")
Back to Journals » Clinical Ophthalmology » Volume 8
A 6-year-old girl with ectopic cilia and hypochromic nevus
Authors da Fonseca F, Yamanaka PK, Lima P, Matayoshi S
Received 1 March 2014
Accepted for publication 16 April 2014
Published 2 July 2014 Volume 2014:8 Pages 1259—1261
DOI https://doi.org/10.2147/OPTH.S63313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Fabricio L da Fonseca,1 Patricia K Yamanaka,1 Patricia P Lima,2 Suzana Matayoshi1
1Department of Ophthalmology, 2Department of Pathology, University of São Paulo Medical School, São Paulo, Brazil
Abstract: Ectopic cilia are rare in humans. We report a 6-year-old girl with typical characteristics of ectopic cilia as described in the rare cases reported in the literature, in association with cutaneous lesions that appeared to be hypochromic nevi. This framework could be a different clinical presentation of ectopic cilia.
Keywords: ectopic cilia, cutaneous lesions, hypochromic nevus
Introduction
Ectopic cilia are very rare in humans. They are a congenital disturbance of the position of the eyelashes, which are usually on the lateral quadrant of the upper eyelid or conjunctival surface of the eyelid. The origin of these abnormally placed cilia is not clear, but a previous theory of meibomian gland substitution has been refuted and an embryologic origin suggested.1,2 In most cases, it causes no apparent medical morbidity and there is no positive family history. Treatment is surgical excision, mostly for cosmetic reasons. Here we report a case of a patient with ectopic cilia and hypochromic patches on the right arm.
Case report
A 6-year-old girl was referred for evaluation of a congenital lateral upper eyelid ectopic cilia cluster (Figure 1). On physical examination, she had hypochromic lesions on the right arm, diagnosed by the dermatology service as hypochromic nevi (Figure 1). The specimen comprised a circular 10×6 mm portion of skin and contained a centrally placed tuft of strong and pigmented hairs. Longitudinal sections and histologic analysis showed dermal and subcutaneous pilosebaceous follicles (Figure 1A and 1B), packed in a dense fibrous tissue core (Figure 1B) extending through the eyelid from the subcutaneous area, scarcely represented in the specimen. The epidermal surface showed pores of hair follicle infundibula (Figure 1B). Well developed sebaceous lobules (Figure 1C), bulbs of pilous follicles (Figure 1D), and apocrine-lined epithelial ducts consistent with glands of Moll (Figure 1E) and associated with pilous follicles were observed. Occasional striated orbicularis muscle fibers were present in the depths of the specimen (Figure 1F), with the lowest hair bulbs (Figure 1F) superficial to them. No tarsus, meibomian gland, or lacrimal gland ducts or acini were identified.
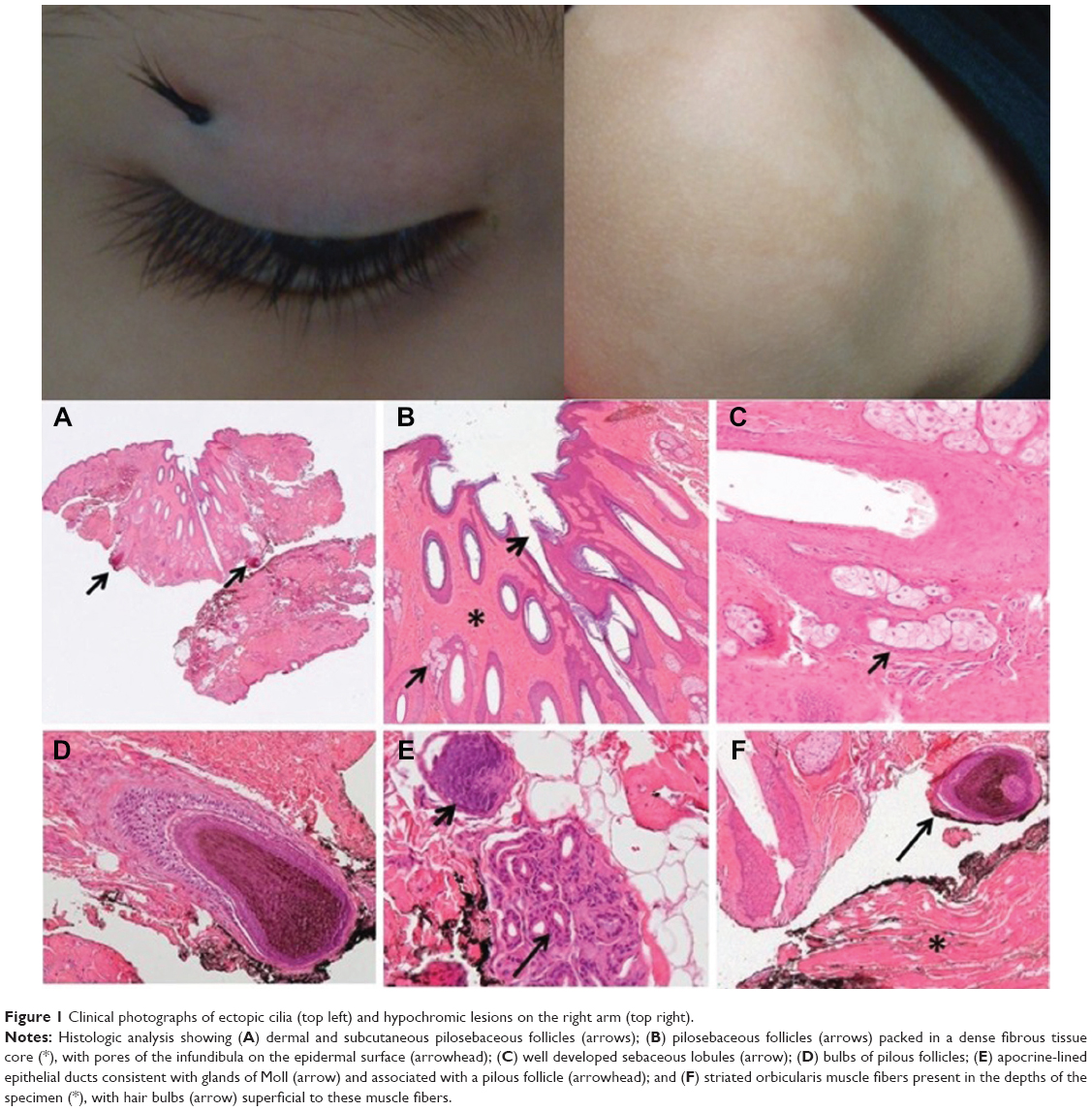 | Figure 1 Clinical photographs of ectopic cilia (top left) and hypochromic lesions on the right arm (top right). |
Discussion
Congenital ectopic cilia of the eyelid skin are rare. They have been observed to protrude from the anterior surface of the eyelid skin and the posterior aspect of the tarsal plate. There are 15 cases located on the anterior surface of the eyelids.1,2 Histologic examination has demonstrated the presence of apocrine and pilosebaceous glands, and there is evidence that ectopic cilia in the palpebral conjunctiva are acquired aberrant cilia, in contrast with anterior ectopic cilia, which are congenital.3
In this case, histopathologic examination of the specimen revealed the typical characteristics of ectopic cilia described in the rare cases reported in the literature. We found strong and pigmented hairs in a dense fibrous stroma associated with sebaceous and apocrine glands located in the dermis and subcutis and superficial to the orbicular muscle fibers. Importantly, ectopic cilia must be differentiated from abnormally placed hairs. As in our present case, the diagnosis of ectopic cilia is confirmed histologically by identification of sweat glands of the apocrine type attached to the follicles.4 Recent reports also underscore the importance of morphologic observation of ectopic cilia in association with lobules of sebaceous glands and apocrine glands.5 In the present case, the cilia arose from the anterior surface of the tarsal plate, being classified as anterior-type ectopic cilia, which are congenital, in contrast with posterior ectopic cilia that arise in the palpebral conjunctiva and are acquired aberrant cilia.3
Although previous reports have not correlated ectopic cilia with other skin hypopigmentation disorders, it is important to note that congenital hypochromic patches (hypochromic nevi) were observed in this case.
Disclosure
The authors report no conflicts of interest in this work.
References
Nakra T, Blaydon SM, Durairaj VD, Shinder R. Congenital upper eyelid ectopic cilia. J Pediatr Ophthalmol Strabismus. 2011;15:48. | ||
Chen TS, Mathes EF, Gilliam AE. “Ectopic eyelashes” (ectopic cilia) in a 2-year-old girl: brief report and discussion of possible embryologic origin. Pediatr Dermatol. 2007;24:433–435. | ||
Hase K, Kase S, Noda M, Ohashi T, Shinkuma S, Ishida S. Ectopic cilia: a histopathological study. Case Rep Dermatol. 2012;4:37–40. | ||
Dalgleish R. Ectopic cilia. Br J Ophthalmol. 1966;50:592–594. | ||
Jakobiec FA, Yoon MK. Histopathologic proof for the origin of ectopic cilia of the eyelid skin. Graefes Arch Clin Exp Ophthalmol. 2013;251:985–988. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.