")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
A cross-sectional study on perception of stigma by Chinese schizophrenia patients
Authors Ren Z, Wang H, Feng B, Gu C, Ma Y, Chen H, Li B, Liu L
Received 6 September 2013
Accepted for publication 15 October 2013
Published 26 March 2014 Volume 2014:10 Pages 535—540
DOI https://doi.org/10.2147/NDT.S54115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Zhibin Ren, Heqiu Wang, Bin Feng, Chenyu Gu, Yongchun Ma, Hong Chen, Bingling Li, Lanying Liu
Department of Psychiatry, Tongde Hospital, Zhejiang Chinese Medical University, Hangzhou, People's Republic of China
Objective: In this cross-sectional study, we sought to assess the extent of internalized stigma among inpatients and outpatients with schizophrenia in the People's Republic of China and to investigate whether education level correlated with the experience of stigma.
Methods: Schizophrenia patients were evaluated using the Brief Psychiatric Rating Scale (BPRS), the Positive and Negative Syndrome Scale (PANSS), the Clinical Global Impressions-Severity of Illness (CGI-S) scale and the Stigma Scale for Mental Illness (SSMI-C). Patients were categorized into high education and low education groups, according to their educational levels.
Results: One hundred thirty-three subjects were included in the study. Their mean course of illness was 4.32±6.14 years (range: 1 month to 15 years). Their mean BPRS score was 19.87±5.46, their mean PANSS score was 44.11±13.1, and their mean CGI-S score was 2.22±0.81. In addition, their mean SSMI-C score was 6.49±0.9. The mean SSMI-C score of patients who have received high school education or above was 7.15±0.98, which was markedly higher than that of patients who have received middle school education or below, which was 5.75±0.79 (P<0.05). Before the study most patients (92.5%, 123/133) took atypical drugs.
Conclusion: Education level impacts on the perception of stigma by schizophrenia patients, and more psychoeducation should be undertaken to improve patients' knowledge about schizophrenia.
Keywords: schizophrenia, stigma, Brief Psychiatric Rating Scale (BPRS), Positive and Negative Syndrome Scale (PANSS), Clinical Global Impression-Severity (CGI-S) scale, Stigma Scale for Mental Illness (SSMI-C)
An Expression of concern has been published for this paper
Retraction has also been published
Introduction
Schizophrenia is a chronic illness that carries a heavy burden for society, families, and individual patients. Stigma is well established as an added burden for people with schizophrenia.1 Stigma is a major problem across different societies, but the particular manifestations of stigma may vary due to apparent or subtle differences in socially or culturally accepted norms of behavior imposed on individual patients. Currently, two major types of stigma are recognized: public or social stigma, and personal stigma. Personal stigma can be 1) perceived stigma, which is what an individual patient thinks society’s beliefs are about the stigmatized patient; 2) experienced stigma, which is actual discrimination an individual patient has experienced; and 3) self-stigma, a product of the internalization of public stigma. In internalized stigma, or self-stigma, an individual patient gradually assimilates public stereotypes of mental illness to such a degree that the patient progressively loses perception of their self, which ultimately leads to changes in his or her behavior in a way that is consistent with the internalized perceptions.2 Thorough investigation of the extent and correlates of internalized stigma is essential to planning recovery programs for schizophrenia patients.
Stigma toward schizophrenia patients in Chinese societies is pervasive, frequently resulting in internalization of these negative conceptions and loss of self-esteem. Chen et al3 interviewed the family members of 72 patients with severe mental illness using the Family Stigma Interview (FSI) and found that stigma was pervasive among family members, especially if they had received high school or further education. In 2005, Gao et al4 surveyed 225 convalescent schizophrenic patients and their family members at three specialty hospitals in Beijing, People’s Republic of China. They found that 42% of the patients experienced unfair treatment at jobs and 56% of their family members hid the illness from others to avoid discrimination. Huang, at Shanghai Changning District Mental Hospital in Shanghai, People’s Republic of China, studied 209 mentally ill patients hospitalized for >12 months and found that stigma was pervasive.5 Phillips et al6 interviewed 1,491 schizophrenic patients in five mental illness institutions between 1990 and 2000 using the Camberwell Family Interview (CFI), finding that 60% of patients and their family members felt moderate impact on their life because of stigma.
There has been growing interest in stigma in schizophrenic patients, including the etiology of stigma, the self-perception of schizophrenic patients, and impact of stigma on schizophrenic patients and their families. Most of our understanding about internalized stigma in schizophrenia patients, however, comes from studies in Western countries. The studies on outpatients with schizophrenia by Ritsher and Phelan7 and Sartorius8 found that stigma was present in these patients during convalescence. Prince and Prince9 also found that a majority (73.2%) of mentally ill patients had self-derogation and felt discriminated against. Ritsher and Phelan followed up 82 outpatients with mental illnesses for 4 months and found that one-third of the patients had high levels of self-stigma, which means that they may have met the criteria for depression, and that two-fifths of the patients reported social regression, while only one-quarter of the patients exhibited high-level stigma resistance.7 Schulze and Angermeyer10 interviewed 25 German patients with schizophrenia and found that almost half of them (49%) experienced discrimination during social activities and exhibited perception of stigma. Chee et al11 studied 600 mentally ill patients at specialty and comprehensive hospitals in Singapore, finding that almost half (48.6%) of them felt that others looked down upon them; slightly more than one-third (37.1%) felt discriminated against in looking for jobs; and more than half (59.2%) of the patients believed that others would avoid them upon learning of their condition.
There is little evidence available from the People’s Republic of China on internalized stigma and its risk factors. In the People’s Republic of China, schizophrenia outpatients account for more than 90% of the total schizophrenia population in the People’s Republic of China and constitute a particularly important group for study.12 Patients with higher levels of education may have better understanding of their own illness by participating in online support forums and reading articles about the traits of their illness, such as easy recurrence, the need for long-term medication, and prognosis, which may, however, also add to the perception of stigma, while patients with lower levels of education lack such knowledge. A recent hospital-based study of 441 patients with mental illness in the People’s Republic of China showed that stigma or lack of knowledge may hamper treatment of the mental illness.13 We hypothesized that the education level of schizophrenic patients may impact on the perception of internalized stigma. In our cross-sectional study, we sought to assess the extent of internalized stigma among inpatients and outpatients with schizophrenia and to investigate whether education level correlated with the experience of stigma.
Patients and methods
Patients
We carried out a cross-sectional study of inpatient and outpatient schizophrenia patients who sought medical treatment at Tongde Hospital of Zhejiang Province, People’s Republic of China between January 2010 and January 2013. Subjects were screened for eligibility by review of the medical records of patients attending regular follow-up appointments. A patient was eligible for inclusion if: 1) he or she was aged between 20 and 70 years of age; 2) he or she met the diagnostic criteria for schizophrenia according to the International Classification of Diseases (ICD-10);14 3) he or she have achieved remission after therapy with antipsychotic agents;15 4) he or she had no concurrent severe systemic diseases; and 5) there was no apparent abnormality in routine blood and urine chemistries, liver function, or electrocardiogram. Individuals with clinically established impairment of insight, significant cognitive impairment, or substance abuse in the previous 3 months were excluded. The study protocol was approved by the local institutional review boards and all study participants or their legal surrogates provided informed consent.
Patient evaluation
Patients were assessed for eligibility at a screening visit, with eligible patients returning for a baseline assessment after approximately 1 week, and then evaluated at subsequent follow-up visits. Patients were evaluated using the Brief Psychosis Rating Scale (BPRS), the Positive and Negative Syndrome Scale (PANSS), the Clinical Global Impression-Severity (CGI-S) scale (1 point: very much improved; 7 points: very much worse) and the Stigma Scale for Mental Illness (SSMI-C).16–19 The 27-item SSMI-C is reported to have excellent internal consistency, with an alpha of 0.91 and a test–retest correlation of 0.90.20 All three clinicians evaluating the patients were trained in using the SSMI-C scale with a kappa value of 0.91 for this study. The SSMI-C has three domains: domain I is the discrimination domain, containing 12 items, which evaluates the degree of discrimination against the subjects due to the illness; domain II is the disclosure domain, containing nine items, which evaluates the degree of disclosure by the subjects; and domain III is the positive aspects domain, containing six items, which evaluates the intensity of perception of the disease by patients. The term “mental illness” was used throughout the questionnaire, but respondents were encouraged to “think of it as whatever you feel is the best term for it.”18 Each item was rated on a 4-point Likert scale ranging from 1= strongly disagree to 4= strongly agree, with higher scores indicating higher internalized stigma. Evaluation was carried out by two senior psychiatrists and mean scores were reported.
All patients were evaluated by mental illness specialists who had been specifically trained in ICD-10 with a kappa value of 0.85 for this study.
Safety
Vital signs and adverse events were monitored at baseline and post-drug therapy using the Treatment Emergent Symptom Scale (TESS).21 Safety assessments were based mainly on the occurrence, frequency, and severity of adverse events, and were also based on comprehensive indexes, including physical examination, electrocardiography, and routine laboratory investigations. For all adverse events, patients were withdrawn from the study where necessary.
Statistical analysis
All results were expressed as mean ± standard deviation and analyzed using SPSS software (v 15.0; IBM Corporation, Armonk, NY, USA). Student’s t-test was used to compare BPRS, PANSS, TESS, and CGI-S scores between two groups. Chi-square test was used to compare differences in SSMI-C scores and demographics. P<0.05 was considered statistically significant.
Results
Demographic and disease characteristics of the study subjects
Two hundred thirty-seven subjects were screened and 133 subjects were eligible for the study. Demographic and baseline characteristics of the study participants are shown in Table 1. The mean age of the study subjects was 32.05±8.95 (range: 20 to 57) years, and there were slightly fewer female (43.9%) than male patients (54.1%). Their mean course of illness was 4.32±6.14 years (range: 1 month to 15 years). Their mean BPRS score was 19.87±5.46, their mean PANSS score was 44.11±13.1, and their mean CGI-S score was 2.22±0.81. In addition, their mean SSMI-C score was 6.49±0.9.
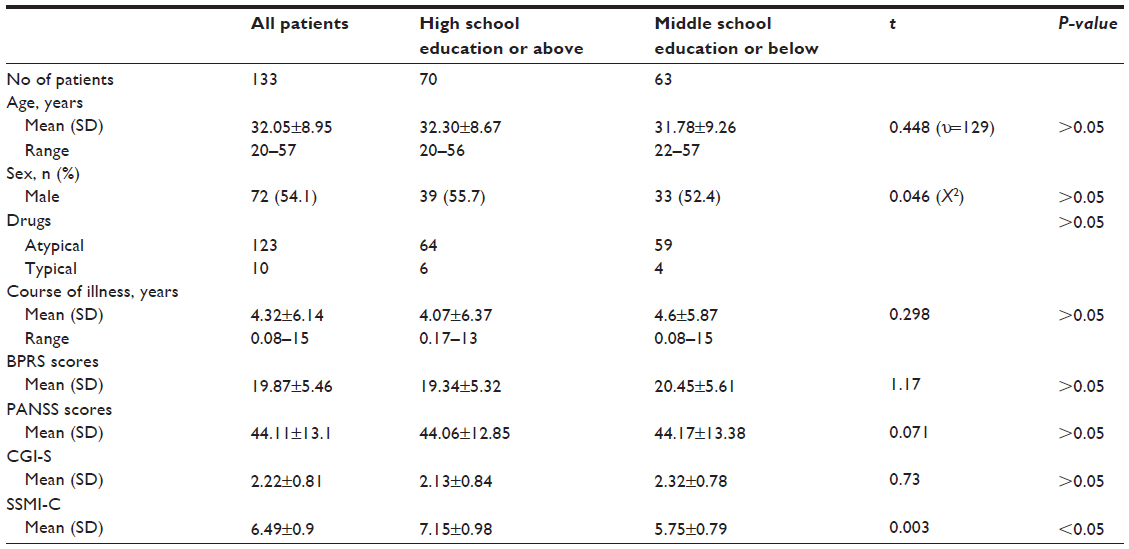 | Table 1 Demographic and baseline characteristics of the study subjects (Mean ± SD) |
We further analyzed the clinical records of patients according to levels of education. Patients who have received high school education or above and those who have received lower levels of education were comparable in demographic characteristics. They also had comparable BPRS scores (high school or above, 19.34±5.32 versus middle school or below, 20.45±5.61; P>0.05), PANSS scores (high school or above, 44.06±12.85 versus middle school or below, 44.17±13.38; P>0.05), and CGI scores (high school or above, 2.13±0.84 versus middle school or below, 2.32±0.78; P>0.05) (Table 1).
Education and internalized stigma
The mean SSMI-C score of patients who have received high school education or above was 7.15±0.98, which was markedly higher than that of patients who had received middle school education or below (5.75±0.79; P<0.05). The mean domain I score of patients who had received high school education or above was 2.30±0.76, which was comparable to that of patients who had received middle school education or below (2.07±0.78; P>0.05). The mean domain II score of patients who had received high school education or above was 2.42±0.96, which was markedly higher than that of patients who had received middle school education or below (2.01±0.79; P<0.05). Moreover, the mean domain III score of patients who had received high school education or above was 2.43±0.79, which was significantly higher than that of patients who had received middle school education (Table 2) (1.67±0.77; P<0.05).
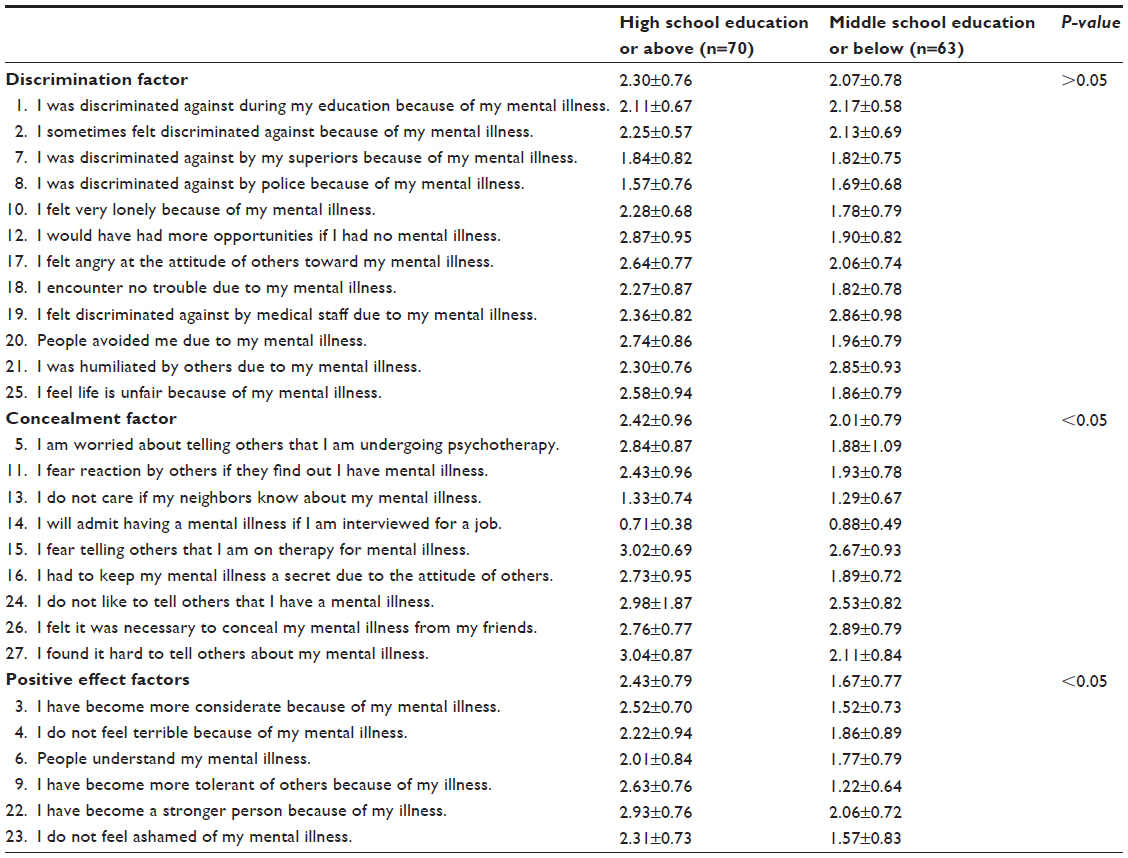 | Table 2 The Stigma Scale for Mental Illness (SSMI-C) score stratified by education |
TESS scores
Before the study most patients (92.5%, 123/133) took atypical drugs. The mean baseline TESS score was not clearly different compared to the mean post-therapy TESS score (P>0.05). Common side effects are listed in Table 3. There was no statistical difference in the frequency of side effects between patients who had received high school education or above and those who had received middle school education or below (P>0.05).
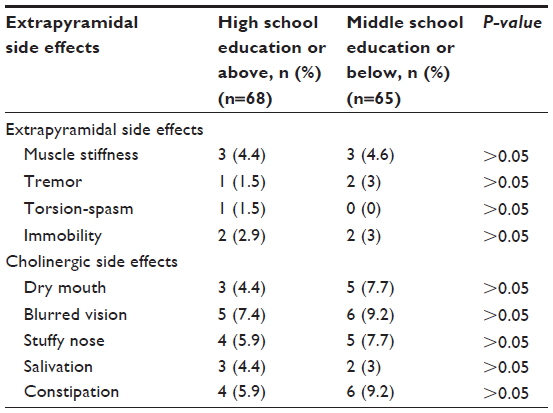 | Table 3 Side effects in the study participants |
Discussion
Internalized stigma leads to self-devaluation, shame, and social withdrawal, rendering it difficult to overcome barriers in establishing relationships and seeking employment, seriously hindering the recovery process. It is important to help patients cope with internalized stigma and to build up individual resistance in order to improve their well-being. The first step toward this goal is an understanding of internalized stigma in schizophrenia patients; however, there is scant data on the presence of stigma in Chinese schizophrenia patients. In the current study, we surveyed the presence of stigma in Chinese inpatients and outpatients with schizophrenia and found that internalized stigma was pervasive in our study subjects. We further found that educational level was an important factor in perception of stigma by schizophrenia patients: those who had high school education or above exhibited markedly higher SSMI-C scores than those with middle school education or below.
With advances in the treatment of schizophrenia, psychiatrists increasingly pay attention to the management of mental health of psychiatric patients. It is well established that discrimination and stigma pose a great barrier to the recovery of schizophrenia patients,22 and stigma of schizophrenia patients impacts on patient behavior in seeking medical therapy as well as adherence to therapy.7 It has previously been shown that stigma is pervasive in schizophrenia patients during convalescence,5 and that internalized stigma differs among urban and rural schizophrenia patients. Herein, we have shown that education level also contributes to differences in internalized stigma in schizophrenia patients, suggesting that proper interventions should be undertaken to tackle internalized stigma of schizophrenia patients, which will aid the planning of recovery programs for schizophrenia patients and improvement of treatment for schizophrenia patients.
We found no marked difference in demographics, BPRS scores, PANSS scores, CGI scale scores, and TESS scores among patients with different education backgrounds during convalescence. The side effects were mild and less frequent in our patients, which may be related to our use of atypical antipsychotic drugs with a benign safety profile, thus avoiding aggravation of internalized stigma of schizophrenia patients due to side effects of antipsychotic drugs.23 We used the SSMI-C to determine internalized stigma of schizophrenia patients with different education backgrounds. We found no significant difference in discrimination domain scores among patients with different education backgrounds, suggesting that, regardless of education background, schizophrenia patients are reluctant to reveal their mental illness to others. These patients all experienced discrimination or humiliation in life and felt that life was not fair, indicating development of intense stigma resistance in these patients. Furthermore, schizophrenia patients of different education backgrounds exhibited marked differences in concealment domain scores. Those who had received high school education or above were more likely to conceal their illness from others than those who had received lower levels of education. They were also less likely to disclose to others that they were on psychotherapy or anti-psychotherapeutic drugs. In addition, they were more sensitive to the attitudes of others. On the other hand, patients who had received high school education or above were more likely to receive psychological counseling than anti-psychotherapeutic drugs and were more tolerant of others. Patients who had received middle school education or below did not appropriately face their illness and were more likely to be pessimistic about their illness, indicating that it is important to educate these patients who received middle school education or above about mental health. Furthermore, patients who had received high school education or above had markedly higher scores in positive affect domain scores than those who had received lower levels of education. The former were more receptive to others and were more independent compared to patients who had received middle school education or below. Because of the pervasive nature of stigma in schizophrenia patients,5 apart from active drug therapy for preventing recovery, psychological education and aggressive psychological intervention are important in reducing the stigma of schizophrenia patients.24,25 As patients with different education backgrounds differ in stigma traits, psychological intervention should be individualized. Patients who have received high school education or above should be assisted in their early return to society and assumption of their work and family roles. Patients who receive middle school education or less should be helped with restoration of self-confidence and provided with mental health education.
The current study is limited by its cross-sectional nature and the size of the study cohort. In addition, this is a single-center experience, with most patients coming from within the same Chinese province. Furthermore, the findings from the current study need to be confirmed by a prospective multicenter study involving a larger patient population with a longer follow-up period.
Acknowledgments
This study was supported by the Zhejiang Province Key Science and Technology Innovation project (2012R10049-07) and the Zhejiang Province medical scientific research fund project (2012KYA039).
Disclosure
The authors report no conflicts of interest in this work.
References
Angermeyer MC, Matschinger H. Public beliefs about schizophrenia and depression: similarities and differences. Soc Psychiatry Psychiatr Epidemiol. 2003;38(9):526–534. | |
Brohan E, Slade M, Clement S, Thornicroft G. Experiences of mental illness stigma, prejudice and discrimination: a review of measures. BMC Health Serv Res. 2010;10:80. | |
Chen Y, Yue Y, Song LS. Investigation and related factors analysis of psychiatric patients’ families stigma. Shanghai Archives of Psychiatry. 2000;12(3):153–156. Chinese. | |
Gao SY, Fei LP, Wang XQ, et al. Discrimination in schizophrenia patients and their families. Chinese Mental Health J. 2005;19(2):82–85. Chinese. | |
Huang PR. Introduction to the improvement of the mental health service system – analysis focus on long-term hospitalized psychiatric patients present. Chin Med Eth. 2009;22(3):72–76. Chinese. | |
Phillips MR, Pearson V, Li F, Xu M, Yang L. Stigma and expressed emotion: a study of people with schizophrenia and their family members in China. Br J Psychiatry. 2002;181:488–493. | |
Ritsher JB, Phelan JC. Internalized stigma predicts erosion of morale among psychiatric outpatients. Psychiatry Res. 2004;30(129):257–265. | |
Sartorius N. Stigma: what can psychiatrists do about it? The Lancet. 1998;352(9133):1058–1059. | |
Prince PN, Prince CR. Perceived stigma and community integration among clients of assertive community treatment. Psychiatr Rehabil J. 2002;25(4):323–331. | |
Schulze B, Angermeyer MC. Subjective experiences of stigma: a focus group study of schizophrenic patients, their relatives and mental health professionals. Soc Sci Med. 2003;(56):299–312. | |
Chee CY, Ng TP, Kua EH. Comparing the stigma of mental illness in a general hospital with a state mental hospital. Soc Psychiatry Psychiatr Epidemiol. 2005;40:648–653. | |
Xiang YT, Weng YZ, Leung CM, Tang WK, Ungvari GS. Subjective quality of life in outpatients with schizophrenia in Hong Kong and Beijing: relationship to socio-demographic and clinical factors. Qual Life Res. 2008;17(1):27–36. | |
Zhang W, Li X, Lin Y, et al. Pathways to psychiatric care in urban north China: a general hospital based study. Int J Ment Health Syst. 2013;7(1):22. | |
The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research. World Health Organization; 1993. Available from: http://www.who.int/substance_abuse/terminology/icd_10/en/. Accessed November 14, 2013. | |
Huang N, Lu Z. Clinical application of the standard for alleviating schizophrenia. Shanghai Archives of Psychiatry. 2010;22(3):316–318. | |
Overall JE, Gorham DR.The brief psychiatric rating scale. Psychological reports. 1962;10(3):799–812. | |
Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophrenia bulletin. 1987;13(2):261–276. | |
Guy W, editor. Clinical global impression scale. ECDEU Assessment Manual for Psychopharmacology. 1976. Rockville, MD, U.S. Department of Health, Education, and Welfare. | |
Fung KM, Tsang HW, Corrigan PW, Lam CS, Cheung WM. Measuring self-stigma of mental illness in China and its implications for recovery. Int J Soc Psychiatry. 2007;53(5):408–418. | |
Geng F, Dong Y, Michael K, Liu HZ. Reliability and validity of the Chinese-version of Stigma Scale for Mental Illness. Chin Mental Health J. 2010;24(5):343–346. | |
Zhang MY. The Treatment Emergent Symptom Scale (TESS). Shanghai Archives of Psychiatry. 1990;2(63):1999. | |
Brohan E, Elgie R, Sartorius N, Thornicroft G; GAMIAN-Europe Study Group. Self-stigma, empowerment and perceived discrimination among people with schizophrenia in 14 European countries: the GAMIAN-Europe study. Schizophr Res. 2010;122(1–3):232–238. | |
Freudenreich O, Catcher C, Evins AE, Henderson DC, Goff DC. Attitudes of schizophrenia outpatients toward psychiatric medications: relationship to clinical variable and insight. J Clin Psychiatry. 2004;65(10):1372–1376. | |
[No authors listed]. Reducing the stigma of mental illness. Lancet. 2001;357(9262):1055. | |
Levav I, Rutz W. The World Health Report 2001. New Understanding, New Hope. Geneva: World Health Organization; 2001. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.