 There was no exploration between ethnic differences in terms of the reasons for nonadherence and factors which influence the three major ethnic groups (Malay, Chinese and Indian) to adhere to health care recommendations. The research gap in this field is the absence of the patients’ perspective and a dearth of qualitative research, and there is lack of understanding of the way patients think and feel about their medications and their behavior.3,11 Qualitative research is a methodological approach that is often used to understand the experiences of a particular group or community because it allows flexible exploration of participants’ experiences.12 In addition, some of the qualitative research has identified important issues such as the quality of the doctor–patient relationship and patients’ health beliefs in a behavioral context toward health recommendations.13
Therefore, this study was initiated to explore hypertensive patients’ experiences with their illness and the reasons which influence them in not following hypertensive care recommendations (antihypertensive medication intake, physical activity, and diet changes) in those attending government primary health clinics follow-up. Hence, this study will provide better understanding of the reasons why hypertensive patients do not follow treatment and lifestyle changes recommendations in different ethnicities in Malaysia. It also provides essential information to health care providers, public health specialists, and policy makers for developing interventions which will consider all these barriers.
Materials and methods
A qualitative approach was adopted in this study, and the methodological schema of description-reduction-interpretation was used.14 Initial data collection was via in-depth interviews (description) with hypertensive patients who underwent follow-up at the chronic disease clinics of government primary health clinics in Hulu Langat and Klang districts, in the state of Selangor, Malaysia. This was followed by finding emerging themes (reduction) in the data and hermeneutic reflection (interpretation of results). The purpose of these interviews was to explore the patients’ experiences with their illnesses and to identify the reasons that influenced them in not following hypertensive care recommendations. In-depth interview was chosen as the method, as this approach yields more information regarding individuals’ complex beliefs than focusing on group discussions.15,16
Ethical approval was obtained from the Malaysian Ministry of Health (National Medical Research Register number 12-625-12500) and the University Malaya Medical Ethics Committee (number 914.5).
Study participants
The participants were both men and women diagnosed with hypertension, who went for follow-up at the chronic disease clinics in government primary health centers within the districts of Hulu Langat (Bangi, Semenyih, Beranang, Kajang, Batu 9, Bandar Seri Putra, and Sungai Chua health clinics) and Klang (Bandar Botanik, Bukit Kuda, Meru, Pandamaran, Port Klang, and Kapar health clinics) in the state of Selangor, Malaysia.
Purposive sampling was adopted to select different age groups and different ethnic groups to represent the major ethnic groups in Malaysia: Malays, Chinese, and Indians. Two doctors in each health clinic were involved in selecting the hypertensive patients who did not follow medication or change their lifestyles, as perceived by the doctors.
The inclusion criteria were patients diagnosed with essential hypertension for at least 6 months, Malaysian nationality, aged above 18 years, able to read and understand English or Bahasa Malaysia, and without physical disabilities which would limit them from undertaking physical activity recommendations. Table 1 shows the characteristics of the 25 participants involved in this study.
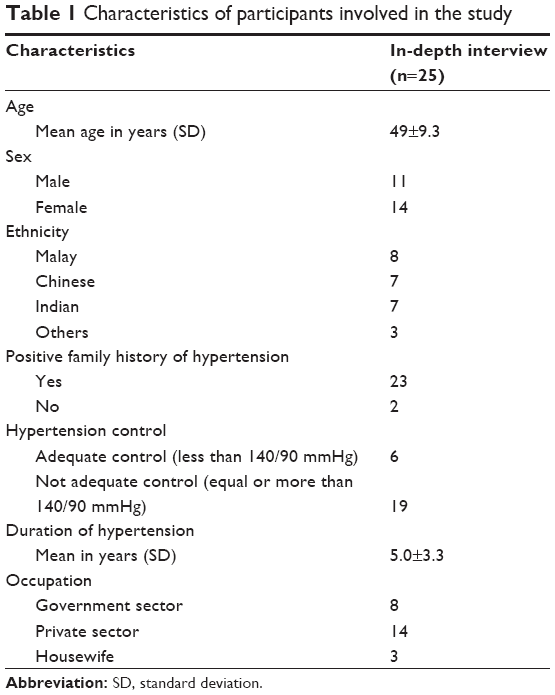 | Table 1 Characteristics of participants involved in the study |
Study instruments
A rough interview guide was developed from the literature review as a reminder of areas to be covered during the interviews (Table S1). The interview guide was developed in English and was translated into Malay. This interview guide was discussed among the research team, and the contents were evaluated by experts (three family medicine specialists, one internal medicine specialist, and two public health specialists). Also, the interview guides were pretested with eight hypertensive patients for their relevance, suitability, and ease to carry out in primary health care settings. The research questions were designed with open-ended questions. Probes, such as “Would you explain that further?”, “Would you give me an example?”, “Is there anything else?” were used throughout the interview to encourage the interviewees to converse. Each interview began with the same opening question: “How did you first discover you have hypertension?” This gave the participants the chance to narrate their flow of thoughts on the topic.
Study procedures
The participants were selected from government primary health clinics, which serve the lower socioeconomic strata to affluent middle class strata. Between March 2013 and the end of July 2013, the hypertensive patients who were selected by their doctors were approached while waiting for their appointments at the chronic disease clinics. They were approached accompanied by the staff nurse in charge after their blood pressure readings were taken at the screening counter. An information sheet on the study and informed consent form were given. The in-depth interviews were all done face to face in an isolated room in the health clinic after the patients had seen their doctors and had taken their medicines in the pharmacy. The confidentiality of the interviews was ensured. Only the interviewer and the interviewee were present to ensure that the participants’ answers were exclusive. All the interviews were conducted in both English and Bahasa Malaysia by the primary investigator, with each interview lasting between 45 and 90 minutes.
A demographic questionnaire was also administered verbally at the beginning of the interview. All the interviews were audio taped. First member checking was done as validation to confirm the information given by each participant. The final sample size reflected continuous sampling until saturation with no new issues or ideas emerging from the participants. Participants’ case notes reviews were done in order to verify the personal information and the blood pressure reading. Five patients were not keen to be interviewed because they claimed that they followed the treatment and lifestyle recommendations from their doctors. Thus, 25 participants were interviewed.
Data analysis
The data from the in-depth interviews were transcribed verbatim. Data were analyzed by the primary investigator (SR) using thematic analysis. The transcriptions were stored and managed accordingly to ensure confidentiality. Second member checking was done as each participant received a copy of the interview transcript for them to review to check for narrative accuracy. The NVivo 9 software from QSR International (the Melbourne-based software developer specializing in qualitative research software) was used for the analysis to assist and to facilitate the coding processes, and further categorization was done to make sense of the essential meanings of the phenomenon and to allow the emergence of the common themes. The primary investigator and a public health specialist who has experience in research generated different initial coding schemes, and the differences were resolved via discussion.
The finalized transcripts were then translated into English by another independent translator. The first author then read the transcripts line by line, repeatedly and thematically, to analyze the contents. In order to draw in-depth views, the participants were given the freedom to express additional reviews and comments. The interviews mainly focused on the experiences with antihypertensive medication and the reasons for not following the hypertensive care recommendations (antihypertensive medication, physical activity, and diet recommendations).
Results
From the analysis of responses, this study was able to identify four themes: a) symptoms of hypertension at first diagnosis, b) barriers and facilitators of hypertensive care nonadherence with antihypertensive medication, c) barriers and facilitators of hypertensive care nonadherence with physical activity and diet, and d) issues with health care professionals and health care system.
Symptoms of hypertension at first diagnosis
The participants in this study generally experienced symptoms at first diagnosis, such as dizziness and headaches. They reported that they had difficulty in sleeping due to stress and overwork prior to the diagnosis. Six participants expressed that they had stress due to workload at home. Most of the participants also seemed to regard stress and blood pressure as synonymous.
Only six of the 25 participants were first diagnosed during a routine medical screening, whereas others were diagnosed when they sought medical attention for their symptoms. Several patient comments are shown below:
I have to reason with my new boss. I could not sleep and started having headaches. When I went and checked, I still remember, the upper reading was 160. The doctor asked me to take medication but I don’t want to because I don’t think I need this medication. I’ve tried controlling my stress, but my blood pressure is still high. [in-depth interview (IDI)/43 years-old/6 years diagnosed with hypertension]
I’ve got headaches, but I don’t know it was high blood pressure. I have to take care of my husband who is suffering from stroke. I’ve overworked and can you imagine how stressful I am? That’s why my blood pressure shot up. I know if I don’t take my medication, I can be just like my husband. [IDI/65 years-old/1 year diagnosed with hypertension]
I experienced dizziness on and off because I don’t have enough rest and sleep. I work and continue working without sleeping. I have no time to rest and I feel so stressed. That’s why I’m suffering from high blood pressure. [IDI/50 years-old/8 years diagnosed with hypertension]
I have blood pressure set at home. My son bought it for me, but I don’t check my blood pressure regularly until at one time I had a really bad headache and I noticed my pressure shot up. [IDI/61 years-old/2 years diagnosed with hypertension].
Barriers and facilitators of hypertensive care nonadherence to antihypertensive medication
Eighteen participants admitted not taking their antihypertensive medication as prescribed. Despite being unsuccessful, they believed that they could control their blood pressure through physical activity, diet, and stress management, hence, medication was not necessary. Twenty one participants stated that their doctor did ask for their agreement to start the antihypertensive medication. However, they sometimes did not take the medication without informing their doctor. Three of them did not consider taking medication as a priority. Fifteen participants expressed their nonchalant attitude, even though they were aware of the complications of hypertension, such as stroke and heart disease.
Most of the reasons for nonadherence to antihypertensive medication were comprised of attitudes of the patients themselves, namely, forgetfulness, perceived side effects of the medications such as dehydration, loss of interest in sex, tire easily, palpitations, feeling hot, and sweating. Sixteen participants were afraid of the side effects of antihypertensive medication. Four participants were also afraid of becoming too dependent on medication and believed that taking medication could damage their body. Most of the reasons given were due to the side effects of the medication and not due to the availability issues. Moreover, two participants took alternative treatments, such as traditional medicine.
Eleven participants were encouraged or influenced not to take the medications by others, especially family members. Ten participants, however, did get support and motivation to take their antihypertensive medication from their family members, whereas four participants motivated themselves and were encouraged by their families. It was noted that there were differences in reasons and facilitators which influence them for nonadherence among the ethnicities. Malay patients tend to find alternative treatments other than medication recommended by their doctors. Indian patients were more influenced by people surrounding them, especially their families (spouse, mother-in-law) and peers (neighbors, friends), in their decision making toward medication adherence. Whereas, Chinese patients preferred simple medication dosage because they tend to forget their medication due to their busy schedule. These concepts are described in the following patient comments:
I did not take my medication yesterday and today because I’m on leave. I left my medication at workplace. Taking medication is not a priority in my daily routine. [IDI/49 years-old/12 years diagnosed with hypertension]
I feel dry when I take blood pressure medication. I find it so difficult because I always have to remember to take it every day. I feel like I have lost sexual desire after taking the medication. All my children have advised me to seek alternative medicine first because they don’t want me to be too dependent on medication. [IDI/58 years-old/3 years diagnosed with hypertension]
The doctor did asked my agreement before starting medication. But I didn’t take my medication because I took alternative medication. My sexual life changed after I took the antihypertensive medication. I got tired easily and had no mood. I also experienced heatiness, palpitations, and sweating with the medication. I’m afraid that my husband and my mother in law know I’m taking antihypertensive medication. They said that I’m still young and need not any medication yet. My neighbor also told me that medication can cause damages to our body. [IDI/31 years-old/5 years diagnosed with hypertension]
I sometimes miss my medication because I have to take it twice daily. I prefer daily dosage of medication. I always forget to take my medicine due to my busy schedule. I haven’t discuss this matter with the doctor yet, but I will tell him during the next appointment. [IDI/48 years-old/7 years diagnosed with hypertension].
Barriers and facilitators of hypertensive care nonadherence with physical activity and diet
Three participants were unaware of the importance of exercise and diet in managing their blood pressure. Seventeen participants found it difficult to change their lifestyle after being diagnosed. Only three participants said that they exercised regularly and changed their diet according to the doctor’s advice. Eight participants felt that it was unsafe for them to exercise or to walk outside their houses. Thirteen participants were not involved in any health-promoting activities, such as the healthy lifestyle campaign in their community, as they were unaware of such activities in their community. Participants claimed that they were busy with their work and daily life commitments, whereas the others were aware of the activities, but they claimed that they were too busy to get involved. Two participants had exercise facilities at home, but the patients neither had time nor self-motivation to use them.
Most participants had difficulty in controlling their diet due to the widespread availability of food in Malaysia. While at work, eight participants expressed their preference to eat out rather than bring their own healthy meals. Salty and oily foods were still prepared at home and were served to the whole family, even though the family members were aware of the participant’s high blood pressure. A common reason given for not following a low salt and low fat diet was the lack of support from family and peers to enable them to resist eating tasty foods high in salt and fats rather than less tasty low salt and low fat options. Some patient comments regarding these barriers were as follows:
I’ve got no time to exercise although I have a treadmill at home. I just eat whatever I want to eat. I eat salted fish every day and if taken a lot, I notice my blood pressure will hike. My wife still cooks food high in salt and fats although she knows I have hypertension. [IDI/63 years-old/4 years diagnosed with hypertension]
I don’t care and there’s no point in controlling because I have already got the disease. [IDI/31 years-old/5 years diagnosed with hypertension]
I go for exercise once a month but I find it so difficult to control my food because delicious food in Malaysia is everywhere and I want to eat everything. I just bought food outside although I know that food from outside is unhealthy. [IDI/49 years-old/12 years diagnosed with hypertension]
I am unaware of any activities going on in my neighborhood. Nowadays is not like before because nobody talks to their neighbors. I just go to church and watch television at home. I’m afraid to go for a jog alone. [IDI/62 years-old/1 year diagnosed with hypertension]
I was invited a few times by the staff nurse in charge to join aerobic class handled by the community but I’ve got no time. I know some of my friends with hypertension have joined the aerobic class twice a week. They also have it once a week during the weekend outside the mosque in my neighborhood. [IDI/59 years-old/12 years diagnosed with hypertension].
Issues with health care professionals and the health care system
Fifteen participants expressed their feelings that the doctor’s consultation time with them was too short after hours of waiting in the queue. Nineteen felt that the doctor should spend more time to explain the side effects of the medication and how to exercise and control their diet. Only five participants said that their doctor informed them that they might experience some side effects at the time of the initial diagnosis. With regard to information on dietary measures, thirteen participants claimed that they were referred once to a dietitian for diet counseling after being diagnosed with hypertension, but no follow-up or further management was done. In terms of health care service delivery, they preferred the same doctors and nurses to routinely manage their hypertensive clinic follow-up. The participants also found that the nurses were friendlier and were able to spend more time with the patients than other members of the health care staff. Three participants were uncomfortable talking about the health care service and refused to give their comments.
Finally, six participants were unsure if the resource center was available for chronic diseases in their respective health clinics. Every health clinic has a resource center, which provides counseling and educational materials for patients with chronic diseases attending follow-up. The counseling methods involve educational class discussion within a small group of patients, individual counseling, and healthy food cooking demonstration. Some patient comments regarding the health care system are,
I do not quite understand what the doctor says every time I go for my follow-up. The doctor just says that I have high blood pressure. I have to take the medication and control my diet. He does not explain that high blood pressure is dangerous and what would happen in the future if I do not take my medication. My children are still small. So, if the doctor doesn’t care about me, why must I care about myself? [IDI/31 years-old/5 years diagnosed with hypertension]
don’t share my problem regarding taking medication with the doctor. They usually say a few words “Okay, just take your medication and you can go now.” It’s not even five minutes compared to the long time spent for waiting. The nurses usually spend their time talking to the patients. I always talk to the nurse who usually takes my blood pressure outside the consultation room. She advises me a lot. She told me the correct way of taking meals. [IDI/43 years-old/6 years diagnosed with hypertension]
The doctor told me that I might experience some side effects with this antihypertensive medication, such as headaches, stomach upsets, and others. But he didn’t tell me how to handle the side effects. [IDI/49 years-old/7 years diagnosed with hypertension]
Pharmacist in this health clinic will explain regarding the dosage and frequency of the medication. Sometimes they also explain the side effects of the medication if I ask them. But I need more information from the doctor regarding the side effects and how to deal with it. If I have the time, I will surf the internet. [IDI/56 years-old/10 years diagnosed with hypertension]
I’m not sure about the resource center. I’ve been referred to a dietitian once after the doctor discovered I have hypertension, but there’s no follow-up. [IDI/39 years-old/9 years diagnosed with hypertension].
Discussion
This study showed that there was evidence of an agreement between the participants interviewed and their doctors before starting the health care recommendations. However, it later resulted in partial adherence due to poor monitoring and counseling from their health care professionals. Most of the participants admitted not taking their antihypertensive medication as prescribed by their doctor although they agreed with the treatment recommendations earlier. The participants also had poor self-management and low self-efficacy in adherence to their hypertensive care. Consistent with previous studies conducted in other developing countries17,18 and developed countries,19,20 this was partly attributed to lack of awareness of self-care and the importance of health screening. Most participants only had their blood pressure assessed during visits to their doctors or to the pharmacy. Only two participants had a blood pressure set at home, yet even they did not use it to regularly monitor their blood pressure. A qualitative study done in Malaysia found that patients who self-monitored were eager to be more involved in discussions about their blood pressure control.21 Similar findings were also reported in a qualitative study looking at primary care patients’ experiences of home blood pressure measurement in the United Kingdom and Japan.22,23 Therefore, wherever feasible, patients should be taught to measure and monitor their own blood pressure and to assess their own adherence.
The participants’ lifestyles also remained the same after being diagnosed with hypertension. However, they claimed to have tried to lower their blood pressure by changing their lifestyle. However, their attempts have clearly failed. The participants in this study wanted to know more about how to control their diet and how to exercise correctly. However, accurate information was not given at screening and during follow-up. Seven participants stated that they were not referred to other health care providers, such as dietitian or staff nurse in charge in the resource center for counseling regarding their lifestyle changes. There is a need for dietitian referral because if the participants knew what food to eat, they might succeed in controlling their diet. Most of the participants were unaware of the existence of the resource center in the health clinics, where they can get information regarding hypertension from counseling, flyers, healthy cooking demonstration. As a result, the participants were uncertain what they should do. A study in Malaysia reported that three quarters of the subjects had unsatisfactory hypertensive control and it was related to food intake and eating habits, including high salt diet.24
Moreover, a study showed that knowledge by itself may not impact adherence.25 However, knowledge has been shown to enhance behavior changes, but to a limited extent.26 Health care providers should give patients enough education about the treatment and disease. Health visits should include realistic assessment of patients’ knowledge and understanding of their medication regimen, clear and effective communication between health professionals and their patients, and efforts to build trust in the therapeutic relationship.27 Participants needed more information regarding side effects and long-term effects of medications that they were taking. This study revealed that the pharmacist have an important role in giving information related to missed doses, adverse effects, and patient understanding of medication regimen.
However, there was evidence that lack of communication still exists between patients and health care providers with regard to medications, especially on their use and side effects. Participants need to understand the importance of maintaining blood pressure and to take their drugs routinely. Furthermore, they need to learn how to deal with missed doses, how to identify adverse events, and what to do when that occur. Participants also preferred simple daily dosing. A study showed that reducing the number of daily doses appeared to be effective in increasing adherence to antihypertensive medication intake and should be tried as a first-line strategy.28
Among the many reasons given for not adhering to medication and other hypertensive care, most were due to patients’ attitudes and not due to health service availability issues. Although the participants’ health visit duration had been long, and they had to wait more than 3 hours outside the consultation room to see the doctor, this did not affect their satisfaction with the overall services at the clinic. The participants also did not have problems with the accessibility and affordability with their antihypertensive medication. This finding is consistent with another study done in Malaysia.29 There were 1,025 government health clinics in Malaysia as of December 31, 2012,30,31 and these clinics are highly subsidized by the Malaysian government, including the medications and treatments.31 However, this may not be applied to other patient populations; hence, other studies found that patients who were without insurance coverage or who had low income were more likely to be nonadherent to their treatment.32
Patients must be given the opportunity to relate their experiences with hypertension during the follow-up. This may allow the health professionals to understand the crucial elements of patients’ adherence, such as their beliefs, attitudes, subjective norms, cultural context, social supports, and emotional problems. For example, most of the participants interviewed experienced stress before they were diagnosed as hypertensive. Therefore, it is important to recognize that such patients need to have early referrals for counseling and aid from psychologists to reduce the stress before it becomes worse. A study by Crowley et al found that high stress was associated with medication nonadherence among hypertensive patients from primary health clinics.33
There was a wide variety of reasons why patients did not adhere to their antihypertensive medications, diet, and exercise. These study findings suggest that adhering to each of these behaviors posed different challenges for the participants. Family members played an important role and may also pose barriers in motivating participants to take their medications compared to friends, neighbors, and others. This study found that family members discouraged some patients from taking antihypertensive medication or resisted dietary changes, such as cooking the same high salt foods. Studies showed family support was associated with better adherence.34–37
This study identified aspects of patients’ beliefs and behaviors regarding antihypertensive medications and their lifestyle change after being diagnosed as hypertensive. Most patients demonstrated that they accepted responsibility for the management of their hypertension, but some were unwilling to make decisions for themselves. The responsibility for adherence must be shared between the patient, health care provider, and community. Mutual collaboration between the patients and their health care providers fosters greater patient satisfaction, reduces the risks of nonadherence, and improves patients’ health care outcomes.38 Community mobilization is needed in terms of advocacy to empower patients to adhere to their hypertensive care and to create positive advocating environments.
Community resources to empower this group of patients should be established in community settings, such as in mosques and churches, as a starting point for patients to develop self-care and create peer support groups. Social support received by patients from other members of their community has been consistently reported as an important factor that affected health outcomes and improved adherence.39 Social support groups are needed to promote the exchange of experiences in dealing with hypertension, its care, and to promote patients’ responsibility for their own care. There is evidence that peer support groups among patients were able to improve adherence to therapy, while reducing the amount of time devoted by health care professionals for chronic disease management.40
Implications for further research and clinical practice
This study discovered that there were differences between ethnicities in reasons and facilitators for nonadherence which influenced the participants. Future qualitative study should be done to further explore the reasons and facilitators which influence the hypertensive patients in each ethnicity in Malaysia.
By conducting these qualitative interviews, items for the reasons of nonadherence or noncompliance can be generated for development within a clinically meaningful scale. This scale may have the greatest importance in developing countries, such as Malaysia, because the information derived from the self-administered health questionnaires is comprehensive, practical, and inexpensive.
A further study among hypertensive patients from private clinics could be included for comparison to better reflect the needs and preferences of hypertensive patients to improve clinical management and public health intervention.
Different tools have been used to evaluate and to assess patient adherence to medication, but there is no single measurement of patient adherence to medications that can be referred to as the “gold standard.” The most commonly and widely used self-reporting measures of medication adherence for hypertension are the Morisky Medication Adherence Scale and the Hill-Bone Compliance to Medication Scale.41,42 The Morisky Medication Adherence Scale classified nonadherence as intentional and unintentional factors related to forgetfulness, carelessness, and stopping medications when feeling better or worse. The Hill-Bone Compliance to Medication Scale addressed barriers and self-efficacy of patients’ in taking their medications. However, in addition to these two scales, the literature has reported other important reasons why individuals are nonadherent to their antihypertensive medications. To this date, the measure of nonadherence is yet to be comprehensive. Furthermore, a study showed that the use of both scales cannot be recommended because their ability to identify medication adherence was essentially by chance, with inconsistency for nearly every third hypertensive patient.43
Limitations
All the interviews were done in government primary health care clinics, and this may affect the participants’ responses. Further exploration by interviewing family members and health care providers would be useful for a better understanding of the problem.
Conclusion
In conclusion, understanding patients’ need and lack of shared decision making seem to be the major adherence barriers faced by hypertensive patients in this study. Therefore, the responsibility for nonadherence has to be shared by the patients, health professionals, the health care system, and the community. Also, community resources should be established. Self-management approach must be responsive to the needs of individuals, communities, and populations, recognizing that the provision of information or resources alone does not mean that people can or will access and use them. Within the limitations, our findings can help doctors who seek to understand their patients’ thinking regarding their antihypertensive medication at the start or review of the course of drugs. They can contribute to discussions on the advantages of drugs in a way that is relevant for patients personally, in support of decisions that are concordant between patients and doctors.
The widespread preference of people to seek alternative and complementary medicines must be acknowledged, and patients need to be encouraged to adopt approaches that are personally relevant, but supported by scientific evidence. Community resources should be established to act as peer support groups to improve patients’ self-efficacy in order to empower them to adhere to their antihypertensive care.
Acknowledgments
We would like to thank the Malaysian Director General of Health for granting us the permission to publish this study. We would like to extend our gratitude to the doctors, to the patients who participated in the in-depth interviews, and the staff members involved at the chronic disease clinics in the primary health clinics during data collection. This study is supported by the research grant from the Ministry of Education and University of Malaya, grant number FL 009/2011.
Disclosure
Researcher time was paid by the Ministry of Health fellowship. The authors report no conflicts of interest in this work.
References
Lüscher TF, Vetter H, Siegenthaler W, Vetter W. Compliance in hypertension: facts and concepts. J Hypertens Suppl. 1985;3(1):S3–S9. | ||
World Health Organization. Adherence to long-term therapies: evidence for action. Geneva: World Health Organization; 2003. Available from: whqlibdoc.who.int/publications/2003/9241545992.pdf | ||
Lee K, Halimatun HM, Steven EK, Ong BK. Understanding the perception concerning medication and types of adherence behaviour in hypertensive patients. Pertanika J Soc Sci Hum. 2012;20(3):781–796. | ||
Wong MC, Tam WW, Cheung CS, et al. Drug adherence and the incidence of coronary heart disease- and stroke-specific mortality among 218,047 patients newly prescribed an antihypertensive medication: a five-year cohort study. Int J Cardiol. 2013;168(2):928–933. | ||
Pittman DG, Tao Z, Chen W, Stettin GD. Antihypertensive medication adherence and subsequent healthcare utilization and costs. Am J Manag Care. 2010;16(8):568–576. | ||
Al-Mustafa BA, Abulrahi HA. The role of primary health care centers in managing hypertension. How far are they involved? Saudi Med J. 2003;24(5):460–465. | ||
Ministry of Health. National Health and Morbidity Survey IV. Vol II. Kuala Lumpur: Ministry of Health; 2011. | ||
Ramli A, Ahmad NS, Paraidathathu T. Medication adherence among hypertensive patients of primary health clinics in Malaysia. Patient Prefer Adherence. 2012;6:613–622. | ||
Turki AK, Sulaiman SAS. Adherence to antihypertensive therapy among patients in Penang General Hospital using structural equation modelling (SEM). Int J Pharm Pharm Sci. 2010;2(1):24–32. | ||
Hassan NB, Hasanah CI, Foong K, et al. Identification of psychosocial factors of noncompliance in hypertensive patients. J Hum Hypertens. 2006;20(1):23–29. | ||
Khuan L, Siew CY, Rahman HA, Yee LY. From compliance to adherence and concordance, what quantitative and qualitative studies have synthesized? J Health Management. 2008;4(1):36–61. | ||
Berg BL. Qualitative Research Methods for the Social Sciences. 4th ed. Boston: Allyn and Bacon; 2001. | ||
Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three decades of research. A comprehensive review. J Clin Pharm Ther. 2001;26(5):331–342. | ||
Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook. Thousand Oaks, CA: Sage; 1994. | ||
Ulin PR, Robinson ET, Tolley EE. Qualitative Methods in Public Health: A Field Guide for Applied Research. San Francisco, CA: Jossey-Bass; 2004. | ||
Kuper A, Reeves S, Levinson W. Qualitative research: An introduction to reading and appraising qualitative research. BMJ: British Medical Journal. 2008:404–407. | ||
Saleem F, Hassali M, Shafie A, Atif M. Drug attitude and adherence: a qualitative insight of patients with hypertension. J Young Pharm. 2012;4(2):101–107. | ||
Dennis T, Meera NK, Binny K, Sekhar MS, Kishore G, Sasidharan S. Medication adherence and associated barriers in hypertension management in India. CVD Prev Control. 2011;6(1):9–13. | ||
Lau E, Kaczorowski J, Karwalajtys T, Dolovich L, Levine M, Chambers L. Blood pressure awareness and self-monitoring practices among primary care elderly patients. Can Pharm J. 2006;139(6):34–41. | ||
Knight EL, Bohn RL, Wang PS, Glynn RJ, Mogun H, Avorn J. Predictors of uncontrolled hypertension in ambulatory patients. Hypertension. 2001;38(4):809–814. | ||
Abdullah A, Othman S. The influence of self-owned home blood pressure monitoring (HBPM) on primary care patients with hypertension: a qualitative study. BMC Fam Pract. 2011;12:143. | ||
Rickerby J, Woodward J. Patients’ experiences and opinions of home blood pressure measurement. J Hum Hypertens. 2003;17(7):495–503. | ||
Saito I, Nomura M, Hirose H, Kawabe H. Use of home blood pressure monitoring and exercise, diet and medication compliance in Japan. Clin Exp Hypertens. 2010;32(4):210–213. | ||
Suzana S, Azlinda A, Hin SL, et al. Influence of food intake and eating habits on hypertension control among outpatients at a government health clinic in the Klang Valley, Malaysia. Malays J Nutr. 2011;17(2):163–173. | ||
Jolles EP, Padwal RS, Clark AM, Braam B. A qualitative study of patient perspectives about hypertension. ISRN Hypertension. 2013;2013:1–10. | ||
Mooney LA, Franks AM. Impact of health screening and education on knowledge of coronary heart disease risk factors. J Am Pharm Assoc. 2003;51(6):713–718. | ||
Brownstein JN, Chowdhury FM, Norris SL, et al. Effectiveness of community health workers in the care of people with hypertension. Am J Prev Med. 2007;32(5):435–447. | ||
Domino FJ. Improving adherence to treatment for hypertension. Am Fam Physician. 2005;71(11):2089–2090. | ||
Aziz AM, Ibrahim MI. Medication noncompliance – a thriving problem. Med J Malaysia. 1999;54(2):192–199. | ||
Lee ES, Forthofer RN. Analyzing Complex Survey Data. 6th ed. Thousand Oaks, CA: Sage; 2006. | ||
Official Portal Ministry of Health Malaysia [homepage on the Internet]. Putrajaya: Ministry of Health Malaysia. Available from: http://www.moh.gov.my/english.php. Accessed 21 July, 2013. | ||
Briesacher BA, Gurwitz JH, Soumerai SB. Patients at-risk for cost-related medication nonadherence: a review of the literature. J Gen Intern Med. 2007;22(6):864–871. | ||
Crowley MJ, Grubber JM, Olsen MK, Bosworth HB. Factors associated with non-adherence to three hypertension self-management behaviors: preliminary data for a new instrument. J Gen Intern Med. 2013;28(1):99–106. | ||
Wilson DK, Ampey-Thornhill G. The role of gender and family support on dietary compliance in an African American adolescent hypertension prevention study. Ann Behav Med. 2001;23(1):59–67. | ||
Morisky DE, DeMuth NM, Field-Fass M, Green LW, Levine DM. Evaluation of family health education to build social support for long-term control of high blood pressure. Health Educ Q. 1985;12(1):35–50. | ||
Kirscht JP, Rosenstock IM. Patient adherence to antihypertensive medical regimens. J Community Health. 1977;3(2):115–124. | ||
Eng E, Hatch J, Callan A. Institutionalizing social support through the church and into the community. Health Educ Q. 1985;12(1):81–92. | ||
Martin LR, Williams SL, Haskard KB, DiMatteo MR. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1(3):189–199. | ||
DiMatteo MR. Social support and patient adherence to medical treatment: a meta-analysis. Health Psychol. 2004;23(2):207–218. | ||
Tehrani AM, Farajzadegan Z, Rajabi FM, Zamani AR. Belonging to a peer support group enhance the quality of life and adherence rate in patients affected by breast cancer: A non-randomized controlled clinical trial. J Res Med Sci. 2011;16(5):658–665. | ||
Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. | ||
Kim MT, Hill MN, Bone LR, Levine DM. Development and testing of the Hill-Bone Compliance to High Blood Pressure Therapy Scale. Prog Cardiovasc Nurs. 2000;15(3):90–96. | ||
Koschack J, Marx G, Schnak enberg J, Kochen MM, Himmel W. Comparison of two self-rating instruments for medication adherence assessment in hypertension revealed insufficient psychometric properties. J Clin Epidemiol. 2010;63(3):299–306. |
Supplementary material
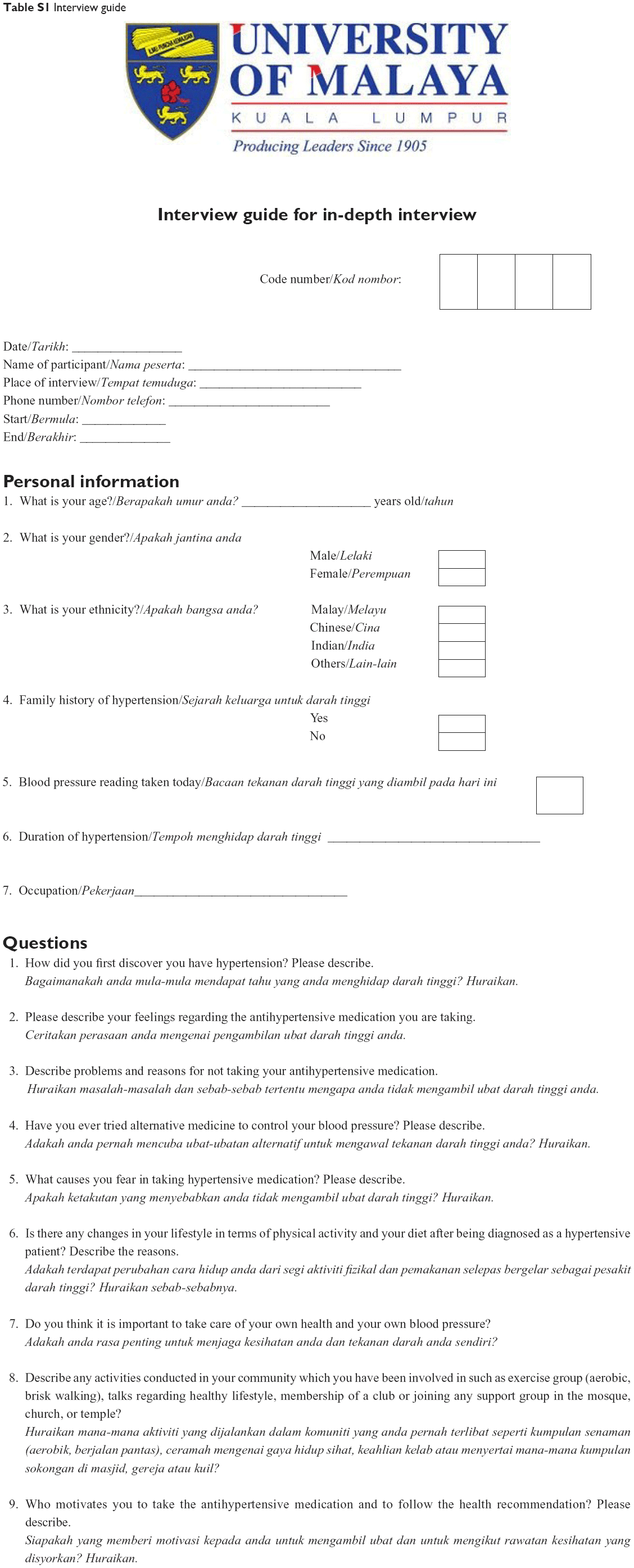 | Table S1 Interview guide |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.